
Abstract
Introduction
Vaccination against coronavirus disease (COVID-19) is a key factor in protecting vulnerable populations, reducing healthcare burdens, and mitigating the economic and social impacts of the pandemic.
Objective
This study aims to investigate Jordanian nurses’ perceptions, acceptance, and factors affecting their decisions toward the COVID-19 vaccines.
Methods
In this study, we conducted a cross-sectional design. Data have been investigated between July 1, 2021 and August 30, 2021. Nurses at three private hospitals in Jordan were surveyed online. The online survey, created using Google Forms, was distributed to nurses via email and social media sites (e.g., WhatsApp and Facebook). Participants were eligible if they were a RN nurse and/or nursing assistance, and had access to the internet via computer and/or smartphone.
Results
Out of 189 responses, 50.6% agreed to receive the COVID-19 vaccine, while 25.5% disagreed, and 23.9% were undecide to receive the vaccine. A large proportion (84.66%) of the respondents had a negative perception toward the vaccine, while only a small minority (15.34%) had a positive perception of it. The older nurses, those with more experience, and those with a higher level of education were more likely to accept the vaccine, with acceptance rates of 56.1%, 54.8%, and 63.9%, respectively.
Conclusion
Of the nurses surveyed, 84.66% had a negative perception of the COVID-19 vaccine, and only 50.6% reported that they would be willing to get vaccinated. It is crucial to address the concerns and reduce apprehension among nurses about the vaccine. Efforts to increase awareness about the importance of vaccination in controlling the disease through workshops and online meetings are needed.
Introduction
The first case of the novel coronavirus disease 2019 (COVID-19), which is brought on by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was found in Wuhan, Hubei province, China, in December 2019. Consequently, due to the infection's alarming rates of spread and severity, the World Health Organization (WHO) proclaimed COVID-19 a pandemic on March 11, 2020 (WHO, 2020). SARS-CoV-2 infection has been linked to a wide variety of illnesses, from asymptomatic to lethal, from mild to severe (Richardson et al., 2020). Fever, exhaustion, a dry cough, shortness of breath, pneumonia, anosmia, and ageusia are typical COVID-19 clinical signs (Guan et al., 2020; Richardson et al., 2020; Tong et al., 2020).
Nations around the world have implemented different control measures, such as social distancing, partial and comprehensive lockdowns, closing schools and businesses, and/or wearing face masks in public, to prevent the spread of SARS-CoV-2 infection and lessen its health effects. A return of COVID-19 has been recorded as societies and economies have reopened, despite the fact that such efforts have helped to flatten the epidemic curve (Devi, 2020; Shimizu et al., 2020). Long-term preventive actions are therefore urgently needed. Herd immunity, which is described as a degree of immunity in a community that prevents epidemics through natural infection, is something that few nations have attempted to accomplish. However, such a strategy has been regarded as unethical and impractical (Griffin, 2020; Orlowski and Goldsmith, 2020).
Review of Literature
Currently, coronaviruses are the leading cause of respiratory illness. Several single-stranded RNA viruses may produce anything from an ordinary cold to life-threatening symptoms (Cascella et al., 2022). There has been increasing worldwide concern about the coronavirus owing to its great transmission capacity, which may be linked to mortality and morbidity (Wang et al., 2021). Current prophylactic means are essential to rapidly inhibit the dramatic situation triggering high mortality rates (Kurtuluş and CAN, 2021). DNA and RNA, viral vector, inactivated, live attenuated viral, and recombinant protein vaccines are some of the methods being investigated to enhance SARS-CoV-2 immunizations. Influenza and other infectious diseases can be prevented through vaccinations (Liu et al., 2020). Healthcare professionals (HCPs) should be vaccinated against diseases that provide a larger risk of infection than the general population (Dini et al., 2018). Healthcare workers (HCWs) are given priority for early COVID-19 vaccination because they are at high risk for occupational SARS-CoV-2 exposure and transmission. As a result, it's critical to identify the extent of vaccine hesitancy among HCWs and state its underlying reasons in order to promote immunization and support efforts to stop the ongoing COVID-19 pandemic.
Vaccine efficacy, safety, and the conceivably rushed production process are the common barriers toward vaccination among HCWs. Vaccine communications present various challenges, which require understanding audiences to improve messages and help save lives. This concern is necessary because vaccine hesitancy in the US has been observed (Piltch-loeb and Diclemente, 2020). Even though immunization facilities are readily available, some people are still reluctant to be vaccinated (WHO, 2014). Public awareness is critical in the fight against the spread of highly contagious respiratory infections, especially in low- and middle-income countries where health services are only moderately equipped to deal with epidemics (Abdelhafiz et al., 2020). It is estimated that vaccine production will take months, and therefore the majority of management of the crisis is dependent on people adhering to the suggested procedures. These measurements are influenced mainly by the public's knowledge, attitude, and practices (Zhong et al., 2020). Learning from China's SARS outbreak in 2003 suggests that panic emotion is associated with how knowledgeable and attuned people are to infectious diseases among people, which can further confuse efforts to counteract the disease spread (Abdelhafiz et al., 2020). Such uncommon situations are made more difficult by underestimating, stigmatizing, panic emotions, false preventive measures, and stigmatization. (Zhong et al., 2020). A variation reported in vaccine acceptance ranged from as low as 27.7% in Congolese HCWs (Kabamba Nzaji et al., 2020) to as high as more than 95% in a study involving HCWs from the Asia Pacific region. Several studies have evaluated vaccine attitudes in HCWs prior to the vaccine's availability and uptake (Chew et al., 2021). Several Arab nations have reported more coronavirus infections and fatalities in recent months, bringing the totals from the start of the pandemic to around 4.5 million and 76 thousand, respectively, until mid-March 2021. Qunaibi et al. (2021) reported a high rate of vaccine hesitancy postvaccine availability in Arab countries; according to Qattan et al. (2021) in Saudi Arabia, about 25% of tested sample was expected to have the vaccine once available, while in Egypt (Hussein et al., 2021) cited 46% of HCWs somewhat/totally agreed to receive the vaccine. A cross-sectional study found that among 385 Egyptian HCWs, 51% were undecided about receiving COVID-19 vaccine, 28% refused, and 21% accepted vaccination. According to the study, the reasons for vaccine hesitancy were a lack of clinical trials and apprehension about the vaccine's side effects (Fares et al., 2021). Another study found that 70% of 5,237 Pakistani HCWs accepted COVID-19 vaccination, 24.5% wanted to wait until more data was available, and 5.2% refused to be vaccinated. The reasons for rejections were vaccine effectiveness and vaccine side effect (Malik, Malik, and Ishaq 2021). In addition, 76.9% of French HCWs would accept a COVID-19 vaccine. Nurses and assistant nurses were less likely to accept COVID-19 vaccination. Vaccine hesitancy was linked to lower COVID-19 vaccine acceptance (Gagneux-Brunon et al., 2021). Lack of information about the vaccine's side effects and a lack of knowledge about the vaccine itself were the two biggest hurdles to COVID-19 vaccination among Egyptian medical students (Saied et al., 2021). Greater vaccination acceptability was mostly associated with attitudes toward vaccination's benefits, perceived vaccine efficacy, social environment influence, patient protection, and medical professionals’ duties. Concerns about side effects and complications were the main reasons why nursing students refused vaccinations(Kregar Velikonja et al., 2021). Unfortunately, there is no previous study that evaluates the perception and acceptance of Jordanian nursing of COVID-19 vaccine, as nursing is part of the Jordanian society that is affected by myths and information transmitted about the vaccine. Therefore, an update of the status of vaccine hesitancy among HCWs in general, and among Arabic-speaking HCWs is highly required. This study will help to fill a knowledge gap about why some nurses refuse COVID-19 vaccination and what factors influence their perception and acceptance to be vaccinated, with the aim of investigating Jordanian nurses’ perceptions, acceptance, and factors affecting their decisions towards the COVID-19 vaccines.
Methods
Design
Cross-sectional design was used in this study to capture a snapshot of the perceptions and acceptance of the COVID-19 vaccine among nurses in Jordan at a specific point in time. The study aimed to provide an understanding of the current situation among nurses in Jordan regarding the COVID-19 vaccine acceptance and perception, rather than following them over a period of time. A cross-sectional design allowed the researchers to draw conclusions about the study sample at a specific point in time.
Data Collection and Setting
The study was conducted between July 1, 2021, and August 30, 2021. The online poll, which was created using Google Forms, was sent to a list of nurses via email and social media sites (e.g., Facebook and WhatsApp). The survey responses were collected anonymously. The sample for this study was obtained from three private hospitals in Amman, Jordan's capital city. Each hospital has an average 200 beds and 120 nursing staff members, including RN nurses and assistant nurses. These private hospitals accept patients with private insurance and some with government insurance. Nursing handles COVID-19 cases before the diagnosis is known, and once the diagnosis is confirmed, they are transferred to Ministry of Health hospitals for follow-up and admission if necessary.
Sample
Convenience sampling was used in this study due to the restrictions during the pandemic that limited the opportunity to reach the nurses and at the same time, the demands of the pandemic in the HCW preoccupied the nurses. However, convenience sampling can still provide valuable insights into the perceptions and acceptance of the COVID-19 vaccine among nurses. An online survey was sent to all nurses working at the selected hospital in Jordan. They received the online survey through emails and phone messages, which collaborators arranged in the internal communication channels at the nursing administrators in each hospital. A total of 189 nurses who fulfilled the inclusion criteria were included in this study. Inclusion criteria required participants to be RN nurse and/or nursing assistants and had access to the internet via computer and/or smartphone, to apply the inclusion criteria, there was a question about the job title with two responses (RN or Nursing assistant, and others); if the response was "others," the participant was excluded from the study.
Sample size applied for nurses working at the selected hospital in Jordan was determined using Epi-info 7 formed on a 5% variance at 95% confidence with 0.80 power at a 0.5 significance level. The minimum required sample size was determined to be (N = 164).
Instruments
Online questionnaires, adapted from previous studies (Fares et al., 2021, Fakonti et al., 2021, and Elhadi et al., 2021), were utilized in this study. To ensure content validity, nursing experts were consulted, including an Associate Professor in Medical Surgical Nursing, an Associate Professor in Community Health Nursing, and an Assistant Professor in Leadership and Management Nursing, who were selected from Tabuk and Cairo universities. To refine the survey items for language and expressivity, a pilot sample of 20 participants was used. The final questionnaire was estimated to take between 5 to 10 min to complete and was initially written in English before being translated into Arabic. The online survey comprised two parts: Part 1 focused on sociodemographic characteristics and health history, such as age, gender, education level, years of experience, chronic illness, had COVID-19 infection, and had COVID-19 vaccine. Part 2 investigated the participants’ perceptions towards COVID-19 vaccines, which consisted of six statements with three response levels (agree, undecided, disagree). The items in this section had good reliability, with a Cronbach's alpha of 0.665. Participants were given one point for each agree response and zero for disagree or undecided responses. Scores below 60% were considered a negative perception, while scores equal to or above 60% were considered a positive perception. The cutoff point was tested on a pilot sample of 20 participants, and 4 marks (60%) were chosen as the optimal cut-off point for a high likelihood ratio. Acceptance of the COVID-19 vaccine was measured by the participants responses to a question if they agreed to receive it. Responses were categorized as “agree,” “undecided,” or “disagree.” In this study, “undecided” responses were considered as “disagree” to examine the association between demographic variables and nurses’ acceptance of the vaccine. The potential factors investigated as influences on COVID-19 vaccine acceptance and perception included age, gender, education level, years of nursing experience, history of receiving the COVID-19 vaccine, presence of chronic illness, and history of COVID-19 infection.
Ethical Considerations
To ensure that this research adheres to ethical standards, it has received ethical approval from the Institutional Review Board at Applied Science Private University (IRB NO: 2020-2021-2-1), Amman, Jordan. Prior to starting the online questionnaire, a comprehensive information sheet was provided to participants to ensure informed consent. Confidentiality and privacy of the data were maintained by storing all personal information collected during the study in secure folders with restricted access only to the researchers, and measures were taken to prevent any unauthorized access.
Statistical Analysis
The data was collected, processed, entered, and analyzed using the Statistical Package for Social Sciences (IBM-SPSS version 21). Descriptive statistics such as frequency and percentage were used to report demographic data. The strength and direction of the linear relationship between sociodemographic characteristics (age, gender, education, experience, chronic illness, COVID-19 infection, and COVID-19 vaccine) and nurses’ perception of the COVID-19 vaccine were determined using Pearson correlation coefficients test, with a significant p-value <.05. The chi-square test was used to assess the association between sociodemographic factors and the level of acceptance, with a significant p-value <.05. Uncompleted forms were excluded from the analysis.
Results
Respondent Demographics and Their Health History
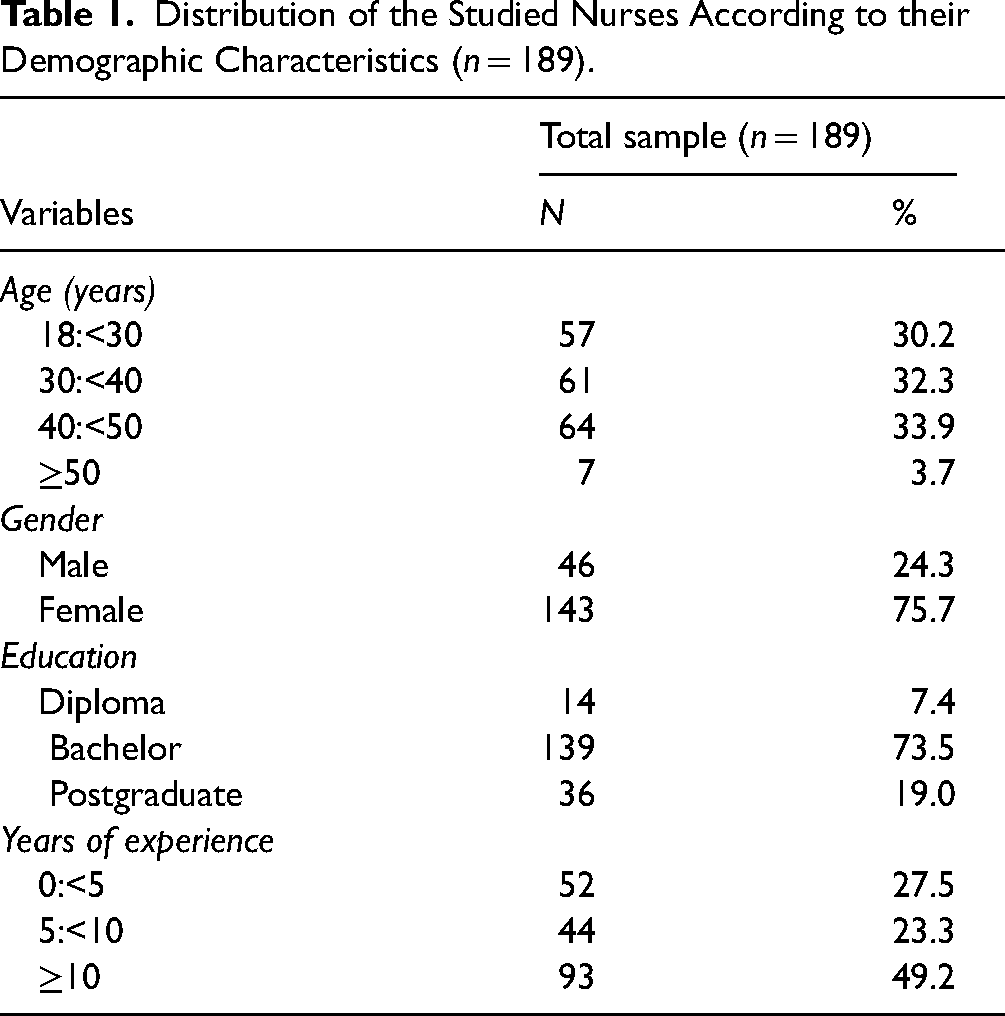
According to the analysis of data (n = 189), mean age of the participants was 30.2 ± 3.7 years, ranging from 18–50 years. Of the participants, 24.3% were males, 75.7% were females, 19.0% were Postgraduate, 73.5% were Bachelor, and 7.4% were Diploma. Participants’ working experience ranged from zero to more than 10 years, with a mean time of 27.2 ± 49.2 years (Table 1). The rate of people who said they had a long-term illness was 19.6%. Although 81.0% of the participant reported that they had COVID-19 vaccine, the rate of nurses who Suffer from COVID-19 infection was 42.3% (Table 2).
Distribution of the Studied Nurses According to their Demographic Characteristics (n = 189).
Percentage Distribution of Nurses According to their Health History (n = 189).

Respondent Perception Towards Corona Vaccine
Table 3 displays the perception of nurses toward corona vaccine. This table shows that 45.5% of the participants reported that the Coronavirus is man-made, whereas 38.6% disagree, 40.2% thought the Vaccines available in Jordan are considered safe. In comparison, 49.7% disagree, 56.6% agreed that COVID-19 Vaccines reduce the spread of disease, whereas 27.5% differ, 52.4% of the participants said they worried about the side effects of the COVID-19 vaccine. In comparison, 21.7% were not worried about side effects. Moreover, 45.0% of nurses said they trust scientific studies regarding the vaccine's effectiveness and complications, whereas 33.3% disagree. Besides, 9.5% of the studied sample said that vaccine complications are serious and should not be taken. In comparison, 28.6% did not consider the vaccine complications to be serious and should be taken (Table 3). Furthermore, 84.66% (160) had a negative perception toward the vaccine, while the remaining 15.34% (29) of the nurses had a positive perception toward it, as depicted in Figure 1. Additionally, Table 4 reveals a significant negative correlation between age and nurses’ perception of the COVID-19 vaccine (r = −.148, p = .043). This suggests that as age increases, nurses may have a less positive perception of the vaccine. Moreover, Table 4 demonstrates a negative correlation between the administration of the COVID-19 vaccine and nurses’ perception of it, although this correlation is marginally significant (p = .054), which means that it is close to, but does not quite reach, statistical significance at the 0.05 level. None of the other sociodemographic variables were significantly associated with nurses’ perception of the vaccine, as their p-values were >.05.

Percentage of the Studied Nurse's Perception About coronavirus disease 2019 (COVID-19) Vaccine (n = 189).
Distribution of the Studied Nurses’ Perception Towards the Corona Vaccine (n = 189).

Correlation Between Sociodemographic Characteristics and Nurses’ Perception About Coronavirus Disease 2019 (COVID-19) Vaccine (n = 189).

* Correlation is significant at the 0.05 level (2-tailed).
Respondent Acceptance of COVID-19 Vaccine
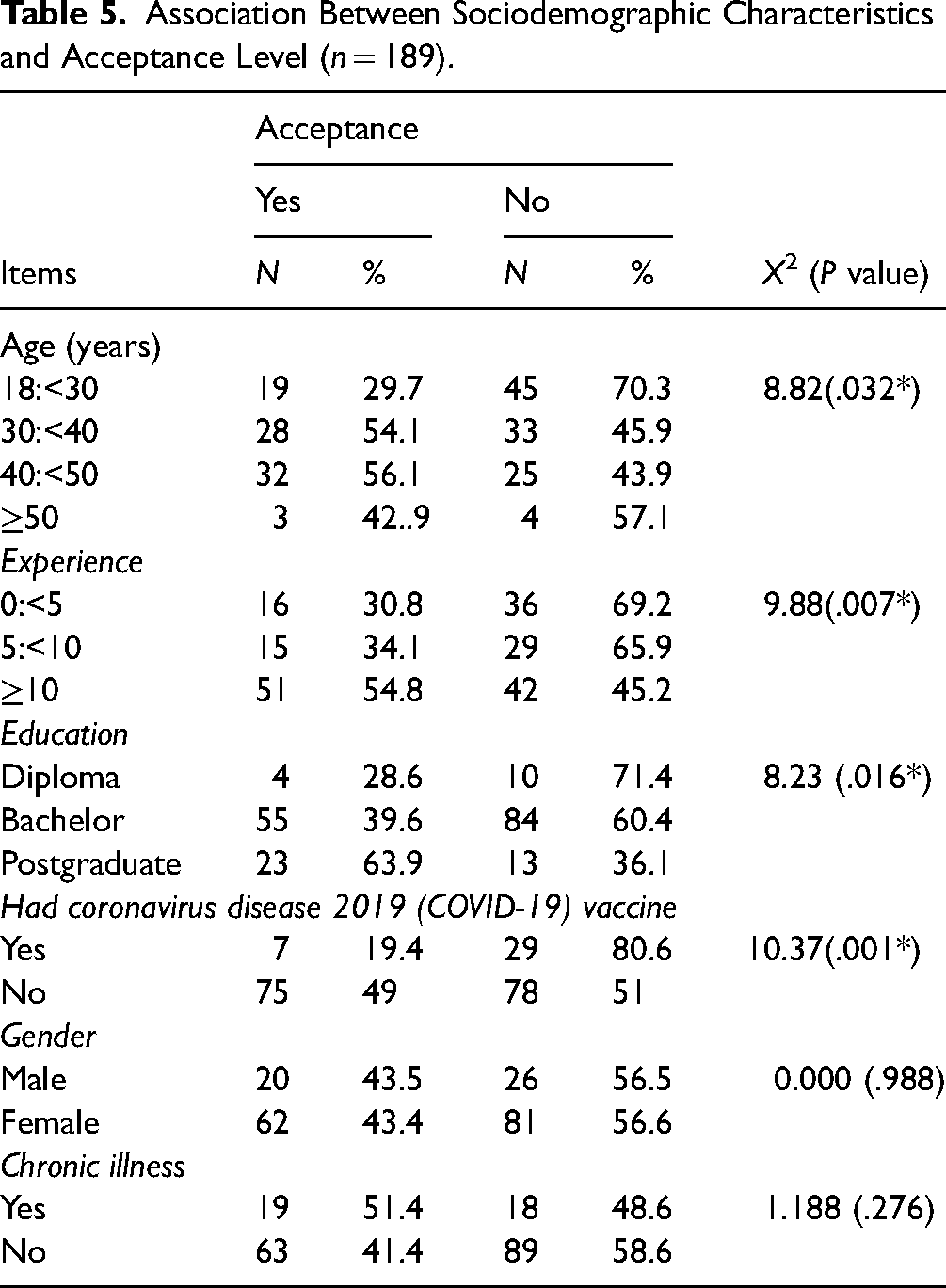
Table 5 depicts the association between demographic parameters and COVID-19 vaccination acceptance level in the examined group. This table indicated statistically significant discrepancies between allowable values for various age groups (p <.032), the lowest acceptance level (29.2%) was obtained for participants aged 18:<30, while the highest acceptance level (56.1%) was obtained for participants aged 40 to <50 years old. Furthermore, there have been significant statistical variations in acceptable levels of various Experience years (p = .007), with considerably lower acceptance levels acquired for 0:5 (30.8%) and greater acceptance level mean scores obtained for 10 years (54.8%). There were also statistically significant variations in acceptance of different levels of education (p = .016*), with Diploma nurses having a much lower acceptance rate (28.6%) and Postgraduate nurses having a significantly higher acceptance rate (63.9%). Furthermore, there were statistically significant variations in acceptable levels of nurses who got the corona vaccine (p = .001), with a considerably greater acceptance level for those who had the vaccine (49%) and a lower acceptance level for those who did not get the vaccine (19.4%). Table 5 also indicates that there is no significant relationship between nurses’ gender, chronic illness, and the acceptance of COVID-19 vaccine. Moreover, Figure 2 shows that 50.6% of nurses agree to receive COVID-19 vaccine compared to 25.5% disagree, and 23.9% of nurses they were undecided about COVID-19 vaccine.

Percentage of the studied nurse's acceptance regarding coronavirus disease 2019 (COVID-19) (n = 189).
Association Between Sociodemographic Characteristics and Acceptance Level (n = 189).
Discussion
This study was conducted among Jordanian nurses to investigate their perceptions, acceptance, and factors affecting their decisions toward the COVID-19 vaccines. It was found that 42.3% of the participants were infected with coronavirus. Meanwhile, 81% of the participants received the COVID-19 vaccine (Table 2). This percentage is considered acceptable and high given the magnitude of the COVID-19 pandemic. Moreover, this study revealed that more than half (50.6%) of the nurses agreed to receive the vaccine compared to less than one-third (25.5%) who disagreed (Figure 2). These findings indicate that even though 81% of nurses received the COVID-19 vaccine, only 50.6% of them agreed to receive it, suggesting that some nurses may have been forced to receive the COVID-19 in accordance with hospital policies. This conclusion corroborates findings from a Saudi Arabian investigation (Alhofaian et al., 2021), in which more than two-thirds of the health care provider is willing to receive the vaccine, and nurses have reported the highest acceptance level among healthcare providers. Additionally, it corroborates the findings of French research (Gagneux-Brunon et al., 2021) which revealed that 76.9% of the healthcare provider accepted the Vaccine. Yet it is odd with the finding of a study conducted in Taiwan (Kukreti et al., 2021) which revealed that willingness to receive the vaccine among healthcare providers and outpatients appeared low.
The present study found that 84.66% of the nurses had a negative perception of the vaccine, while 15.3% of them had a positive perception toward it (Figure 1). This finding suggests that the majority of the surveyed nurses have a negative perception of the COVID-19 vaccine. Possible reasons for this negative perception could include concerns about the safety or efficacy of the vaccine, misinformation, or lack of information about the vaccine, or personal beliefs or values that conflict with vaccination. However, the result of this study showed that around 50% of participants expressed safety issues regarding the vaccination once it became accessible, as evidenced by their concern regarding potential adverse effects. Additionally, fewer than half (45.5%) of individuals felt that the COVID humans created 19 viruses, almost half of them (49.7%) thought the vaccines available in Jordan were considered not safe, more than half (56.6%) agreed that COVID-19 vaccines reduce the morbidity and mortality, and (52.4%) of the participants concerned about the vaccine's adverse effects and its complication. Besides, less than half (45.0%) of nurses were trusted by the scientific studies regarding the vaccine's effectiveness and complications. In comparison, less than one-third of them (28.6%) considered the Vaccine complications severe and should not be taken. This finding corresponds with the results of (Elhadi et al., 2021) who reported that among 2452 healthcare providers (37%) of the worries regarding vaccine-related serious consequences, (38.7%) considered COVID-19 to be man-made; (86%) felt vaccination might help reduce morbidity and death rates (Elhadi et al., 2021).
Additionally, the new study's findings corroborate Pogue et al’ conclusion that most participants (63%) in the United States of America expressed concern about the COVID-19 vaccine's negative effects (Kregar Velikonja et al. 2021). Additionally, (Fakonti et al., 2021) found in his study that the primary reasons for nurses and midwives in Cyprus not obtaining the COVID-19 vaccine were worries about the vaccine's rapidly fear and developing of side effects. Although (Fares et al., 2021) found that vaccine hesitation was due to a lack of clinical testing and concern about vaccine side effects, the primary factor that may boost vaccination acceptability among healthcare professionals was access to sufficient and correct information about available vaccinations. Another survey performed in Jordan discovered that (49%) of participants felt that most of the people would avoid taking the Vaccine owing to worries about the Vaccine's adverse effects and that they simply don't trust any information regarding the vaccine (El-Elimat et al., 2021). TV, newspapers, radio, social networks, colleagues, friends, healthcare providers, scientists, and government officials have all been sources of health information and knowledge about the COVID-19 pandemic (Ali et al., 2020). Providing accurate information and transparency about vaccine safety and effectiveness is essential to building people's trust, especially those uncertain about vaccines. For any future national vaccination campaign to be successful, it is necessary to identify the sources of information most trusted by the public about COVID-19 (El-Elimat et al., 2021).
The findings of this study showed that age is significantly negatively correlated with nurses’ perception of the COVID-19 vaccine, suggesting that as age increases, nurses may have a less positive perception of the vaccine. Furthermore, a negative correlation between the administration of the COVID-19 vaccine and nurses’ perception of it was found in this study. However, this correlation was only marginally significant (p = .054), meaning it was almost statistically significant but did not quite reach the level of significance at (0.05). Additionally, this study found none of the other sociodemographic variables, including gender, education, experience, chronic illness, and history of COVID-19 infection, were significantly correlated with nurses’ perception of the vaccine. This finding is consistent with a study conducted in China among HCWs, which found that older HCWs were less likely to accept the COVID-19 vaccine than younger HCWs, likely due to their concerns about the vaccine's safety and efficacy (Wang et al., 2021). Similarly, another study conducted in the United States found that HCWs aged 50 and older were less likely to report receiving the COVID-19 vaccine than younger HCWs, possibly due to their greater concerns about the vaccine's safety and side effects (Painter et al., 2021). According to Hurley and Freund (2021), age is negatively correlated with COVID-19 vaccine acceptance, which suggests that older adults may have a less positive perception of the vaccine. Furthermore, Taylor, Landry, Paluszek, and Fergus (2021) found that HCWs who had not received the COVID-19 vaccine were more likely to have negative perceptions of the vaccine, including concerns about safety and efficacy. Overall, these findings underscore the need to consider age and perceptions, when developing strategies to promote COVID-19 vaccine acceptance among HCWs.
The present study revealed that the lowest acceptance level (29.2%) was among those aged 18 years to less than 30 years old, while the highest acceptance level (56.1%) was among those aged 40 years to less than 50 years old. This finding corroborates findings from Libyan research (Elhadi et al., 2021) which reported that the highest acceptance level was among age 31 to less than 50 years old of health care providers. In contrast to another study done in Jordan, (El-Elimat et al., 2021) suggested that older age groups >35 years old have been less likely to receive COVID-19 immunizations than younger age groups. This discrepancy is thought to be attributable to the study's methodology, as senior respondents are less likely to engage in online surveys. In addition, a lower acceptance level was among less than 5 years of experience (30.8%), whereas the higher acceptance level was among more than 10 years (54.8%). This finding corresponds with the results of (Fakonti et al., 2021), who reported that nurses with more years of experience were intended to accept the vaccine in Cyprus. This conclusion is consistent with research done in Turkey; a correlation was discovered between years of extensive experience and vaccination acceptability among healthcare providers (Yigit et al. 2021). There is a strong possibility that the COVID-19 vaccination will be approved in the older age range, as they are more vulnerable and more likely to be interested in utilizing it. At the same time, more experienced nurses could see the positive effects of vaccination and therefore be less reluctant. The current study revealed that Diploma nurses had a lower acceptance level (28.6%), while postgraduate nurses had a higher acceptance level (63.9%). These results correspond with a study conducted in Pakistan that revealed that HCWs who have a higher level of education reported higher levels of acceptance of vaccines (Malik et al. 2021). Yet, this conclusion contrasts with the findings of (Fares et al., 2021 & Fakonti et al., 2021), who found no statistically significant relationships between educational attainment and degree of acceptance among healthcare personnel. This discrepancy might be due to differences in the methodology and study settings.
The current study's findings also showed that there was no significant association between the acceptance of the COVID-19 vaccine and the gender of the nurse or their chronic disease. This result was supported by Gagneux-Brunon et al. (2021) who found that chronic condition was not a predictor of acceptance of COVID-19 vaccine among HCWs. Yet, this conclusion odd with the results of Malik et al. (2021), who reported that female gender was a predictor for accepting or refusing the COVID-19 vaccine among HCWs. Also, the results of Yigit et al. (2021), who revealed that male gender was a predictor for COVID-19 acceptability among healthcare practitioners. The study's sample size is assumed to be responsible for this disparity. To manage a pandemic, the COVID-19 vaccine must be available and effective. There must be trust and acceptance for health and policy decisions. As a result, both the general public and HCPs have voiced their unhappiness. Vaccination refusal can be caused by hesitancy and postponement. To increase vaccination rates among nurses in Jordan, it is essential to combine education and recommendations. Herd immunity requires higher levels of compliance among nurses, according to our research. It is necessary to reduce anxiety and increase vaccination confidence. As a result, nurses should be informed about the vaccine advantages and the dangers of sickness for themselves, their families, and their patients.
Strengths and Limitations
Our study results are providing an initial and first report about the perception and acceptance of COVID-19 vaccine among Jordanian nurses as well as the factors that influence their acceptance. This will help the policymakers to plan a vaccination program and promote nurses according to the predictors of acceptance identified in this study. This can be viewed as the study's strength. Even though our study sample was small, a limit factor in our study is the use of a nonrandom sampling technique which raises questions about its representativeness, which limits the generalizability of our findings. Another one is that participation required access to a computer, tablet, or smartphone, which could have led to bias in participant selection. In addition, at a time when COVID-19 vaccines are still being developed and tested, we noticed participants’ willingness to accept a vaccine. Therefore, people's opinions on vaccination may change when more evidence about the safety and efficacy of COVID-19 vaccines becomes available. In addition, a chi-square test was used in this study to identify the factors influence on COVID-19 vaccine acceptance among Jordanian nurses. In fact, the chi-square test cannot be used to determine the direction and magnitude of the association. We suggested that future studies with a larger sample size use a multivariable regression analysis to identify the factors influence on COVID-19 vaccine acceptance. As a result, the association's adjusted effect sizes can be reported.
Implications for Practice
The findings of this study indicate that a significant number of nurses have negative perception about COVID-19 vaccine and exhibit hesitancy toward taking it. To address this concern, healthcare policymakers should improve communication with nurses through various channels, involving them in online meetings and workshops to provide accurate information about the vaccine, and create a supportive environment to improve vaccination rates among HCWs. Overall, this study provides valuable insights into nurses’ perceptions and acceptance of the COVID-19 vaccine, which can inform strategies to increase vaccination rates and achieve better disease control.
Conclusion
The findings of the current study shed light on nurses’ perception and acceptance of the COVID-19 vaccine, as well as the factors influencing their perception and acceptance. which showed that nurses’ perception and acceptance of the COVID-19 vaccine were significantly associated with various factors, including age, years of experience, and educational level. The majority of the nurses had a negative perception of the vaccine, and only half of them agreed to take the vaccine. Additionally, many nurses had concerns about the safety and side effects of the vaccine and believed that the Coronavirus was man-made. The study results suggest that efforts need to be made to address these concerns and increase nurses’ awareness of the importance of vaccination in disease control.
Footnotes
Acknowledgments
The authors thank the nurses who participated in this study.
Author Contribution:
K.A.R. and A.H.A contributed to the study conception and design, data collection, data analysis and interpretation, and drafting and critical revision of the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
The Institutional Review Board of the Applied Science Private University (IRB NO: 2020-2021-2-1 Date: 16-6-2021) approved the study.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Prior to starting the online questionnaire, a comprehensive information sheet was provided to participants to ensure informed consent.