
Abstract
Introduction
Bullying is a widespread problem in healthcare organizations, resulting in nurses’ poor mental health. Effective leadership, such as authentic leadership, may help to overcome this problem.
Objective
To examine the relationship between authentic leadership, workplace bullying, and nurses’ mental health, controlling for demographic characteristics.
Methods
A descriptive correlational design was utilized with a sample of 170 nurses. Nurses were recruited from four private hospitals in Jordan and completed a survey about their perception of managers’ authentic leadership, their experience of workplace bullying, and their mental health.
Results
About 48.8%, 25.9%, and 25.3% were categorized as “not bullied,” “occasionally bullied,” and “severely bullied,” respectively. Participant nurses had mild depression (m = 12.11) and moderate anxiety (m = 10.92). Workplace bullying was higher among nurses who earn less than 600 Jordanian dinars and nurses working in the smallest hospital, with 130 beds. Authentic leadership explains 6% of the variance of workplace bullying, 3% of anxiety, 7% of stress, and 7% of depression above and beyond the variance explained by other variables.
Conclusions
Healthcare organizations are facing a challenge in providing a healthy work environment. Employing authentic leadership in the workplace could be one of the factors that could help in addressing this issue.
Introduction
The healthcare system is facing many challenges like nurse shortage, workplace bullying, increasing rates of infectious and new diseases, an increase in the aging population, the limitation of budgets, and a stressful work environment (Catton, 2020; Rayan, 2019). Effective leaders have the skills and qualifications to face these challenges and provide the best solutions. In addition, effective leaders are capable of achieving the organization's goals while improving staff and patient satisfaction (Alilyyania et al., 2018). One of the leadership styles that has been under study over the past few years is authentic leadership. Authentic leadership showed positive results in improving the work environment and increasing patient and nurse satisfaction and well-being (Alilyyania et al., 2018). The current study examines the role of employing the authentic leadership style by nurse leaders to address two of the most significant challenges that face nurse leaders, including workplace bullying and nurses’ poor mental health.
Literature Review
Authentic leadership is described as a type of leadership that focuses on positive psychological capacities and an ethical climate. It encourages greater self-awareness, an internalized moral perspective, balanced processing of information, relational transparency on the part of leaders, and positive self-development (Walumbwa et al., 2008). Nursing and authentic leadership are a big match since they depend largely on human values that are the core of nursing (Alilyyania et al., 2018). Although the concept of authentic leadership is relatively new, there have been numerous empirical studies connecting authentic leadership to work behaviors and work outcomes (Labrague et al., 2021; Ribeiro et al., 2018: Semedo et al., 2016).
Workplace bullying is a major problem in healthcare organizations, which has been highlighted by many studies worldwide (Lever et al., 2019). Nurse bullying is defined as “frequent, undesired, hurtful actions performed to cause distress and shame to the nurse” (American Nurse Association (ANA), 2015). The impact of workplace bullying on nurses and organizations is enormous. It could aggravate burnout in nurses, which leads to an increase in the intention to leave the organization and turnover (Kim et al., 2019). Also, workplace bullying causes psychological distress, burnout, depression in the victims of bullying, and physical symptoms like insomnia and headache (Harb et al., 2021; Lever et al., 2019). In Jordan, a study about workplace bullying among nurses working at private hospitals showed that 43% of participant nurses viewed themselves as severe workplace bullying victims and 31% as occasional workplace victims of bullying (Obeidat et al., 2018).
Nurses’ mental health should be a concern of nurse administrators because nurses are exposed to mental health problems such as anxiety and depression more than other professionals (Perry et al., 2015; Ta’an et al., 2020). Nurses are under tremendous stress due to many factors, including but not limited to the high workload, the administration, and the conflicts with doctors, patients, and relatives (Al-Ghabeesh et al., 2022; Happell et al., 2013; Rayan & Baker, 2019).
Previous research found that authentic leadership has a positive impact on creating structural empowerment, which in turn fosters nurses’ mental health (Read & Laschinger, 2015; Saleh et al., 2022). Research also found a negative relationship between adopting authentic leadership and exposure to workplace bullying (Warszewska-Makuch et al., 2015).
Workplace bullying and nurses’ poor mental health are two factors that have negative effects on nurses and healthcare organizations. Jordan is similar to other countries where workplace bullying against nurses is a major concern in healthcare organizations (Al-Ghabeesh & Qattom, 2019). To date, limited knowledge is available regarding the role of leadership styles in reducing bullying and improving nurses’ mental health. Authentic leadership is a model that has been associated with positive outcomes, but its role in reducing workplace bullying and improving nurses’ mental health has yet to be established. Literature review revealed that demographic variables such as gender, income, work settings, marital status, educational status, years of experience, employment status, and working patterns could impact workplace bullying and nurses’ mental health (Al-Ghabeesh & Qattom, 2019; Badu et al., 2020; Cheung & Yip., 2015; Khodadadi et al., 2016; Maharaj et al., 2018; Turan & Ancel, 2020; Vahedian-Azemi et al., 2020). Therefore, controlling their impact is needed when investigating factors associated with workplace bullying and nurses’ mental health.
Purpose
This study aimed to examine the relationship between authentic leadership, workplace bullying, and nurses’ mental health, controlling for demographic characteristics. The study has the following questions:
What are the scores of authentic leadership as reported by registered nurses? What are the levels of mental health problems (depression, anxiety, and stress) as reported by registered nurses? What is the prevalence of bullying as reported by registered nurses? Are there any differences in the scores of mental health problems (anxiety, depression, and stress), workplace bullying, and authentic leadership based on nurses’ demographics? Can authentic leadership predict workplace bullying, depression, anxiety, and stress, controlling for demographic characteristics?
Methods
Design
A descriptive correlational design was utilized to measure Jordanian nurses’ perceptions of authentic leadership, workplace bullying, and mental health. The study was descriptive as it described authentic leadership, workplace bullying, and mental health problems (depression, anxiety, and stress) as reported by registered nurses. It also was correlational as it aimed to explore the relationships between the main study variables, controlling for demographic characteristics.
Sample
The target population was all Jordanian registered nurses. The accessible population was nurses working in private hospitals in Amman, Jordan. Data were collected from four private hospitals located in Amman. The private sector was chosen because most of the previous studies on workplace bullying and nurses’ mental health were conducted in the public sector (Abu-Horirrah et al., 2022; Al-Shiyab & Ababneh, 2018; Ghareeb et al., 2021). The selected hospitals include hospitals that provide general care and different services, including medical, surgical, pediatric, maternal, critical, and emergency care. Hospital 1 has around 130 beds. A total of 83 nurses work in this hospital. Hospital 2 is a nonprofit training educational medical institution with around 200 nurses. In this hospital, there are 273 beds. The third contains 200 beds, and around 300 nurses are working at this hospital. The last hospital is a modern, multispecialty hospital with 200 beds and 280 nurses.
Recruitment was done using a convenience sampling technique. Using G*power for regression analysis, the minimum required sample size to achieve 80% power, with a medium effect size (0.15), an alpha of .05, and 13 possible predictors, is 131 participants. The sample size was increased to 170 to address the possibility of having substantial missing data. A total of 205 participants were invited to participate in the study. A total of 170 completed questionnaires were returned (the response rate was 83%).
Inclusion/Exclusion Criteria
Participants were recruited according to the following eligibility criteria: (1) being Jordanian, (2) having a bachelor's degree or a higher academic degree in nursing, (3) having at least 1 year of nursing work experience, and (4) having worked at bedside. Exclusion criteria included nurses with a history of mental health problems and nurses with administrative positions.
Data Collection
After getting the required approvals, the researchers accessed the hospitals and met the potential participant nurses and explained the purpose of the study and its procedure. Data were collected using an electronic self-reported questionnaire constructed on Google Forms. Nurse managers facilitated the data collection by helping identify the eligible participants and sending the electronic questionnaire through WhatsApp and e-mails randomly. The researcher's e-mail and telephone number were shared with all participants in case of having questions or concerns.
Measurements
Demographic Data
Information about demographic data included the following: gender, age, marital status, level of education, hospital, working area, monthly income, years of experience in nursing, years of experience in the current hospital, years of experience in the current department, employment status, working patterns, and nurse-to-patient ratio.
Authentic Leadership Questionnaire
Perception of managers’ authentic leadership was measured using the “Authentic Leadership Scale” (ALS), which was developed by Walumbwa et al. (2008). This instrument was used to measure authentic leadership in the leaders as perceived by their subordinates. The instrument consists of 16 items that address four subscales: relational transparency (5 items) that is related to how the leaders present a true and genuine self; internalized moral perspective (4 items) that reflects self-regulations and morals; balanced processing (3 items) that reflects how the leaders objectively consider alternative views; and self-awareness (4 items) that addresses the leaders’ interpretation of the world and their strengths and weakness. Each of these items is rated on a 5-point Likert-type scale ranging from 0 to 4 (0: not at all; 4: frequently if not always). There are no cutoff scores for the Authentic Leadership Questionnaire (ALQ), but the higher the score, the more frequently the leader performed authentic leadership skills. The ALQ is a reliable and valid tool. It showed high internal consistency reliability; Cronbach's alpha for the entire scale was 0.91 (Walumbwa et al., 2008).
Permission to use the Arabic translated version of the ALS was obtained from the scale publisher (Mind Garden).
Depression Anxiety Stress Scales
This instrument was used to measure the three related negative emotional states of depression, anxiety, and stress. It consists of 42 items (Lovibond & Lovibond, 1995). The frequency or severity of the participants’ experience over the last week was rated on a 4-point Likert-type scale that ranges from 0 to 3 (0: did not apply to me at all; 3: applied to me very much or most of the time). Each emotional state consists of 14 items, with a total score ranging from 0 to 42. Regarding depression, the cutoff point is as follows: 0–9 (normal), 10–13 (mild), 14–20 (moderate), 21–27 (severe), and 28–42 (extremely severe). Regarding anxiety, the cutoff point is as follows: 0–7 (normal), 8–9 (mild), 10–14 (moderate), 15–19 (severe), and 20–42 (extremely severe). Regarding stress, the cutoff point is as follows: 0–14 (normal), 15–18 (mild), 19–25 (moderate), 26–33 (severe), and 34–42 (extremely severe). The Arabic version of Depression Anxiety Stress Scales (DASS), which is a valid and reliable tool, was used. Cronbach's alpha is adequate for the depression, anxiety, and stress subscales (0.91, 0.84, and 0.90, respectively). The Arabic version reliability coefficients for the three scales were depression .93, anxiety .90, and stress .93 (Moussa et al., 2016).
Negative Acts Questionnaire-Revised
This instrument was used to measure exposure to workplace bullying. It consists of 22 items and has three factors: personal bullying (7 items), work-related bullying (12 items), and physically intimidating bullying (3 items). Each item is rated on a 5-point Likert-type scale ranging from 1 to 5 (1: never; 5: daily). The total score range from 22 to 110. Higher scores indicate higher degrees of bullying. Participants with scores of <33 are considered “not being bullied,” 33–45 were “occasionally bullied,” and <45 were “severely bullied” (Einarsen et al., 2009). The Arabic version was used and revealed acceptable levels of reliability and validity. Reliability coefficients for the total and subscale scores of the Negative Acts Questionnaire-Revised (NAQ-R) ranged from .63 to .90 (Makarem et al., 2018).
Ethical Considerations
Approvals were obtained from the Institutional Review Board (IRB) at the school where the researchers are working and from each selected hospital. Permission to use the ALQ was obtained from Mind Garden Institute. After getting access to the potential participants, the researcher informed them about the study's purpose, research process, and study protocol. Participants were assured that they are free to participate without coercion and were reminded that they have the right to discontinue completing the questionnaire without being affected in any way and that their information would be confidential.
Statistical Analysis
Data analysis was performed using SPSS (version 26). Descriptive statistics were employed to describe sample characteristics and the scores of the main study variables using means, standard deviations (SDs), frequencies, and percentages. The t-test and one-way analysis of variance (ANOVA) were used to detect differences in the main study variables based on participants’ sociodemographics. Pearson’s correlation was used to examine the relationships among the main variables. Hierarchical multiple regression was used to identify the unique variance in workplace bullying, depression, anxiety, and stress that can be explained by authentic leadership.
Results
Sample Characteristics
A total of 170 nurses participated in the study. The mean age of participants was 30 years (SD ± 6.9). More than half of the participants were females (n = 99, 58.2%). In terms of marital status, 50% were married. The majority of the participants had a bachelor's degree (n = 146, 85.9%). The mean for years of experience was 7.8 years (SD ± 6.6). The mean length of being employed in the current hospital was 4.8 years (SD ± 5.5), while the mean of being employed in the current department/area of work was 3.9 years (SD ± 3.9). More than half of the participants reported receiving less than 600 Jordanian dinars (JD) per month (n = 111, 65.3%) (Table 1).
Sociodemographic and Professional Sample's Characteristics.
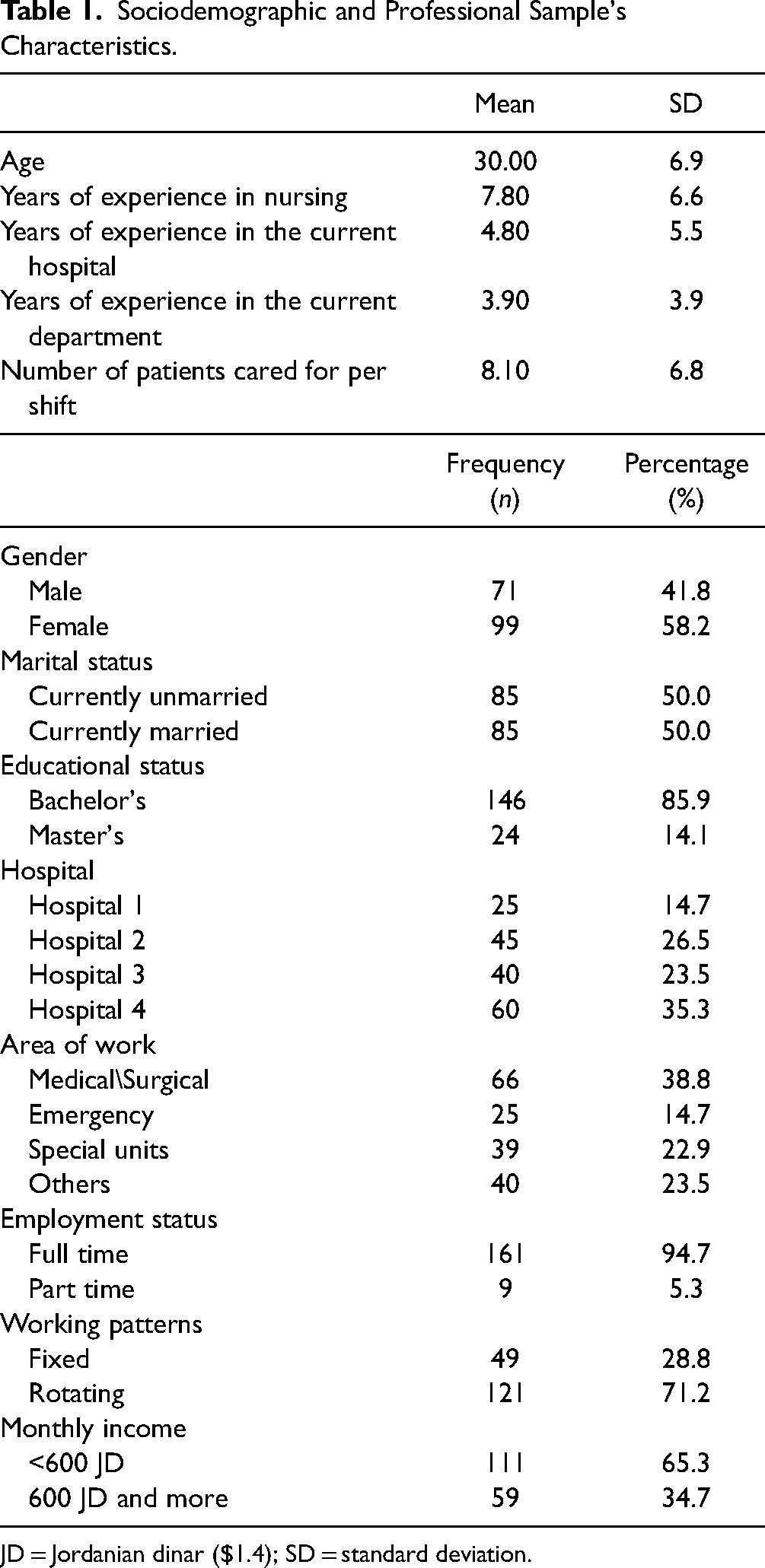
JD = Jordanian dinar ($1.4); SD = standard deviation.
Authentic Leadership, Depression, Anxiety, Stress, and Workplace Bullying
The overall mean score for authentic leadership was 2.22 (SD ± 0.96). In terms of the subscales, the highest mean scores were reported for morality/ethics (mean = 2.24, SD ± 0.97), followed by balanced processing (mean = 2.22, SD ± 1.11) and self-awareness (mean = 2.22, SD ± 1.01), and the lowest mean score was reported for transparency (mean = 2.20, SD ± 1.00) (Table 2). Participants demonstrated mild depression (12.11), moderate anxiety (10.92), and normal stress (13.69) (Table 3). About 48.8%, 25.9%, and 25.3% were categorized as “not bullied,” “occasionally bullied,” and “severely bullied” subsequently (Table 4).
Authentic Leadership Scores.

Depression, Anxiety, and Stress Levels.

Prevalence of Bullying at the Workplace.

Differences in Anxiety, Depression, Stress, Bullying, and Authentic Leadership Based on Sociodemographic Variables
Female nurses were found to have significantly higher stress and anxiety scores than male nurses. Results showed that nurses who earned less than 600 JD per month had significantly more experiences of workplace bullying compared to nurses who earned more than 600 JD per month. Post hoc analysis found that nurses who worked in Hospital 1 had significantly more frequent experiences of workplace bullying compared to nurses who worked in other hospitals. Results showed that nurses who had more workload had significantly higher scores of depression, anxiety, and stress. No significant differences exist in workplace bullying and depression, anxiety, and stress based on the following: age, marital status, educational status, employment status, working patterns, and area of work. In addition, workplace bullying and mental health were not associated with years of experience in nursing, years of experience in the current hospital, and years of experience in the current department. Finally, no significant results were found on the scores of authentic leadership based on sociodemographic characteristics (Table 5).
Differences in Anxiety, Depression, Stress, Bullying, and Authentic Leadership Based on Sociodemographic Characteristics.

M/S = medical/surgical; SD = standard deviation, * P< 0.05.
The Relationships Between Authentic Leadership and Workplace Bullying, Depression, Anxiety, and Stress, Controlling for Demographic Characteristics
Workplace bullying was correlated positively with depression (r = .615, P < .001), anxiety (r = .631, P < .001), and stress (r = .583, P < .001) and negatively with authentic leadership (r = −.230, P = .003). Depression, anxiety, stress, and workplace bullying correlated positively with each other and negatively with authentic leadership (Table 6).
Correlations Between Authentic Leadership, Bullying at the Workplace, Depression, Anxiety, and Stress.

ALQ = Authentic Leadership Questionnaire.
**Correlation is significant at the .01 level (two-tailed).
The hierarchical regression analysis was conducted to examine the unique relationship between authentic leadership and both workplace bullying and nurses’ mental health. Authentic leadership explained an additional 6% of the variance in workplace bullying above and beyond the 11% explained by monthly income and hospital. In addition, authentic leadership explained 7% of the variance in depression above and beyond the 4% explained by workload. Authentic leadership also explained 3% of the variance in anxiety above and beyond the 5% explained by gender and workload. Finally, authentic leadership explained 7% of the variance in stress above and beyond the 8% explained by gender and workload (Table 7).
Predictors of Bullying at the Workplace, Depression, Anxiety, and Stress Through Authentic Leadership.

ALQ = Authentic Leadership Questionnaire.
Discussion
The current study examined the relationships between authentic leadership, bullying behavior, and mental health among Jordanian nurses. Overall, participants reported a “sometimes” frequency of performing authentic leadership behaviors by their managers. In addition, the overall mean score of ALS in this study was around the midpoint of the scale. The scores of authentic leadership in this study were relatively higher than the scores reported in previous studies (Alkharabsheh & Alias, 2018; Mrayyan et al., 2022). This might suggest better recognition of the need to become true leaders and the impact of such leaders on organizational behavior and wider healthcare service outcomes. The highest score of the subscales was for the moral and ethical perspective, which refers to the degree of the commitment of the leaders to his/her high standards of ethics and morals, letting these standards guide their decisions (Walumbwa et al., 2008). This outcome is similar to another study, which revealed that the moral ethical subscale had the highest mean score (Warszewska-Makuch et al., 2015). This might be related to the Arabic–Islamic culture, which encourages this attitude (AlSarhi et al., 2014). The lowest score of the subscale was for transparency, which was supported by the studies of Mrayyan et al. (2022) and Labrague et al. (2021).
Nevertheless, it is not surprising that no significant results were found on the scores of authentic leadership based on sociodemographic characteristics. A systematic review of the literature found that authentic leadership was influenced by factors beyond the personal characteristics of nurses such as structural empowerment, burnout, trust, psychological capital, decisional involvement, work environment, work climate, team psychological safety, emotional exhaustion, job performance, work engagement, and organizational culture (Alilyyania et al., 2018).
About 25.9% and 25.3% of the participants were categorized as “occasionally bullied” and “severely bullied” subsequently. These results are lower when compared to recent studies by Al-Sagarat et al. (2018) and Obeidat et al. (2018), who reported moderate rates of bullying behavior experienced by Jordanian nurses. In this study, which targeted the private sector, the prevalence of bullying was lower than that in the studies done in Jordan. The lower rates might be explained by a possible increasing awareness of nurses about the unacceptability of bullying behavior in healthcare settings and patient satisfaction in the private sector.
Participants had mild depression and moderate anxiety. It is evident in the literature that depression can negatively affect the level of performance and job satisfaction of nurses (Jeong & Min, 2021). Therefore, while the level of depression is mild, early intervention is needed to prevent further worsening of depression.
Nurses who earn lower than 600 JD per month reported more experiences of being bullied than other participants. Many nurses with high income work in administrative positions and have less direct contact with patients and family members. On the contrary, nurses with low income usually work at bedside and have direct contact with patients and experience higher rates of violence. This supports the hypothesis that bullying behavior persists within the workplace as a function of the exercise of power (Taylor & Taylor, 2017).
Results also found a variation in bullying experience between hospitals. Bullying was higher among nurses working in the smallest hospital, with 130 beds. While this might seem self-incriminating, it is important to note that overall levels of bullying behavior are low. There should be an in-depth exploration of why bullying persists at all within these organizations and what can be done to eliminate bullying altogether. Evidence from the literature supports the implementation of a zero-tolerance policy to address this issue (American Association of Critical Care Nurses, 2019).
Female nurses were found to have higher levels of anxiety and stress compared to male nurses. The literature is inconsistent on this issue. For example, Khodadadi et al. (2016) found higher levels of stress, depression, and anxiety in female nurses compared to their male counterparties, while Cheung and Yip (2015) and Maharaj et al. (2018) found no gender differences in nurses’ mental health.
Consistent with previous research, and as expected, a higher workload resulted in higher levels of depression, anxiety, and stress among the participants (Badu et al., 2020; Turan & Ancel, 2020). The overwhelming volume of tasks that need to be completed contributes to workplace stress and negatively affects the psychological health and well-being of nurses (Vahedian-Azemi et al., 2020).
Results of the study showed that nurses who had more frequent experiences of being bullied had significantly higher levels of depression, anxiety, and stress and lower scores on authentic leadership. These results are consistent with the previous literature that highlights the negative psychological impact of bullying on nurses (Layne et al., 2019; Wilson, 2016). Lever et al. (2019) in a systematic review that involved 45 studies found that bullying can lead to worse mental health, higher rates of depression, higher reports of burnout, higher levels of psychological distress, worse anxiety, more suicidal ideation, higher rates of insomnia and sleep disturbances, and higher rates of sick leave.
This study showed that authentic leadership was associated with less workplace bullying. This outcome is in line with a study done in Ontario, which shows that authentic leadership could decrease bullying and burnout in the workplace (Laschinger et al., 2012). When leaders are open and transparent with the nurses and have high integrity when dealing with their followers, they will create behaviors of high standards in the workplace that mitigate bullying. Conversely, the lack of authentic leadership skills among the participants’ nursing leaders can have an adverse influence on several aspects of nurses’ health and well-being. In the same context, levels of depression, anxiety, and stress among nurses could increase when their leaders have low scores on authentic leadership (Nelson et al., 2014).
Strengths and Limitations
Although this study is one of the few studies that closely examined the relationships between authentic leadership, bullying behavior, depression, anxiety, and stress among nurses working within the Jordanian healthcare context, it has some limitations. First, using the cross-sectional design limits the ability to infer a cause–effect relationship. Second, the study was conducted using convenience sampling, which could limit the generalizability of findings. Third, the study was largely dependent on self-reported questionnaires. This can be remedied in future research by employing a mixed-method research design that enables researchers to conduct in-depth examinations and obtain more contextual information related to the link between the study variables.
Implications
The findings of this study support employing authentic leadership in the management process in the healthcare organization, which could improve nurses’ mental health. This could also enhance teamwork, performance, motivation, engagement, and patient care and discourage bullying behaviors. Holding workshops that shape the nurses’ skills in authentic leadership is crucial. Depression, anxiety, and stress are consequences of a poor work environment. Depressed, anxious, and stressed nurses are prone to committing mistakes and may unnecessarily compromise the health and safety of their patients and the wider public. Policies and guidelines should also be directed toward eliminating and preventing any bullying incidents and improving nurses’ mental health. Formulating policies and guidelines that enforce zero tolerance for any type of bullying behavior is required. Hospitals should have strategies in place to support nurses who report being depressed, anxious, and stressed. Professional psychological support should be available at the workplace to support nurses who have psychological disturbances.
Conclusions
Healthcare organizations are facing a challenge in providing a healthy work environment. More than half of the participant nurses were exposed to workplace bullying. Exposure to workplace bullying was associated with increased depression, anxiety, and stress among nurses. Authentic leadership could act as a protective factor against workplace bullying, anxiety, stress, and depression among nurses regardless of their demographic characteristics.
Footnotes
Consent
The study was undertaken with the understanding and written consent of each subject.
Data Availability
Data are available on request from the authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Considerations
Approvals were obtained from the Institutional Review Board (IRB) at the School where the researchers are working and from each selected hospital. Permission to use the ALQ was obtained from Mind Garden Institute.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.