
Abstract
Introduction
Using technology in the clinical setting where clinical alarms frequently occur, resulting in many false alarms, which is called alarm fatigue, alarm fatigue may increase nurses’ distraction, and that might negatively affect patient safety.
Objective
This study aimed to assess alarm fatigue among oncology nurses in Jordan.
Methods
A descriptive cross-sectional design was used in a non-profit specialized cancer center. A self-reported questionnaire was answered by nurses who participated in the study.
Results
A total of 222 questionnaires were analyzed with a more than 95% response rate. More than half of the sample (60.4%) were females. The participants were young nurses with a mean age of 25.18 ± 3.33 years. The total mean score of alarm fatigue was 31.62 ± 7.14 on a scale ranging from zero to 52. Post-hoc analysis showed that the palliative unit (25.73 ± 7.22) and emergency room (28.73 ± 6.62) had low scores of total mean alarm fatigue than remaining area of practice, such as the ICU (33.92 ± 6.99); p-value: .004.
Conclusion
Alarm fatigue is a global issue affecting many practice areas. An educational program is recommended for nurses to learn how to deal with alarm fatigue. In order to effectively manage alarms, nurses’ education and individual training are crucial.
Introduction/Background
Using technology for patient care, such as monitors, syringe pumps, and suction machines is an innovative treatment option. This technology would help nurses and other health care providers (HCP) monitor the physiological patients’ parameters and provide treatment and follow-up (ElKefi & Asan, 2021; Funk, 2011; Lopes, 2014). One of the aims of using the machine-related features is to alert the HCP of any health-related dysfunction through the alarms. HCPs, including nurses, are exposed to the machines’ alarms, which would be overwhelming, causing problems for patient safety and HCP due to distraction and mistrusting alarms (Lopes, 2014; Ruskin & Hueske-Kraus, 2015; Sendelbach & Funk, 2013; Yue et al., 2017).
The definition of fatigue is the inability to act. There are two types of fatigue: acute, which occurs after a rest period, and chronic, which occurs after a long period of rest (Winwood et al., 2005). A monitoring device produces excessive stimulation, leading to alarm fatigue (Sendelbach, 2012).
The Emergency Care Research Institute (ECRI) published the annual list of the top 10 Health Technology Hazards. Between 2012 and 2014, alarm fatigue was number one on the list (Bonafide et al., 2015). Approximately 1000 alarms per shift facing HCPs require neither a technical nor a clinical action. In addition, 80% and 99% of total alarms were nonactionable (Ruskin & Hueske-Kraus, 2015). A nonactionable or avoidable alarm may cause nurses to be desensitized and affect nurses’ responses, leading to delayed or inadequate responses (Bonafide et al., 2015; Vitoux et al., 2018). Inaction or delayed reaction to an alarm would affect patient life and potentially be life-threatening. The US Food and Drug Administration (FDA) has reported over 500 alarm-related patient deaths within the last 5 years (Ruskin & Hueske-Kraus, 2015). Nurses are primarily in direct contact with patients; although they face more than other HCPs patients or any technical complaints, they are more exposed to and overwhelmed by alarms (Lewandowska et al., 2020; Sowan et al., 2016).
Alarm fatigue is a patient safety risk. The risk of alarm fatigue increases when nurses cannot respond properly to one or more alarms at the same time. Alarm fatigue can lead to one or more patients losing their lives if it is not addressed (American Association of Critical-Care nurses, 2018). Sensory overload and desensitization to alarms are caused by overexposure to alarm fatigue especially in the oncology settings. It is therefore possible to miss alarms or respond to them too late. As a result, alarm fatigue has been attributed to deaths of patients when serious clinical events were missed or assumed to be false alarms.
Review of Literature
Most studies aimed to investigate the impact of alarm fatigue on nurses in acute critical care settings (Lewandowska et al., 2020; Lopes, 2014; Salous et al., 2017). So, there is a need for further studies to address the impact of alarm fatigue on nurses working in other different areas of work (Lopes, 2014). Although alarms are significant and sometimes lifesaving, they can affect patients’ safety if they are often false-positive alarms in an inappropriate setting. The issue of excessive alarms has been studied in various medical facilities in the past two decades, especially in intensive care units (Konkani et al., 2012).
The literature review was done by searching the following search engines: PubMed, Medline, CINHAL, EBSCOhost, and Google Scholar for the keywords as single or combined alarm fatigue, patient safety, nonactionable alarms, and physiologic alarm.
Baillargeon (2013) conducted a risk assessment study at medical/surgical wards in an acute care teaching hospital in Providence, Rhode Island. The results revealed that up to 52% of alarms were considered to cause alarm fatigue, and the results showed the response time was delayed by over 10 min. The author concluded that nurses were at risk of alarm fatigue based on a high frequency of alarms, an increase of false, nuisance, technical and valid alarm, and delayed responses resulting in mistrust of alarms. Finally, the study recommended an educational program for nurses about managing machine settings, time management, and health patient education to reduce the number of alarms exposed (Baillargeon, 2013).
An observational study was conducted in the children's hospital of Philadelphia, Pennsylvania, to find the relationship between nurses exposed to a high non-actionable physiological monitor alarm and time of response to a critical alarm. In the study, 36 nurses were observed for 210 h, with 5070 alarms. The results showed that 99% of alarms in the medical ward and 87% in pediatric intensive care unit alarms were non-actionable. The authors concluded that if non-actionable alarms increase, it will lead to a delayed response that would affect patient care, considering the excessive number of non-actionable alarms were alarm fatigue (Bonafide et al., 2015).
In another observational study conducted by Drew et al. in 2014, in 31 days period for a total of 461 ICU patients, authors observed arrhythmia alarms to discover the alarm fatigue; the observation was computerized and recorded for all bed monitoring. The results showed that 2,558,760 special alarms, such as arrhythmia, were distributed as 1,154,201; “parameters, 612,927”; “technical, 791,632” and “381,560 audible alarms”. Around 88.8% of the 12,671 annotated arrhythmia alarms were false positive, which means inappropriate use settings caused alarms; 93% of the 168 true ventricular tachycardia alarms were not sustained long enough to warrant treatment. The authors concluded that adjusting the setting may decrease the number of alarms, and decreasing the number leads to decreased alarm fatigue (Drew et al., 2014).
Pergher and da Silva (2015) conducted a mixed-method study of 14 beds of adult ICU in a military hospital in Rio de Janeiro, Brazil. The study investigated the cause of the invasive blood pressure alarms and nurses’ response time. The data was collected using the structured observation technique in 60 h of observation; they recorded 76 invasive blood pressure alarms. The results revealed upon response time as 28% of alarms were at average time response (2.45 min). In comparison, 72% of alarm the time response was 10 min and considered alarm fatigue. The author defined alarm fatigue according to response time as every alarm that didn't respond within 10 min will be alarm fatigue (Pergher & Da Silva, 2015).
Sowan et al. (2016) implemented a quality improvement project to inspect the effectiveness of changing alarm default settings and educational interventions for nursing staff in reducing alarm fatigue. The project included 20 transplant/cardiac ICU beds with 39 nursing staff. They used several interventions, such as educating nursing staff in the cardiac ICU unit on the appropriate use of the monitors and changing the default settings of some parameters on the monitors based on recent evidence and scientific clinical rationale. The results revealed that standard in-service education on cardiac monitor use and changing default alarm settings is not enough to enhance alarm system safety (Sowan et al., 2016).
Alarms management in ICUs is very complicated, involving the availability of unit procedures and policies, alarm management practices by nurses and clinicians, unit design, usability and complexity of monitoring devices, and the adequacy of training on system use. The study suggested that multidimensional interventions are required to achieve and improve alarm systems safety (Sowan et al., 2016).
A systematic review indicates alarm fatigue is prevalent and severe in developed countries (Cvach, 2012); the FDA reports 566 deaths related to monitor alarms every year (Andrade-Méndez et al., 2020).
Several studies have reported the effectiveness of certain interventions in improving alarm systems safety (Bach et al., 2018; Bell & Cox, 2010). Some of these interventions assess the incidence of false-positive alarms and nuisance within the unit environment. They developed a hospital or unit policy regarding appropriate parameters for setting alarms tailored to a specific patient's needs. Reviewed units’ default alarm settings for appropriateness to patient population and arranged for adjustment as required. Also, the intervention was to determine if a defined alarm response time must be included in the monitoring policies and protocols (Bell & Cox, 2010).
The current study aimed to assess alarm fatigue among oncology nurses in Jordan. This study includes two research questions “What is the prevalence of alarm fatigue among nurses in a specialized oncology center in Jordan?” and “Is there a relationship between the area of work and alarm fatigue?”
Methods
Design
A descriptive, cross-sectional design was used in this study. This design is suitable to meet the objectives of this exploration and correlational study.
Sample
A convenient sample of nurses who met the following inclusion criteria was included in the study: registered nurses with more than 3 months of experience; during the first 3 months, the nurse is still in the preceptorship period. There was no restriction on the sample size once it met the inclusion criteria. A minimum of 214 participants was needed to achieve 80% power with an alpha of .05.
Inclusion/Exclusion Criteria
A convenient sample of nurses who met the following inclusion criteria was included in the study: registered nurses working in the cancer center in Jordan with more than 3 months of experience. We choose 3 months of experience because, before 3 months of experience, the nurse is still in the preceptorship period.
This study was conducted in one of the comprehensive accredited cancer centers in the Middle East, treating both adult and pediatric patients with cancer. It has 180 beds and covers more than 60% of Jordanian patients with cancer.
Instruments
Data collection was conducted using a two-part questionnaire.
Torabizadeh et al. (2017) granted the instrument's validity. The questionnaire was revised and validated by a panel of 10 experts; the authors had the questionnaire analyzed by several professors in the fields of anesthesiology, intensive care, and nursing, as well as some experienced head nurses and nurses in intensive care units. All of them were familiar with the concept in question. Several anesthesiologist professors and some experienced nurses in intensive care, such as head nurses, analyzed the questionnaire. They were familiar with questionnaire concepts. The questionnaire needs 10 min to complete (Torabizadeh et al., 2017). Researchers used the test-retest approach to assess the reliability. The internal consistency was perfect; Cronbach's alpha (α) was 0.91 (Torabizadeh et al., 2017).
Ethical Consideration
The ethical approval to conduct this study was obtained from the institutional review board. The Principal investigator explained the purpose of the study to the participants. The questionnaire had a cover letter ensuring that the survey was anonymous and no identifiers were required. In addition, this cover letter was read by the participants before answering the questionnaire. They answered the questionnaire and returned it; this was considered consent to participate in the study. Only aggregated data were used for publication purposes.
Statistical Analysis
Data were analyzed using the Statistical Package for the Social Sciences (SPSS) version 21. All data were coded, then the outliers were checked, and the data analysis was performed as follows: Descriptive statics (i.e., frequency, percentage, mean, and standard deviation) were used to describe the sample characteristics. T-test and analysis of variance (ANOVA) tests were used to check if there was any difference among the areas of work regarding the sample characteristics according to the level of measurement.
Results
A total of 222 questionnaires were analyzed, with a more than 95% response rate. Most of the participants were females (60.4%), and the mean participants’ age was 25.18 ± 3.33. Most of them (97.3%) had a bachelor's degree in nursing. The study was conducted in ICU, pediatric, emergency room (ER), bone marrow transplant (BMT), medical/surgical, leukemia, palliative, and very important person unit (VIP). Other demographic characteristics of the participant are presented in Table 1.
Participants’ Demographics.

Total Alarm Fatigue Scores Among Nurses
The total mean alarm score was 31.62 (7.14) on a scale ranging from zero to 52, which is a high-impact level of alarm fatigue assessed among oncology nurses. The mean scores for all items were above 2, item 13, “At visiting hours, I pay less attention to the alarms of the equipment,” got the highest mean score of 2.83 (1.06) (Table 2).
Descriptive Statistics for Nurses’ Alarm Fatigue.

Demographic Differences in Total Fatigue Score
ANOVA and t-tests were performed to check if there was any difference among the gender, education, and areas of work regarding the sample characteristics according to the level of measurement. There are no significant differences between gender and education with total fatigue score (p-value > .05) (Table 3).
Demographic Differences in Total Fatigue Score.
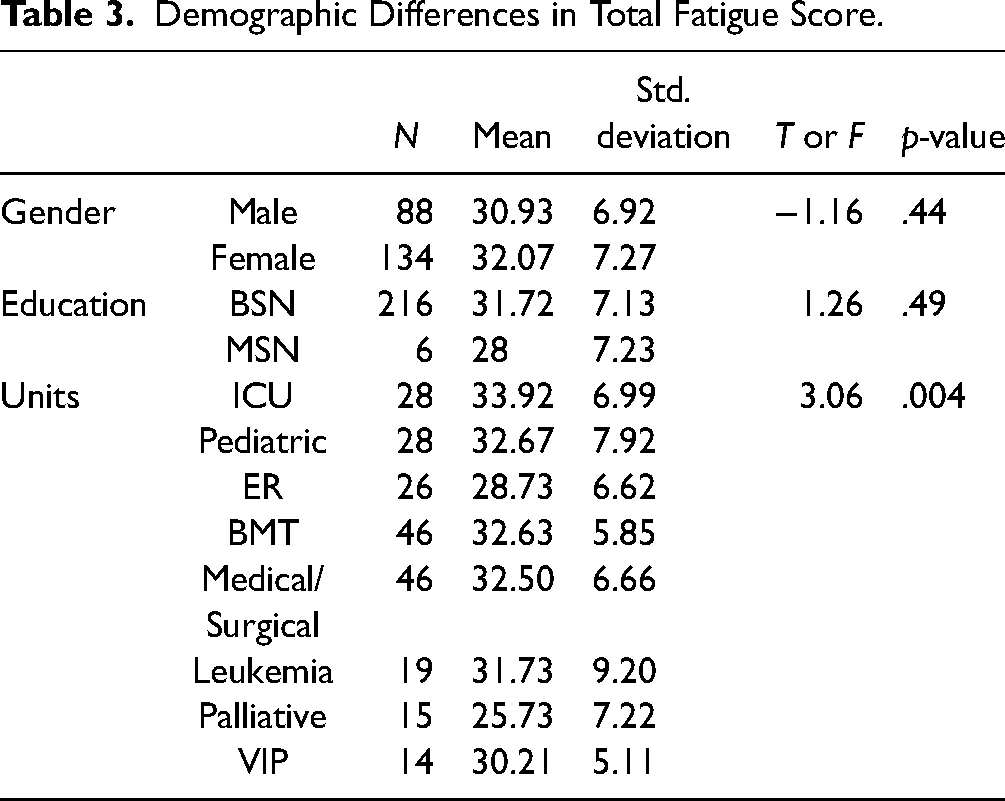
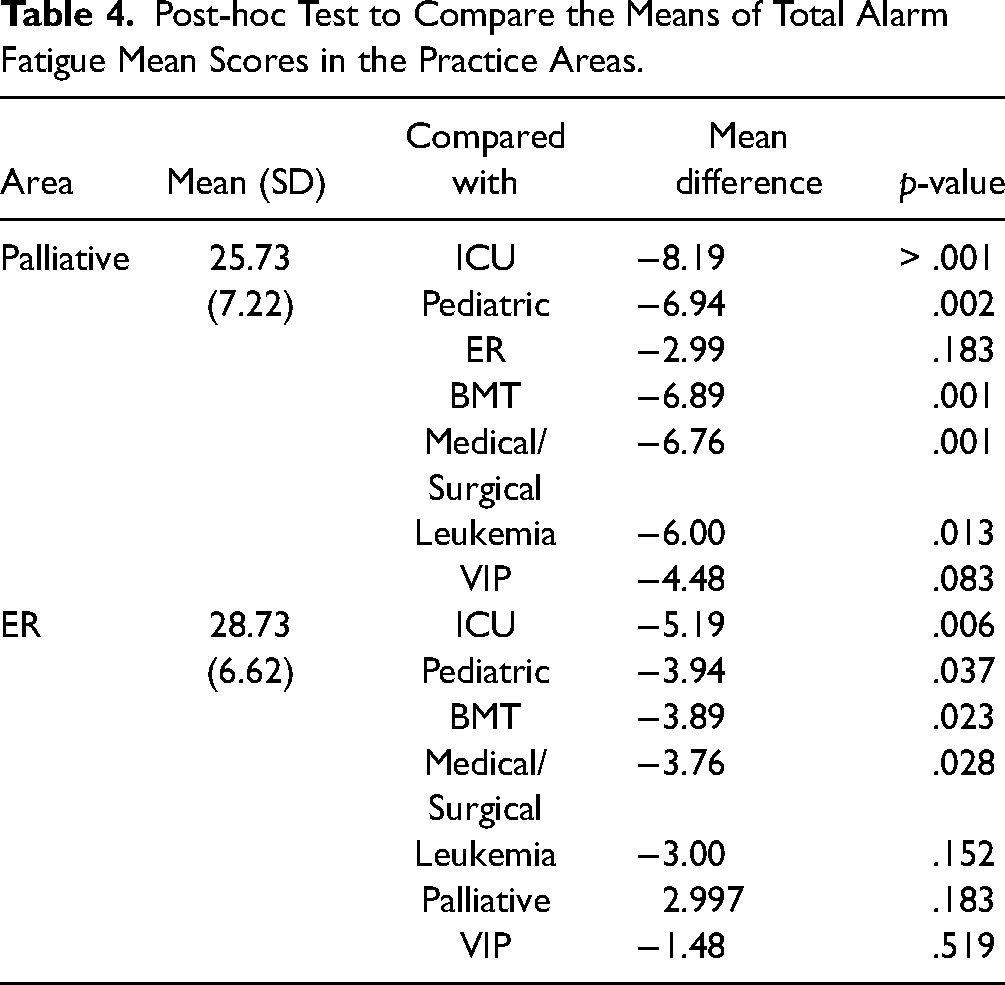
ANOVA with post-hoc test was performed to compare the means of total alarm fatigue mean scores among the practice areas. There was a significant difference in total mean alarm fatigue scores among the practice areas. Post-hoc analysis showed that the palliative unit (25.73 ± 7.22) and ER (28.73 ± 6.62) had low scores of total mean alarm fatigue than remaining area of practice, such as the ICU (33.92 ± 6.99); p-value: .004 (Table 4).
Post-hoc Test to Compare the Means of Total Alarm Fatigue Mean Scores in the Practice Areas.
Discussion
Alarm fatigue is a common problem worldwide, which might affect nursing work and patient care. In the literature, the impact of alarm fatigue at ICUs was the highest. Limited information was found about alarm fatigue among Jordanian nurses. So, the current study aimed to assess alarm fatigue among oncology nurses in Jordan.
A high score of alarm fatigue was found among Jordanian nurses working at the oncology center. The result showed the highest scores of alarm fatigue recorded in the ICU, which is supported by many previous studies that showed a high score of alarm fatigue in ICUs (Drew et al., 2014; Pergher & Da Silva, 2015; Sowan et al., 2016). However, this finding can delay timely care or desensitize health personnel, threatening patient safety and potentially leading to fatal outcomes (Andrade-Méndez et al., 2020). Moreover, excessive alarms can result in important alarms going unnoticed and intercurrences going unnoticed. As a result of noise, health workers may be stressed, burnt out, and experience conflict, while patients may develop insomnia, and require anxiolytics and analgesics for pain management (Bridi et al., 2014). On the other hand, both units palliative and ER reported lowered alarm fatigue scores. That might be for several reasons; the use of intravenous medication in most cases in the ER and palliative is less than in other units, leading to the limitation in using the pump machine. In addition, using a cardiac monitor in the ER is a temporary time because the patient under observation stays a short time at the ER and would be transferred as soon as possible to another unit. While in palliative care, few patients need close monitoring or the use of cardiac monitors. Moreover, the ER is more centered on reanimation interventions, ongoing evaluation, and intervention based on the assessment; and other comfort interventions in palliative care.
In this study, the low score of alarm fatigue is shown in the palliative unit and ER regarding the total mean alarm fatigue than the remaining area of practice. But in the literature, there are no studies reported for both units to assess alarm fatigue; in this study, alarm fatigue was evaluated in more units, such as ICU, BMT, pediatric, VIP, medical/surgical, leukemia, palliative, and ER; the medical/surgical also reported high score alarm fatigue, and this is supported in previous studies (Baillargeon, 2013; Bonafide et al., 2015). A typical shift on the medical/surgical floor may see up to 1,000 alarms (Ruskin & Hueske-Kraus, 2015). It is important to note that alarms can be triggered by generic device settings or malfunctioning electrodes. According to experts, 85% to 99% of alarms do not need to be addressed (Patient Safety Advisory Group, 2013).
An educational intervention, an organizational intervention, and a technical intervention can all be used to address alarm fatigue. It is possible to reduce the number of nuisance alarms experienced by healthcare workers by selecting only the right monitors (not over-monitoring), selecting alarm limits carefully, and implementing multimodal alarms (Ruskin & Hueske-Kraus, 2015).
The nurses rated the visiting hours could disturb them so that they could pay less attention to the alarms of the equipment. Consequently, the nursing staff can feel exhausted with an excessive number of duties and clinical alarms constantly coming in. Therefore, it is necessary to arrange the visiting hours and an effective alarm management strategy should be introduced.
Strengths and Limitations
An educational program is recommended for nurses on how to deal with alarm fatigue, such as managing the setting of machines and educating the patient about nurse calls and how it is crucial. In addition, frequency checks of the machine calibration in the unit in addition to maintenance and biomedical engineering. After finishing each machine, the storekeeper of the unit calibrates the machine and keeps it ready to use. According to guidelines published by the American Association of Critical-Care Nurses in 2013, alarms should be handled according to specific procedures. As part of the recommendations, induction and continuous training was suggested (American Association of Critical-Care Nurses, 2013). In order to effectively manage alarms, nurses’ education and individual internships are crucial.
The current study has many limitations, such as using a convenient sample method, conducting the study in one hospital, and using a self-reported questionnaire.
Conclusion
Alarm fatigue is a global issue affecting many practice areas. There is a high-impact level of alarm fatigue assessed among oncology nurses, and it seems to be more impact of alarm fatigue in the ICU. However, the palliative unit and ER had less impact on alarm fatigue.
Oncology settings have their own unique circumstances that require alarm management strategies to be tailored to be realistically implemented. It requires an integrated system approach and in-depth planning and analysis of the alarm management process to improve alarm management.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Consideration
Institutional Review Board (IRB) approval was obtained from the King Hussein Cancer Center.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article