
Abstract
Introduction
Given the vital nature of their profession, ICU nurses endure significant psychological and physical stress. Burnout, low job satisfaction, and deteriorated patient care might result from the high-stress atmosphere.
Objectives
This study aims to assess the level of alarm fatigue and stress among nurses who work in acute care units.
Methods
A descriptive design was used to recruit nurses in acute care units. A self-administered questionnaire was used to collect the required data composed of three parts, namely demographical data; the alarm fatigue part, which was created by Torabizadeh et al. and composed of 13 items, and the perceived stress scale (PSS) which is a psychological diagnostic instrument created to assess how much people find their daily lives to be stressful. It was created by Cohen et al. and composed of 10 items.
Results
An average age of (35.3 ± 6.24) years, and an average number of years of experience of (7.63 ± 5.56), were found among the 128 nurses that were recruited. Acute care nurses had a significant degree of alarm fatigue, as indicated by the overall alarm fatigue score of (M = 30.1 ± SD = 7.47). A moderate degree of stress was also indicated by the overall perceived stress score, which was (M = 21.5 ± 5.02). Among nurses, alarm fatigue and felt stress are not correlated with any demographic feature, including sex, educational attainment, marital status, and working location.
Conclusion
Stress and alarm fatigue are serious problems for acute care units that can jeopardize nurse and patient safety. The implementation of methods that mitigate alarm fatigue and stress, such as alarm customization, adequate staffing, and support systems, can enhance the work environment in acute care units. Healthcare companies can raise the grade of care provided to patients and enhance the general well-being and job satisfaction of their nursing staff by addressing these challenges.
Introduction
Nurses in acute care units use cutting-edge technology and creative devices like electrocardiogram (ECG/EKG) monitors, invasive hemodynamic monitors, and ventilator monitors to keep an eye on changes in patients’ physiologic and hemodynamic conditions (Ali Al-Quraan et al., 2023). Medical equipment alerts are common in hospital settings (Lewandowska et al., 2020). Since alarm management is utilized to continuously monitor admitted patients in acute care units, it plays a key part in the everyday responsibilities performed by nurses (Dehghan et al., 2023). However, the Alarm sound generated from the medical monitors is excessive and needs frequent assessment and in most cases, it needs no intervention (Lewandowska et al., 2023). In clinical practice, a high percentage of false alarms remains a challenge to solve that leads to overwhelming and excessive fatigue of healthcare providers, including nurses (Storm & Chen, 2021). Alarm fatigue is a term used to describe the sensory overload and desensitization that prevent nurses from reacting appropriately to actual threats (Simpson & Lyndon, 2019). One of the primary causes of safety incidents, which can pose major hazards, is a lack of situational awareness of alert noises (Storm & Chen, 2021).
Nurses respond to a lot of alarms during their shifts, ranging from 150 to 400 alarms for a single patient. This can take up to 35% of their time at work in their units (Lewandowska et al., 2020). Nurses may experience sensory overload and burnout as a result of trying to determine whether an alarm is relevant amidst the deafening din of machinery. Alarm fatigue and general workplace stress are significantly increased by the simple process of recognizing, assessing, and validating an alarm—even in situations where no action is necessary (Simpson & Lyndon, 2019).
Alarm fatigue is becoming a more significant global public health issue that compromises patient safety (Nyarko et al., 2023). It is reported that alarm fatigue causes a delayed response to alerts and the failure to notice genuine emergencies, both of which could endanger patient health (Lewis & Oster, 2019). Changing tracking alarm settings to meet a particular patient's needs, also known as customizing, individualizing, or changing alarms is one way to reduce the frequency of alarms and improve their value for patient safety. Excessive alarms are a main challenge among nurses that is difficult to deal with in clinical practice (Lewandowska et al., 2020).
Review of Literature
Sounds generated from medical alarms are classified as the top 10 health technology hazards as reported by Emergency Treatment Research Institute in 2020 (Top, 2019). Furthermore, it was reported that 72%–99% of the alarm sounds that are generated in ICUs are false-positive alarms (Clifford et al., 2016). Nurses experience sensory overload when they are overexposed to false-positive alarms that arise without reliable physiological data violations, which reduces their sensitivity to alarms (Dehghan et al., 2023), leading them to overlook these alerts, endangering their patients and impairing their quality of life (Oliveira et al., 2018). Along the same line, a study was performed by Cho et al. (2016) to examine the state of clinical alarms in the ICU, the degree of alarm fatigue experienced by nurses in connection with clinical alarms, and the challenges associated with alarm management. A long 48 h of observation resulted in a total of 2,184 clinical alarms, or 45.5 alarms per participant each hour. Sixty-eight (1,394) of these alarms were classified as false alarms. Out of 35, the alarm fatigue score was 24.3 ± 4.0. Also, a systematic review conducted by Lewandowska et al. (2020) included seven studies to assess the perception of nurses about the clinical alarm and its impact on the ICU environment. Acute care nurses believe that alarms are annoying and occur too frequently, interfering with patient care and eroding their confidence in alarm systems. With an excessive number of responsibilities and a constant barrage of alarms, they feel overworked.
In addition to elucidating the relationship between alarm fatigue and mental workload among nurses in ICUs, a study performed by Seok et al. (2023) sought to ascertain the level of alarm fatigue and mental workload experienced by ICU nurses. A descriptive, cross-sectional design was adopted. A questionnaire was used to gather information from 90 nurses working in four acute care units in Seoul, Republic of Korea, on their level of alarm fatigue and mental workload. Out of 44, the average alarm fatigue score was 28.59. With a score of 3.59 out of 4, the item with the highest score was “I often hear a certain amount of noise in the ward.” In addition, 75.21 out of 100 was the average score for mental workload. The item with the highest mental exertion, effort, had a score of 78.72 out of 100. Nonetheless, studies to lessen alarm fatigue and create suitable standards are required because it can impair productivity. It was not registered for this study.
Worldwide, several studies were conducted to assess the effect of alarm fatigue among healthcare providers to reduce the effect of alarms on nurse's psychological, physiologic, and technical status. In Jordan, a study was performed only among oncology nurses to assess the level of alarm fatigue (Ali Al-Quraan et al., 2023). Studies on elucidating the relationship between alarm fatigue and stress among nurses in the ICU are lacking. Addressing alarm fatigue is critical for ensuring patient safety, enhancing the quality of care, and supporting the well-being of nurses and other healthcare providers. It requires a multifaceted approach that involves technological, organizational, and educational interventions (Hani & Ahmad, 2023). To enhance patient outcomes and deliver high-quality care in the acute care unit, it is crucial to comprehend not just the degree and contributing elements of alarm fatigue but also its effects on nurses, including their stress levels. Hence, this study aims to assess the level of alarm fatigue and stress among nurses who work in acute care units.
Methods
Design
A descriptive, cross-sectional design was used.
Research Questions
The following research questions will be addressed in the current study:
What is the extent of alarm fatigue and stress in the acute care units among nurses? Is there a relationship between alarm fatigue and nurse's perception of stress in the acute care units? Are there significant differences among demographical characteristics, total fatigue score, and perceived stress score?
Settings and Sampling
This study was conducted in governmental hospitals in the Northern regions of Jordan in 2024. Five governmental hospitals were included in this study which have one acute care unit cardiac care unit, and emergency department in each one. These hospitals were Princess Basma Teaching Hospital which was established in 1956 with 237 total beds and an occupancy rate of 86.0%, and King Abdullah University Hospital (affiliated with Jordan University of Science and Technology) was located in Irbid Governorate the second-largest city in Jordan that has total beds of 2,431 and occupancy rates of 95.0%; Ajloun Governmental Hospital that is located in Ajloun Governorate that established in 1998 with total beds of 60 beds and an occupancy rates of 35.2%; Jerash Governmental Hospital located in Jerash Governorate that serves the area along with other smaller facilities that was established in 1967 with a total beds of 125 and an occupancy rates of 57.4%; and Al-Mafraq Governmental Hospital in Al-Mafraq governorate that was established in 1967 with total beds of 55 and an occupancy rates of 57.8% (MOH, 2020).
Inclusion/Exclusion Criteria
The target population was all acute care nurses. However, the accessible population are the nurses who worked in acute care units who met the following inclusion criteria (1) have at least 6 months of work experience in acute care units or emergency departments to ensure that participants have enough exposure to the ICU environment and alarm systems to provide relevant and reliable data, (2) employed in acute care units, cardiac care units, and emergency department, (3) agreed to participate in this study. Implied informed consent was applied since the nurse who agreed to fill out the questionnaire is considered implicitly as an agreement to be a participant in the current study. Convenience sampling was used to recruit the required sample for the current study. According to the G*Power, using a statistically significance α = .05 and β value of .8 (Faul et al., 2009), the estimated sample size is 111 participants. However, to overcome the problem of decreased response rate and attrition rate it was increased to include 128 participants. Data collection was started on December 12, 2023 and finished by March 12, 2024.
Instruments
A self-administered questionnaire was used to collect the required data composed of three parts; (1) demographic characteristics of nurses including age, sex, years of experience, marital status, educational level, and number of children (if any). The second part is the alarm fatigue part which was created by Torabizadeh et al. (2017). The questionnaire is composed of 13 items with a range score between 8 (minimum) and 44 (maximum), with higher scores indicating a greater impact of alarm fatigue on nurses’ performance. Each item on the questionnaire is scored from 0 to 4, except Items 1 and 9 which are scored reversely. The item “never” on the questionnaire is always scored 0 and the item “always” is scored 4, except Items 1, and 9 which are scored reversely. In general, 11 items are scored out of 4, the total being 44; and two items are scored reversely, meaning the possible maximum is 0, so the possible maximum score is 44. On the other hand, if a respondent gets 0 for the positively scored items and 4 for the reversely scored items, then the total will be 8, that is, the minimum. Higher scores indicate a greater impact of alarm fatigue on nurses’ performance. If a respondent selects “never” for Items 1 or 9, it is scored 4 and it means a great impact of alarm fatigue, but “always” for Items 1 and 9 is scored 0 and it means that the responding nurse acts rightly.
To ensure the tool's cultural and linguistic validity, a rigorous translation and back-translation process was conducted. Initially, the tool was translated from English to Arabic by a bilingual expert fluent in both languages and familiar with the subject matter—this forward translation aimed to maintain the items’ conceptual equivalence. Following the translation, a separate, independent bilingual expert, who was blind to the original version, performed a back-translation of the Arabic version into the original language. The questionnaire shows a Cronbach's alpha of .91, a test-retest correlation coefficient of .99, and a Guttman split-half correlation value was .79. The study's findings demonstrate that the alarm fatigue scale designed for nurses can be measured with a valid and trustworthy questionnaire (Handan et al., 2021; Wunderlich et al., 2023).
The third part is the perceived stress scale (PSS) which is a psychological diagnostic instrument created to assess how much people find their daily lives to be stressful. It was created by Cohen et al. (1983). The PSS typically consists of statements regarding thoughts and feelings related to stress. It is a self-report questionnaire using a 5-point Likert scale, where 0 represents never and 4 represents very often, respondents are asked to indicate how much they agree or disagree with each statement. The scale has 10 items that ask respondents about how unpredictable, unmanageable, and overburdened they believe their lives to be. The responses to each item on the PSS are added up to produce a final score. Higher total scores, which can range from 0 to 40, indicate perceptions of greater stress. An increased overall score is typically regarded as a greater experience of stress. Scores ranged from 0 to 13 indicating low stress level, while from 14 to 26 considered moderate stress, and from 27 to 40 considered high perceived stress level. According to Cohen and Williamson, PSS-10 scores showed acceptable internal consistency reliability of .78 and moderate concurrent criterion validity concerning the amount of stress experienced on average during a week (r = .39, p < .05) (Baik et al., 2019).
Ethical Considerations
The institutional review board granted its ethical approval from Irbid National University (#001/2023) and the Ministry of Health (ERC #: 115/2024) to be carried out. The nurses were given an explanation of the study's purpose by the researchers. The survey included a cover letter guaranteeing that no identifying information was needed and that the survey was anonymous. Before responding to the questionnaire, the participants also read this cover letter. Their completion and return of the questionnaire constituted their agreement to participate in the study and it was considered as implied informed consent for their agreement to participate in the study.
Statistical Analysis
Statistical Package for the Social Sciences (SPSS), Version 25 was used to analyze the data. Following the coding of all the data and the verification of the outliers, the data analysis was carried out as follows: Frequency, percentage, mean, and standard deviation are used for descriptive statistics. The analysis of variance (ANOVA) test and the t-test were used to determine whether there were any differences in the sample characteristics according to the level of measurement between the areas of work. Besides, Pearson product-moment correlation was used to assess the relationship between alarm fatigue and stress among nurses in ICUs.
Results
Sample Characteristics
A total of 128 acute care nurses were recruited in this study. The mean age of nurses was (M = 35.3, SD = 6.24) with an average of (M = 7.63, SD = 5.56) years of experience. Most nurses have a bachelor's degree (n = 104, 81.3%) with around half participants working in ICU (n = 62, 48.4%). Most participants were married (n = 106, 82.8%).
Total Alarm Fatigue Scores Among Nurses
The total alarm score has an average of (M = 30.1, SD = 7.47) which reflects a high impact of alarm fatigue among nurses who worked in acute care units. The lowest average of alarm fatigue items was in Item # 2 “I turn off the alarms at the beginning of every shift (M = 1.49, SD = 1.45” while Item # 8 “Alarm sounds make me nervous” (M = 3.05, SD = 1.05; Table 1).
Descriptive Statistics for Nurses’ Alarm Fatigue (n = 128).

Note. M = mean, SD = standard deviation.
Total PSS Scores Among Nurses
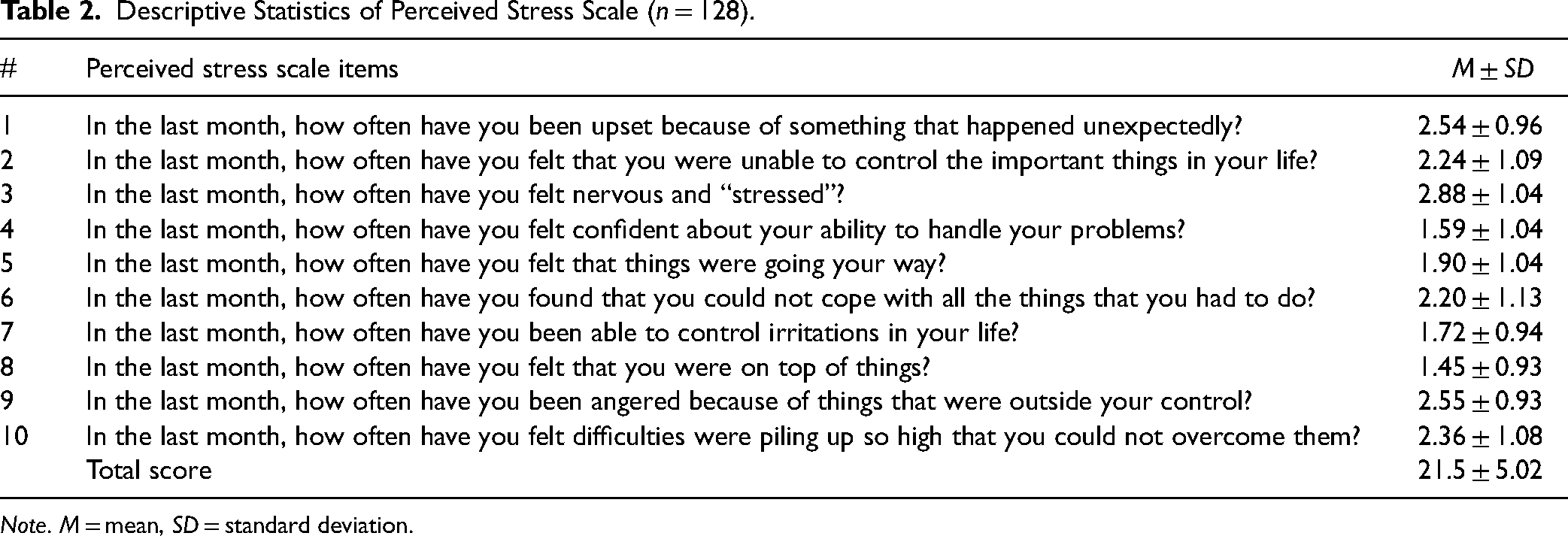
The total mean score of the PSS was (M = 21.5, SD = 5.02) on a scale ranging from 0 to 4, indicating a moderate level of perceived stress. The lowest mean score was revealed in Item # 8 “In the last month, how often have you felt that you were on top of things?” with an average of (M = 1.45, SD = 0.93), while the highest average of stress among nurses was in Item #3 “In the last month, how often have you felt nervous and ‘stressed?’” with an average of (M = 2.88, SD = 1.04) followed by Item # 9 that is “In the last month, how often have you been angered because of things that were outside your control?” with an average of (M = 2.55, SD = 0.93; Table 2).
Descriptive Statistics of Perceived Stress Scale (n = 128).
Note. M = mean, SD = standard deviation.
Independent sample t-test and ANOVA were performed to verify the presence of a significant difference between demographics of sex, marital status, educational level, unit of work, and total alarm fatigue. It was found that there was no significant difference between sex, marital status, level of education, and working area (p < .05; Table 3).
Demographic Differences in Total Fatigue Score.

Note. P is significant at .05.
Similarly, t-tests and ANOVA were performed to assess the significant differences between the demographics of nurses and the total score of the PSS. It was found that there was no significant difference between sex, marital status. educational level, and working area (p < .05; Table 4).
Demographic Differences in Perceived Stress Sacel.

Note. P is significant at .05.
Finally, the Pearson correlation was run to assess the association between the total fatigue score and the PSS. It was revealed that there was a significant positive correlation between both scales (r = .046, p < .001).
Discussion
This study highlights the level of alarm fatigue and stress among nurses who work in acute care units. Alarm fatigue is acknowledged as a concerning issue in medical settings, such as acute care units, where nurses are regularly exposed to a variety of alarms from monitoring equipment. Medical staff who experience alarm fatigue become less vigilant as a result of too many alerts, which could jeopardize patient safety (Lewandowska et al., 2020).
In this study, it was found that nurses had a high level of alarm fatigue in the acute care unit which was consistent with several studies that show a high level of alarm fatigue among oncology Jordanian nurses in the study conducted by Ali Al-Quraan et al. (2023) who revealed a high level of alarm that reached (M = 31.62, SD = 7.14). Similarly, a study performed by Cho et al. (2016) found that the alarm fatigue score was (M = 24.3 ± 4.0 out of 35). Similarly, a study performed by Yahyaei et al. (2023) who conducted a cross-sectional survey among 308 acute care nurses found moderate alarm fatigue among nurses. However, this finding could threaten patient safety since many nurses reported that they get off the alarms at the beginning of the shift and go unnoticed by excessive alarms. Besides, many nurses reported that alarm sounds make them nervous which is associated with high levels of stress, burnout, and fatigue. Simultaneously, patients experience overwhelming alarms that interfere with their sleep. These results aligned with a systematic review by Lewandowska et al. (2020), which found that a large number of nurses felt that alarms were burdensome and too frequent, interfering with patient care and decreasing public trust in alarm systems.
Additionally, in the current study, it was found that no significant differences between total scores of alarm fatigue and perceived stress including sex, educational level, marital status, and working areas. This finding is not consistent with the findings of a study performed by Yahyaei et al. (2023) that revealed a significant difference among females working as compulsory medical service workers and assigned to variable shifts, and those required to work mandatory overtime reported higher degrees of alarm fatigue. In this study context, alarm fatigue is not influenced by these demographic factors. Other aspects like workload, specific unit conditions, or individual coping mechanisms might still play a role.
This study revealed a positive correlation between alarm fatigue and perceived stress among nurses who worked in acute care units. This finding was consistent with a study performed by Nyarko et al. (2023) who reported that alarm fatigue was positively associated with emotional exhaustion and depersonalization. On the other hand, this finding was inconsistent with a finding found by Nyarko et al. (2023) who reported that there was no discernible relationship between mental workload and alarm fatigue. Although alarm fatigue was a common occurrence for nurses, it was not directly associated with their mental burdens. This may have been because of their professional consciousness as they continued to perform their tasks despite alarm fatigue.
Strengths and Limitations
Several advantages to studying and investigating alarm fatigue in acute care units among nurses, which add to the comprehensiveness and reliability of the study. Addressing a critical issue in healthcare settings, where alarm fatigue can have serious consequences on patient safety. The findings of this study have direct implications for improving patient care in acute care units. However, utilizing a self-reported questionnaire in conjunction with a convenience sample approach was considered a possible limitation of this study.
Implications for Practice
In light of the findings of the present study, it is strongly recommended that stakeholders within the Ministry of Health in Jordan undertake the development and execution of comprehensive training initiatives tailored for healthcare professionals, with a specific emphasis on nurses operating within acute care units. These training programs should be designed to augment the participants’ understanding of alarm fatigue and stress management. Integral components of such programs should encompass instruction on optimal alarm prioritization, response strategies, and the integration of coping mechanisms. The overarching objective is to alleviate the detrimental consequences associated with prolonged exposure to alarm-related fatigue. This academic recommendation underscores the imperative for targeted educational interventions to enhance the preparedness and resilience of healthcare professionals in acute care settings.
Conclusion
Alarm fatigue is a widespread problem that impacts nurses who work in acute care units. Nurses exhibit a high impact degree of alarm fatigue and stress levels with a greater tendency to occur in the acute care units. Healthcare professionals can raise nurse well-being, increase patient safety, and influence policy by knowing this relationship. The findings of the study can direct future investigations into creating efficient treatments and utilizing technology breakthroughs to lessen alarm fatigue and the tension that goes along with it. In the end, our research helps to build a hospital environment that is safer, more effective, and encouraging for both patients and medical staff.
Key Points
Alarm management plays a significant role in nurses’ daily tasks since it is used for continuous monitoring of admitted patients in acute care units
Among acute care nurses, a high level of alarm fatigue was influenced by the overall alarm fatigue score. Furthermore, a moderate amount of stress was indicated by the overall perceived stress score.
Training programs should be designed to augment the nurse's understanding of alarm fatigue and stress management
Footnotes
Acknowledgment
The authors would to thank all nurses who participated in this study.
Author Contributions
SBH: conceptualization, data collection, analysis, and writing. EAAA: final drafting and data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Institutional Review Board (IRB) approval was obtained from Irbid National University (#001/2023).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.