
Abstract
Introduction
Illness perception and self-efficacy in patients with coronary artery disease (CAD) may affect medication adherence, which is one of the most important challenges in disease management in this group of patients.
Objective
The present study aimed to investigate the factors influencing medication adherence in CAD patients, especially the effect of illness perception and self-efficacy.
Methods
This study was cross-sectional and conducted from April to September 2021. A total of 259 patients with confirmed CAD were selected by convenience sampling method based on inclusion criteria. Illness perception, self-efficacy, and medication adherence were investigated using Brief IPQ, SCSES, and MARS_10 questionnaires, respectively. The data were analyzed using the STATA software (version 14) and the regression path analysis method.
Results
Patients had moderate illness perception and high self-efficacy, and 61.8 of them adhered to their medication regimen. Greater illness perception, better self-efficacy, and higher education had a positive effect on medication adherence, and increasing age had a negative effect on it. The final path model shows a good fit of the data in the model (χ2: 0.37, df: 274, χ2/df: 0.36, CFI: 1, IFI: 0.95, TLI: 1.07, and RMSEA: 0.00).
Conclusion
The results of the present study suggest that patients’ illness perception can play an important role in predicting self-efficacy in disease management and the level of medication adherence in patients with CAD. To improve self-efficacy and medication adherence, future intervention studies should focus on the patient's illness perceptions and their improvement.
Introduction
Coronary artery disease (CAD) is the most common cause of death in developed and developing countries and has an annual mortality rate of about 7 million (Abubakar et al., 2015; Alizadehsani et al., 2018). In Iran, CAD is the most common cause of death, which accounts for approximately 50% of the death rate per year (Hatmi et al., 2007). This disease can lead to severe consequences such as congestive heart failure, acute pulmonary edema, cardiogenic shock, and a high mortality rate (Hosseinzade et al., 2013). It seems that considering the progressive and chronic nature of CAD, controlling and managing the disease is an important measure (Lindholm & Mendis, 2007). In the meantime, medication adherence is a modifiable, important behavior, and also a cornerstone of CAD management (Zullig et al., 2017). Today, medication therapy is known as one of the effective approaches for the treatment of CAD patients alone and together with other procedures such as angioplasty and coronary artery bypass surgery (Hinkle & Cheever, 2018). But in the meantime, medication adherence in patients with CAD as a chronic, progressive, and lifelong disease is one of the important challenges facing disease management (Ni et al., 2022). The treatment of chronic diseases is mainly accompanied by the long-term use of many different types of drugs, and improved medication adherence can have a significant effect on the health of patients, but due to insufficient medication adherence, their full benefits are often not realized (Brown & Bussell, 2011). According to the results of studies, the rate of medication non-adherence in heart diseases ranges from 33% to more than 55% (Al-Ganmi et al., 2018; Allahbakhshian & Gholizadeh, 2020). Medication non-adherence can cause adverse consequences such as frequent admissions, increased use of medical services and care costs, reduced quality of life, and increased mortality (Park et al., 2015; Vervloet et al., 2012). Medication adherence is one of the dimensions related to adherence to treatment; in a report, the World Health Organization (WHO) classified the factors of adherence to treatment into five groups: socioeconomic, health care team and system, therapy, patient, and condition-related factors (Organization, 2003). On the other hand, one of the variables that can predict patients’ behaviors in disease management, including medication adherence, is illness perception which refers to the patient's organized beliefs about his/her disease and affects adaptive responses, health, and adherence to a healthy lifestyle (Al-Smadi et al., 2016; Miyazaki et al., 2018). Illness perception is the main factor in predicting the patient's presence and active performance in the treatment and subsequent outcomes (Zare et al., 2016). Among these, one of the concepts influencing the behaviors related to disease management in patients with chronic diseases is self-efficacy was defined by bandura in 1977, shows the beliefs and judgments of a person about his/her abilities in performing duties and responsibilities throughout his/her personal life (Park et al., 2015). It is important to determine the factors affecting self-efficacy in improving its level because it is not possible to improve the level of self-efficacy without identifying such factors (Hatef et al., 2018). Meanwhile, illness perception can be effective on self-efficacy in patients with chronic diseases (Mohammadi et al., 2022). Self-efficacy can be considered an effective factor in improving self-care and controlling CAD (Barnason et al., 2003). Although there have been some studies on the relationship between the above variables, this is the first study that simultaneously and comprehensively investigates the relationship between illness perception, self-efficacy and, medication adherence in patients with CAD in a conceptual model and by examining the effect of mediating variables and there is no similar study that has simultaneously examined the relationship between these three variables in this group of patients. Besides, although according to the results of previous studies, having a correct, appropriate and real illness perception may be effective in creating and changing self-efficacy and medication adherence, and effective self-efficacy also plays a role in the medication management and adherence but contradictory and different results have been obtained in some studies that have investigated the relationship between illness perception, self-efficacy and medication adherence, such as the existence of a negative relationship or no significant relationship between the illness perception and self-efficacy with medication adherence (McCulley et al., 2018; Saarti et al., 2016).
Therefore, the present study aims to investigate the relationship between illness perception, self-efficacy, and medication adherence and to identify the direct, indirect, and total effects of demographic, clinical, and behavioral variables on medication adherence and especially focusing on the role of illness perception and self-efficacy in CAD patients.
Review of Literature
In 2018, Miyazaki et al. conducted a study to investigate the relationship between medication adherence and illness perception in patients with atrial fibrillation treated with direct oral anticoagulants. This study determined that illness perception can affect adherence to the medication regimen in patients. The illness perception is one of the factors that can be changed and it is an essential factor in medication adherence in patients with chronic diseases (Miyazaki et al., 2018). In the study conducted by Kim et al. in 2020 with the presence of people with type 2 diabetes aged 50 years and older, it has been reported that illness perception can play an important role as a significant factor in medication adherence and the existence of self-efficacy and medication adherence in good level are among the effective factors for maintaining the desired level of health (Kim et al., 2021b). In 2020, Gutierrez and Sakulbumrungsil published a study aimed at evaluating the factors associated with medication adherence in patients with hypertension in the Philippines in the form of a systematic review. In the results of this study, it is reported that factors such as young age, celibacy, low education level, low health literacy, low knowledge, negative attitude towards the disease, low social support, low self-efficacy, and low illness perception are factors that can go along with poor medication adherence (Gutierrez & Sakulbumrungsil, 2021). In Mohammadi et al.'s study, the relationship between illness perception and self-efficacy is mentioned. In this study, illness perception and self-efficacy had a positive relationship and patients in this study in a high level of illness perception and self-efficacy. The researchers in this study admit that the illness perception should be evaluated in patients who have weak self-control skills and nurses can help patients in this field by carrying out interventions to improve illness perception and self-efficacy (Mohammadi et al., 2022). In the study by Saarti et al. in 2016, approximately 71% of the participants adhered to the medication regimen for high blood pressure. Those people who had higher scores related to illness perception had lower mean scores of medication adherence, however, no significant statistical relationship was observed between illness perception and medication adherence (Saarti et al., 2016).
Due to a myriad of variables affecting the control and management of chronic diseases, medication adherence in patients plays an integral role in ensuring the effectiveness of healing process. In spite of some preceding studies featuring and exploring the existing relationship between medication adherence and other involved variables such as illness perception and self-efficacy, due to the different results of studies and the unique differences of patients suffering from CAD as a disease with its adverse consequences and high mortality rate, the present study was deemed relevant to subject matter. Therefore, the present study seeks to amend the lack of relevant literature review through careful assessment of factors influencing CAD patient's medication adherence, especially those associated with aforementioned involved variables. In this study, the presented model makes use of the path analysis method conducted simultaneously and for the first time within a controlled group of CAD patients.
Theoretical Framework
In this study, illness perception and self-efficacy were considered as two variables that may be related to medication adherence in patients with CAD. Regarding illness perception and self-efficacy, Leventhal's self-regulatory model and Bandura's theories are mentioned respectively. Leventhal's self-regulatory model was proposed in 1980 and is also known as the common-sense model. Previous studies investigated illness perception based on Leventhal's self-regulatory model and classified this variable into five dimensions: identity, timeline, consequences, cause, and cure/control (Hale et al., 2007). Additional research added illness coherence, concern, and emotional manifestations to these five dimensions, and the control dimension was divided into two dimensions: personal control and treatment control (Moss-Morris et al., 2002). Leventhal believes that people use the advice given to manage their disease when they have a correct illness perception that this can lead to a reduction in mortality, complications, and consequences of the disease and an improvement in quality of life (Leventhal et al., 1992). The researches of Leventhal and his colleagues show that knowing the illness perception leads to the recognition of factors affecting the adaptation and acceptance of the disease process and leads to the improvement of support programs for patients. In addition, it also provides the possibility that the guidelines and nursing programs be designed carefully based on evidence and provide more effective help to respond to the needs of patients (Broadbent et al., 2009). According to Bandura, self-efficacy is a dynamic cognitive process in which a person evaluates his ability to perform a specific task. According to him, the higher the perceived self-efficacy in people, the more ability they will have in choosing challenging behaviors, the more effort they will have and the more success in doing them, and the more stable they will be when problems arise and people that have a low self-efficacy, they will dedicate less effort to do a task or reach a goal, and they may have a greater desire to leave it. Self-efficacy leads to changes and differences in people's performance, feeling, and thinking (Bandura & Cervone, 1986). Based on the existing theories, we assumed that there is a possibility of a relationship between these two variables with medication adherence. However, the review of the literature observed the contradictory results in studies such as the absence of correlation or positive or negative coefficients in the relationship between variables, which made this study be conducted for the first time in patients with CAD to investigate the effects and relationship between these variables in a model by path analysis.
Methods
Design
This was a cross-sectional and descriptive correlational study from April to September 2021. The article is written in the path analysis method.
Hypotheses
Illness perception affects self-efficacy in patients with CAD referred to the specialized heart clinic.
Illness perception affects medication adherence in patients with CAD referred to the specialized heart clinic.
Self-efficacy affects medication adherence in patients with CAD referred to the specialized heart clinic.
Illness perception and self-efficacy are predictors of medication adherence.
Sample
To access research samples, the researcher referred to the cardiovascular medical and training center and its specialized clinic, affiliated to Tabriz University of Medical Sciences from April to September 2021. A total of 259 eligible patients with confirmed CAD were selected and included in the study based on the inclusion criteria and convenience sampling method. The purpose of the study was explained to the participants and if they wanted to participate in the study, informed consent was obtained from them and the questionnaires were completed in the form of separate interviews and receiving information from the patients themselves to avoid bias in the study. The sample size in this study was calculated based on a descriptive correlation study and using the formula mentioned below, but the article was written based on the path analysis method. One of the minimum sample size recommendations for SEM is 200 which is based on having a sufficient sample size to reduce the likelihood of convergence problems and to obtain unbiased estimates or standard errors. This sample size is enough to perform path analysis, according to the references related to SEM models, which suggest a minimum sample size of 200 (Jackson, 2001).
The standard normal deviate for α = Zα = 1.9600
The standard normal deviate for β = Zβ = 1.2816
C = 0.5 * ln[(1 + r)/(1−r)] = 0.2027
Total sample size = N = [(Zα+Zβ)/C]2 + 3 = 259
Research Tools
Brief Illness Perception Questionnaire
The Brief Illness Perception Questionnaire (BIPQ), developed by Broadbent et al. (2006), was used to assess the patients’ illness perception. This questionnaire consists of 9 items that evaluate illness perception based on an 11-point Likert scale. The possible score range for the first eight questions is from 0 to 10. Question 9 is open-ended and ranks from 1 to 3 based on the three items of lifestyle, stress, and heredity as the cause of the disease of the participants from their point of view. The first five items are cognitive perceptions, including consequences, timeline, personal control, treatment control, and identity. Items 6 and 8 investigate emotional aspects including concern and emotional representation and question 7 investigates the understanding of illness or comprehensibility (Broadbent et al., 2006). To compute the total score of illness perception, the reverse scores of items 3, 4, and 7 will be added to items 1, 2, 5, 6, and 8 and the final score range is from 0 to 80. Scores 0–27, 28–55, and 56–80 indicate low, moderate, and high illness perception, respectively. Higher scores mean that participants have considered their disease as a serious and threatening disease, and lower scores indicate a more optimistic view of the disease (Nur, 2018). For this questionnaire, internal consistency reliability has been reported using Cronbach's alpha coefficient (α = 0.8) and the total test-retest reliability coefficient for the 6-week interval ranged from 0.42 to 0.75 (Broadbent et al., 2006). The Persian version of the illness perception questionnaire has been confirmed by Bazzazian with appropriate validity and reliability (Bazzazian & Besharat, 2010).
The Sullivan's Cardiac Self-Efficacy Scale
In the present study, Sullivan's Cardiac Self-Efficacy Scale (SCSES) was used to evaluate self-efficacy, which was designed by Sullivan et al. (1998). This questionnaire consists of 16 questions and assesses the patient's self-efficacy based on a 5-point Likert scale ranging from 0 to 4: 0 (not at all sure), 1 (low), 2 (moderate), 3 (high), and 4 (I am very sure). This questionnaire investigates self-efficacy in three dimensions: control symptoms subscale (questions 1–10), lifestyle-related questions (questions 11–12), and maintain function subscale (questions 13–16) (Fors et al., 2015). The possible score range is 0 to 64. Scores 0–22, 23–32, and 33–64 indicate low, moderate, and high self-efficacy, respectively (Keshavaraz et al., 2020). Sullivan et al. reported a Cronbach's alpha coefficient of 0.90 and 0.87 for symptom control and maintain functioning dimensions, respectively (Sullivan et al., 1998). In Iran, Varaei et al. have investigated the validity and reliability of this questionnaire, and the reliability of this questionnaire has been reported (α = 0.97) (Varaei et al., 2017).
The Medication Adherence Report Scale
The MARS-10 questionnaire was designed by Katherine Thompson and consists of 10 items with yes–no answer format and evaluates three dimensions related to medication adherence: the patient's behavioral dimension in medication adherence (questions 1–4), the patient's attitude towards medication adherence (questions 5–8), and the evaluation of the patient's attitudes to negative side effects towards taking medication from their point of view (questions 9–10). The score range is 0 to 10, scores 5 and below indicate medication non-adherence, and 6 and above indicate medication adherence (Wang et al., 2020). It is expected that the patient will answer yes to questions 7 and 8 and answer no to other questions with a positive attitude and medication adherence (Prabahar et al., 2020). Cronbach's alpha coefficient of this questionnaire was calculated as 0.75 (Thompson et al., 2000). In Iran, the validity and reliability of the Persian version of this questionnaire on patients with bipolar disorders have been confirmed (α = 0.82) (Javadpour et al., 2013).
The Abbreviated Mental Test
In this study, the Abbreviated Mental Test (AMT) questionnaire was used to evaluate the cognitive status of the participants. This questionnaire was first designed by Hodkinson in 1972 (Hodkinson, 1972) and contains 10 questions, each question has one score and scores between 7 and 10 indicate the absence of cognitive disorders and a normal state (de Caso et al., 1994). The psychometry of this tool was done in 2014 by Foroughan et al. in Iran and the validity and reliability of the Persian version of the AMT have been appropriate (α = 0.76) (Bakhtiyari et al., 2014).
Demographic and clinical data of patients were also collected using a standardized questionnaire.
Inclusion/Exclusion Criteria
Inclusion criteria included: (1) Being at least 18 years old, (2) Patients with CAD confirmed by a cardiologist, (3) Ability to take medications independently, (4) The ability to communicate, (5) CAD diagnosed at least 6 months ago (Gholami et al., 2018), (6) Being treated with cardiac drugs, (7) Absence of psychiatric disorders according to the patient's medical record, (8) Absence of cognitive disorders (assessed by the AMT questionnaire), (9) Willingness to participate in the study. Exclusion criteria included: (1) Patients in the acute stage of the disease, (2) Having a malignant or difficult to cure disease, (3) Declaring dissatisfaction and unwillingness to continue participating in the study.
Institutional Review Board Approval
For anonymity, the information in this section is not included in the main text.
Statistical Analysis
Data analysis was carried out by the path analysis method to determine the direct, indirect, and total effects of behavioral, clinical, and demographic variables on medication adherence in STATA ver. 14. Path coefficients were all standardized. In this study, the reported p-value for the path coefficients demonstrates the significance of the relationships between the variables. The significance level bar was considered .05, and as a result, a p-value of less than .05 was considered significant. Also, chi-square/df of ≤ 2, comparative fit index (CFI) of ≥ 0.95, Tucker-Lewis index (TLI) of ≥ 0.95, and root mean square error approximation (RMSEA) of < 0.06 were used to evaluate the model fit (Fabrigar et al., 1999). This sample size was big enough to allow the inclusion of 16 independent variables in the path regression analysis. The recommended sample size for pass analysis is a minimum of 10 subjects for each included variable (Kline, 2015). As mentioned earlier, demographic, clinical, and behavioral variables were included in the model, and the hypothetical relationships between these variables are shown in Figure 1.

Self-efficacy can be influenced by the illness perception and influence the medication adherence. Also, behavioral variables can be influenced by demographic and clinical variables.
Results
Sample Characteristics
A total of 259 eligible patients with confirmed CAD were included in the present study. Table 1 shows the demographic and clinical characteristics of the participants. The mean ± SD of participants’ age was 63.05 ± 6.31 years. More than half of the participants were men (68.7%) and 97.3% of the participants were married. A total of 93.8% of the participants had an associate degree and below and others had a bachelor's and MA. The majority of the participants were self-employed (45.9%). Most of the participants lived in cities (93.1%) and 6.9% lived in villages. A total of 75.7% of study subjects had no sufficient income. Among the underlying diseases, hypertension, diabetes, and hyperlipidemia, hypertension was the most prevalent disease (65. 3%). Antiplatelet drugs (78.8%) were the most common drugs used by the participants. A total of 38.6% and 8.1% of participants had a history of angiography and coronary artery bypass graft, respectively. The ejection fraction in most participants (62.6%) was in the range of 40%–50%.
Sociodemographic and Clinical Characteristics of the Participants (n = 259).

CABG = coronary artery bypass graft; EF = ejection fraction.
Illness perception, self-efficacy, and medication adherence status are shown in Table 2 and the direct, indirect, and total effects of demographic, clinical, and behavioral variables on medication adherence are also shown in Table 3. Moreover, the results showed direct, indirect, and total effects of demographic, clinical, and behavioral variables on medication adherence, although all these effects were not significant. It should be noted that illness perception and self-efficacy were also influenced by some demographic, clinical, and behavioral variables (Al-Smadi et al., 2016; Sarkar et al., 2007) (Figure 2). Furthermore, the mean ± SD of illness perception was 44.45 ± 3.22, which showed a moderate illness perception. Results also demonstrated that the mean ± SD of self-efficacy was 34.06 ± 7.57, which indicates a high self-efficacy level. Also, more than half of the participants (61.8%) adhered to their medication regimen (mean ± SD = 6.01 ± 1.09). Table 4 shows the response rate to questions of the medication adherence questionnaire.
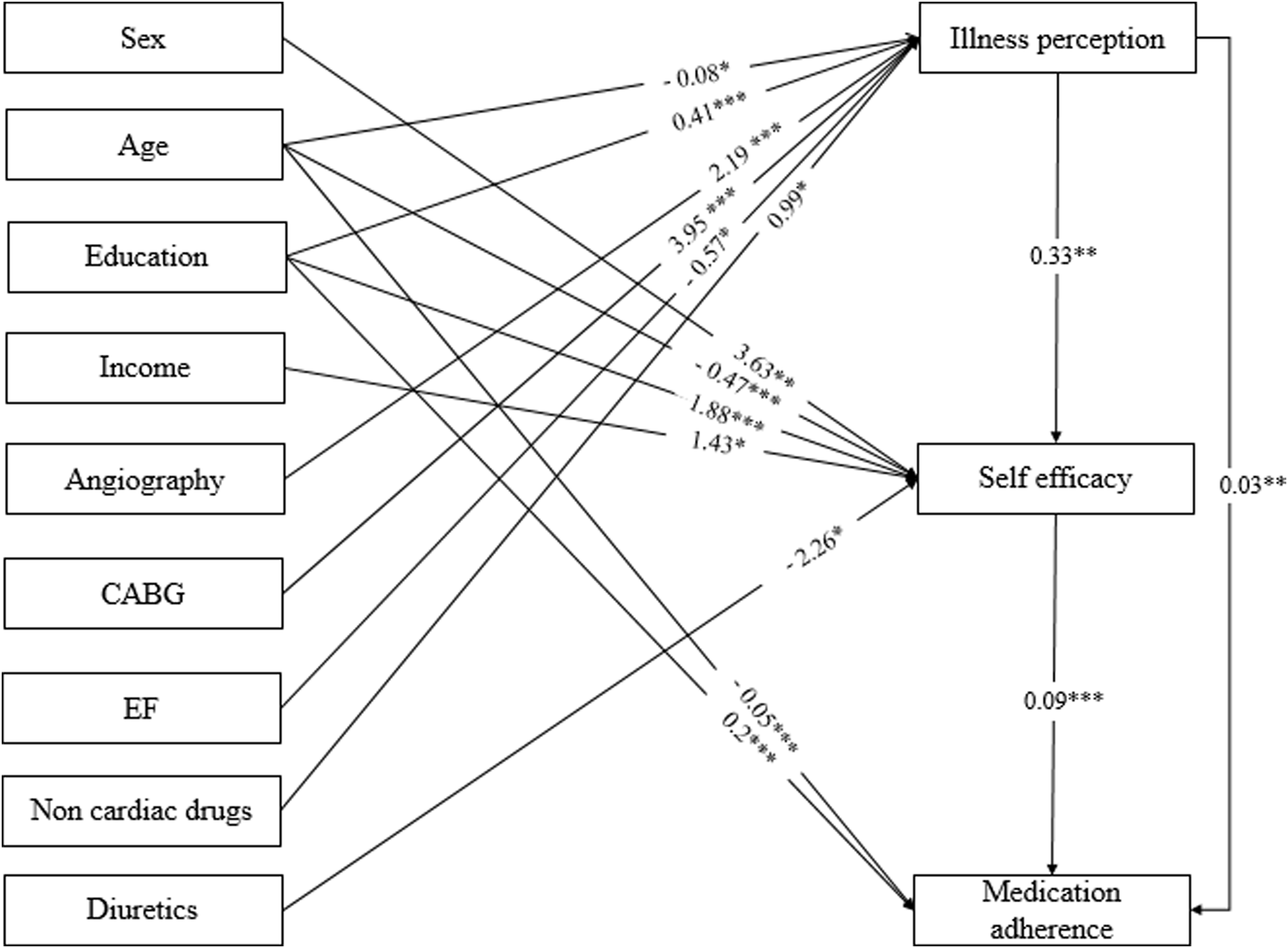
Standardized path coefficients and the interaction between the variables, which has shown only statistically significant paths (p < .05). *p < .05; **p < .01; ***p < .001.
The Mean (SD) Scores of Illness Perception, Self-Efficacy, and Medication Adherence (n = 259).
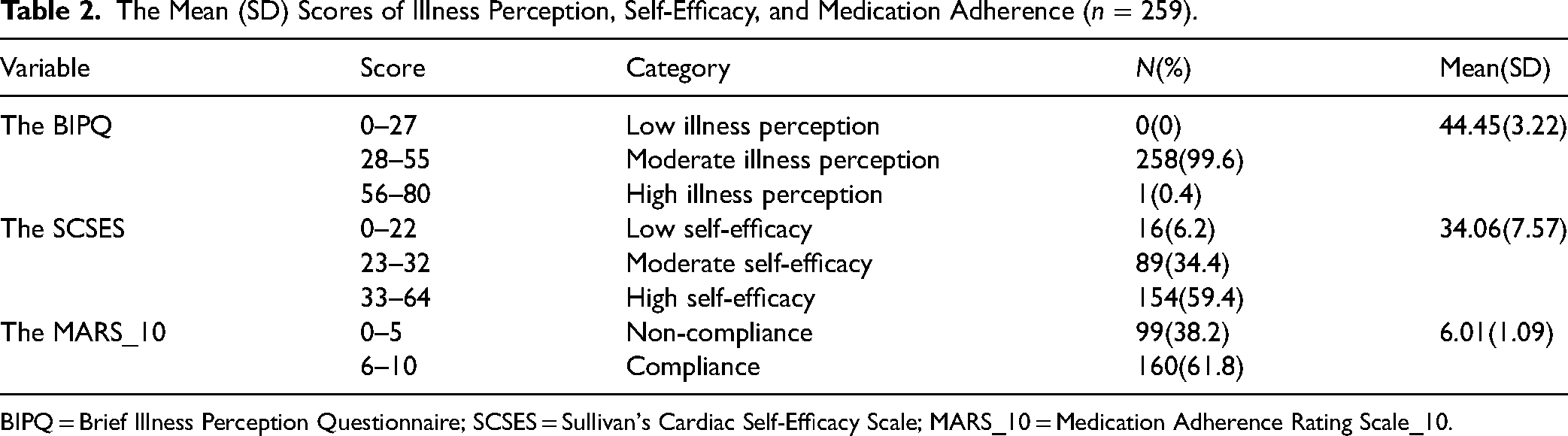
BIPQ = Brief Illness Perception Questionnaire; SCSES = Sullivan's Cardiac Self-Efficacy Scale; MARS_10 = Medication Adherence Rating Scale_10.
The Standardized Direct, Indirect, and Total Effects of Different Sociodemographic, Behavioral, and Clinical Factors on Medication Adherence (n = 259).

CABG = coronary artery bypass graft; EF = ejection fraction.
Participants’ Trends Toward Medication Commitment (n = 259).

Illness Perception and Self-Efficacy
Regarding the effect of behavioral variables, illness perception had a direct effect on self-efficacy, and people with a higher illness perception had a more favorable self-efficacy.
Illness Perception and Medication Adherence
Illness perception also had an indirect effect on medication adherence, that is, a perception of the threatening and serious conditions of the disease led to better medication adherence. Illness perception also had an indirect effect on medication adherence through self-efficacy.
Self-Efficacy and Medication Adherence
Self-efficacy had a direct effect on medication adherence, and higher self-efficacy had a positive effect on medication adherence.
Results of the present study also revealed that greater illness perception (β = 0.03), better self-efficacy (β = 0.09), and higher education (β = 0.2) had a positive effect on medication adherence, and increasing age (β = −0.05) had a negative effect on it. Table 5 shows a summary of the final state of the studied model, which indicates the good fit of the data in the model (χ2: 0.37, df: 274, χ2/df: 0.36, CFI: 1, IFI: 0.95, TLI: 1.07, and RMSEA: 0.00).
Summary of Final Model Fit Statistics.
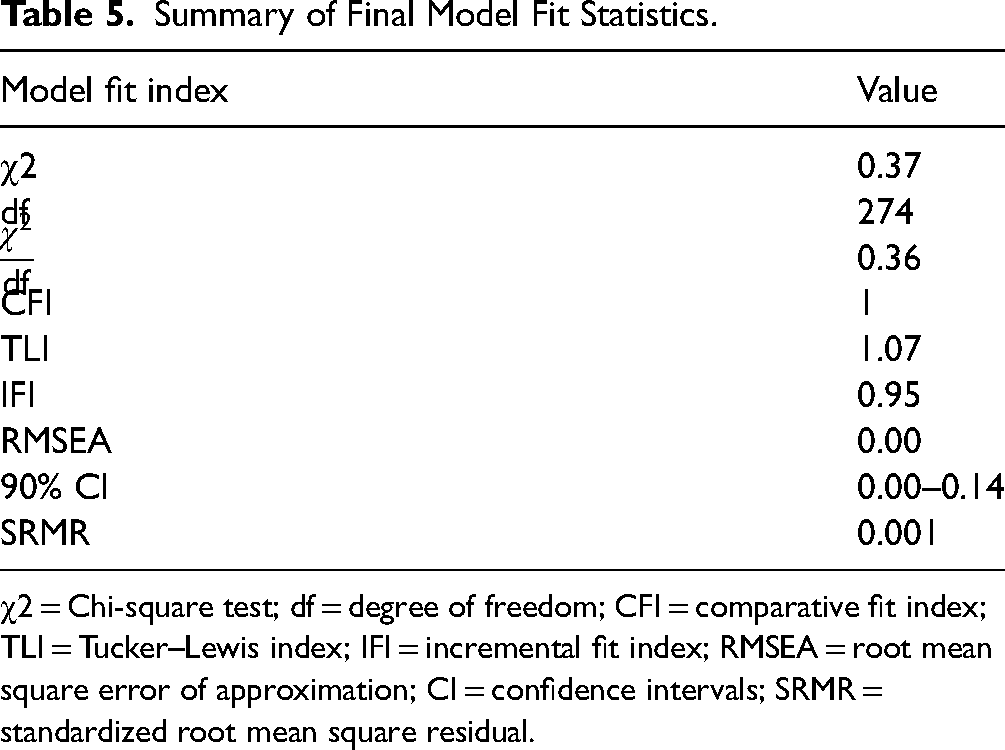
χ2 = Chi-square test; df = degree of freedom; CFI = comparative fit index; TLI = Tucker–Lewis index; IFI = incremental fit index; RMSEA = root mean square error of approximation; CI = confidence intervals; SRMR = standardized root mean square residual.
Discussion
The present study aimed to investigate medication adherence determinants in CAD patients, especially the effect of illness perception and self-efficacy. CAD is one of the most important challenges facing the health system in every country. CAD prevalence is directly related to increasing age and can affect a significant part of the population (Duncan et al., 1996). Medication adherence is the cornerstone of CAD management (Zullig et al., 2017). Medication non-adherence can cause adverse clinical outcomes. In this group of patients, such frequent admissions increased mortality (Park et al., 2015). Medication adherence is a multifactorial phenomenon and is influenced by several factors, therefore, it is important to identify these factors because non-adherence has a negative effect on the effectiveness and costs of treatment under chronic conditions with long-term treatments (Gast & Mathes, 2019; Sabaté & Sabaté, 2003). This was the first study that investigated the relationship between illness perception, self-efficacy, and medication adherence in CAD patients. Data analysis was carried out using the path analysis method that made it possible to more accurately investigate the interactions between multiple factors and thus determine the direct, indirect, and total effects of demographic, clinical, and behavioral variables on medication adherence. Results showed that more than half of the participants (61.8%) adhered to their medication regimen, which is consistent with previous studies (He et al., 2022; Pedersen et al., 2022; Silva Tinoco et al., 2021). It was also shown that greater illness perception, better self-efficacy, and higher education had a positive effect on medication adherence, and increasing age also had a negative effect on it. It is important to identify medication adherence determinants, including demographic, behavioral, and clinical variables, to improve the medication adherence status and prevent the subsequent consequences. Medication adherence can reduce the mortality rate in this group of patients by 20% within 1 year (Kulkarni et al., 2006). As we mentioned earlier, 61.8% of the participants adhered to their medication regimen. However, different degrees of medication adherence have been reported in different studies. The medication adherence rates among CAD patients were reported at 42.9% in one study (Padilha et al., 2021) and 70.9% in another one (Silva Tinoco et al., 2021). In another study, the rate of non-compliance to medication regimen in this group of patients was reported as 70% (Allahbakhshian & Gholizadeh, 2020) and in a study on patients, after cardiac angiography, only 32% of patients had a high level of adherence to the drug regimen (Allahbakhshian et al.). In another study on medication adherence in patients with chronic diseases (diabetes, hypertension, or both) in Saudi Arabia, Prabahar et al. reported that 76.44% of patients adhered to their medication regimen (Prabahar et al., 2020). Overall, medication adherence in people with chronic disorders is estimated to be approximately 50% on average (Sabaté & Sabaté, 2003). However, to achieve acceptable treatment outcomes in people with chronic diseases, the average adherence to treatment including medication adherence should be 80% or higher (Basım et al., 2021). However, differences in demographic and clinical variables and questionnaires used in previous studies may affect these results.
As mentioned earlier, greater illness perception, better self-efficacy, and higher education had a positive effect on medication adherence and increasing age had a negative effect on it. High education increases the probability of medication adherence and vice versa (Ni et al., 2019). In a study on CAD patients, Lu et al. found that people with higher education had better medication adherence (Lu et al., 2020). However, there are some studies indicating the lack of any relationship between these two variables (Shariatinia, 2018). There are several studies on the effect of age on medication adherence. Some previous studies on CAD patients showed no significant relationship between age on medication adherence (Padilha et al., 2021; Zyryanov et al., 2020). However, results of a systematic review of cancer patients treated with oral anticancer drugs showed the best medication adherence among the middle age and poor medication adherence among younger and older people (Mathes et al., 2014). Participants had a moderate illness perception (44.45 ± 3.22). Similarly, Nur et al. reported moderate illness perception among patients with ischemic heart disease (Nur, 2018).
Illness Perception and Self-Efficacy
The present study showed that illness perception had a direct effect on self-efficacy. Patients with greater illness perception had a greater ability to perform activities and behaviors related to self-efficacy. A total of 59.4% of the participants had high self-efficacy (34.06 ± 7.57). In a study on CAD patients, Barham et al. reported that the self-efficacy score was 34, which this score was at a moderate level according to the number of questions and rating scales (Barham et al., 2019). Illness perception can be effective in improving self-efficacy in chronic diseases (Mohammadi et al., 2022). The results of Mohammadi et al.'s study also confirm this relationship. They showed a significant and positive relationship between illness perception and self-efficacy in patients with type 2 diabetes, that is, patients with a greater perception of illness conditions, including the effect of the disease on their lives, had more abilities in performing activities related to self-efficacy and disease management (Mohammadi et al., 2022). However, Knowles et al. found a significant but negative relationship between these two variables (Knowles et al., 2020). Al-Amer says that the relationship between illness perception and self-efficacy can be a theoretical sequence in which illness perception can predict self-efficacy. In fact, a person's general idea about his/her illness can have a better effect on his/her self-confidence to achieve certain skills or the ability to perform self-care activities (Al-Amer et al., 2016). In their study on patients with type 2 diabetes, Kim et al., except for the two dimensions of the illness perception questionnaire, referred to other dimensions as strong predictors of self-efficacy in disease management (Kim et al., 2021a).
Illness Perception and Medication Adherence
The present study showed that illness perception indirectly affected medication in such a way that is people who perceived their illness as a serious and threatening disease had better medication adherence behaviors. Strengthening and increasing patients’ illness perception can be considered a basic strategy in educational interventions to increase medication adherence (Doust Mohammadi et al., 2018). Consistent with the present study, DoustMohammadi et al. confirmed the significant relationship between illness perception and medication adherence (Doust Mohammadi et al., 2018). Miyazaki et al. also reported in their study that illness perception is a fundamental and effective factor for medication adherence in patients with chronic diseases (Miyazaki et al., 2018). However, in a study of hypertensive patients, Saarti et al. reported that the average illness perception score was higher in people with poor medication adherence, although this study showed no relationship between illness perception and medication adherence (Saarti et al., 2016).
Self-Efficacy and Medication Adherence
The results of the present study revealed that more than half of the participants adhered to their medication regimen (61.8%) and had a high level of self-efficacy (59.4%). In this study, self-efficacy had a direct and positive effect on medication adherence. Self-efficacy can be considered an effective factor in improving self-care and CAD management (Barnason et al., 2003) and facilitating medication adherence (Martos-Méndez, 2015), which is consistent with the results of some studies. In a study titled medication adherence and predictive factors in patients with cardiovascular disease, Al-Ganmi et al. found that self-efficacy was significantly effective on medication adherence (Al-Ganmi et al., 2019). Shen et al. also found a significant and positive relationship between self-efficacy and medication adherence and referred to self-efficacy as an independent predictor of medication adherence (Shen et al., 2020). However, in a study of a group of adults with rheumatoid arthritis, McCulley et al. reported that people with higher self-efficacy had poorer medication adherence. In this study, the researchers said that the reason for this result is unclear. Still, they have speculated that patients with better self-managing skills or believing in it, so might decide not to take their medication regularly. It is also possible that the current results reflect the effect of confounding variables (McCulley et al., 2018). In a study, Daniali et al. reported no correlation between self-efficacy and medication adherence in patients with chronic disease (Daniali et al., 2017). Poor illness perception and self-efficacy at a low level can be associated with poor medication adherence (Gutierrez & Sakulbumrungsil, 2021).
Limitations of the Study
This study was cross-sectional and there is a possibility of changing people's attitudes and behaviors in the long term, which can affect the results. Since the questionnaire used in this study to investigate medication adherence also recorded the attitude of the patients towards the medication use and its side effects, the experience and attitude of the participants towards the disease-related conditions have an impact on their medication adherence. In addition, self-reported questionnaires were used to evaluate the behavioral variables, which may have influenced the study's rigor.
Recommendations
The present study evaluated illness perception and self-efficacy as two behavioral variables affecting medication adherence. Moreover, the effect of demographic and clinical variables was also investigated. However, variables such as health literacy, social support, mental health, quality of life, and other psychological, social, cultural, and spiritual factors can affect the studied variables, which are recommended to be considered in future studies. Variables that, even though they may even be identifiable, cannot be accurately controlled have not been evaluated in the present study. It seems that the participants’ attitudes and experiences of the disease, which are always personal and unique attitudes for each person, have been able to have an impact on the results of the present study. This was a cross-sectional study and the perceptions and beliefs of people with chronic disorders will change over time. Therefore, it is suggested to evaluate the patients’ illness perception in the long term and groups with a larger population, and its relationship with other variables and their effects, as mentioned earlier, should be considered because this case may increase the generalizability of the study.
Implications for Practice
Considering the importance of management and control of chronic diseases, among which medication adherence plays one of the most important roles in this field, evaluating the level of illness perception in patients and then trying to improve it and improve the abilities of patients, all of them can be effective in improving medication adherence, among which health professionals, especially nurses, due to their greater communication with patients and their active presence can play an important role in this matter by assessing the illness perception and ability of patients. In addition, the results of this study showed the effects of some demographic and clinical variables on the main variables. For example, low levels of education and increasing age are among the factors that have influenced medication adherence, as a result, nurses should focus more on this group of patients in their care and training considering these issues.
Conclusions
The present study proved the effects of the behavioral variables, that is, of illness perception and self-efficacy, on medication adherence in CAD patients. Participants had moderate illness perception, and also high self-efficacy, and more than half of the participants adhered to the drug regimen. A person's interpretation and illness perception in the face of a health threat and higher self-efficacy can affect a person's confidence in developing a specific skill or ability to change health behaviors (Lau-Walker, 2006; Schwarzer & Warner, 2013). Since the responsibility for the successful management of a chronic disease should not rest solely with the patient (Wolf et al., 2007), health professionals, especially nurses, can play an effective role in this regard. They can evaluate the patient's perception of their illness, predict their self-efficacy, and act to improve it (Lau-Walker, 2004). Nurses also can play an important role in improving medication adherence in people with chronic disorders by assessing the severity of the disease, the patient's functional status, communication systems, monitoring educational programs, strengthening health literacy, and patient awareness (Lee et al., 2017).
Footnotes
Acknowledgements
This article is the result of the master's thesis of medical surgical nursing. Hereby, the authors would like to express their thanks to the Research Vice-Chancellor of Tabriz University of Medical Sciences for funding the research, the respectful personnel of the treatment units and the patients participating in this study.
Author Contributions
Soheil Mobini: contributed to the conception of this study and gathering the data. Atefeh Allahbakhshian: contributed to the conception and design of this study and supervised the whole study process. Reza Shabanloei: contributed to the conception and design of this study. Parvin Sarbakhsh: contributed to the analysis of the data of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded and supported by Tabriz University of Medical Sciences (Grant no. IR.TBZMED.REC.1399.1031).
Institutional Review Board Approval
This study was approved by the Ethics Committee of Tabriz University of Medical Sciences (Grant no. IR.TBZMED.REC.1399.1031). All the participants in this study got information about this research including the purpose of the research and the benefits of participating in it then, if they want to participate in the study, informed consent was obtained from them and they were assured that the information that has been taken will remain confidential.
It should be noted that in the sample section, to remain anonymous, the name of the sampling location is not mentioned completely. Sampling of this study was done in cardiovascular medical and training hospital and its specialized clinic, affiliated to Tabriz University of Medical sciences.