
Abstract
Antenatal care (ANC) is a critical period for promoting the health of both mothers and babies. ANC visit is a key entry point for a pregnant woman to the health care system to receive health intervention. The new World Health Organization (WHO) guideline recommends eight ANC contacts. However, the coverage of at least four ANC visits is still low in the Simiyu region.
Objective
To assess determinants of focused ANC visits utilization among women in the Simiyu Region Tanzania.
Methodology
The study employed a cross-sectional study among women of reproductive age. Data was collected through an interviewer-administered questionnaire and analyzed using Stata version 15. Data were summarized using mean and standard deviation for continuous variables while frequency and percentage were used for categorical variables. A generalized linear model, Poisson family, with a log link was used to identify determinants of focused ANC utilization.
Results
All 785 women analyzed reported having at least one ANC visit, with 259 (34%) having four or more visits and only 40 (5.1%) having eight or more visits. Women who made a self-decision were 30% less likely to complete four and more ANC visits than their counterparts (APR = 0.70; 95%CI = 0.501–0.978). Women who visited the dispensary were 27% less likely to complete four ANC visits than those who visited health centers (APR = 0.73; 95%CI = 0.540–0.982). However, education level and planned pregnancy were both marginally significantly associated with focused ANC utilisation.
Conclusion
Generally, the majority of pregnant women in the Simiyu region do not adequately utilize four and more ANC visits. There is a need to enhance health education to women and their spouses on the importance of attending four or more visits and improving the quality of maternal health services to facilitate the utilization of ANC among women in the study area.
Background
The United Nations Sustainable Development Goals 3:1 aim at reducing maternal mortality to less than 70 per 100,000 live births by 2030 (Apanga & Kumbeni, 2021; UN, 2016). Globally, it has been shown that complications related to pregnancy lead to over 50% of maternal deaths each year. According to World Health Organization (WHO) report, about 90%–95% of these mortalities come from developing countries (WHO, 2005). In Tanzania, the maternal mortality ratio is about 556 maternal deaths per 100,000 live births (MoHCDGEC et al., 2016).
Antenatal care (ANC) is among the maternal and child health service intervention designed to reduce preventable maternal and childhood mortalities (WHO, 2014). Essentially, an ANC visit is a key entry point for a pregnant woman to receive numerous health services including preventive, curative, and health promotion services commonly on nutrition, HIV/AIDS, malaria, anemia, tuberculosis, and sexually transmitted infections (WHO, 2014). All of these services help a woman to improve her health and the health of her unborn baby.
Currently, WHO prenatal care guidelines recommend, pregnant women, have at least eight ANC contacts with health care providers (WHO, 2016). The new guideline reflects a change from the focused ANC (FANC) model with a minimum of four or more ANC visits to a more expanded model that accentuates many contacts and services. This model suggests the first contact occurs in the first trimester of gestation (at 12 weeks gestation), followed by two contacts in the second trimester (at 20th, and 26th weeks gestation) and five contacts in the third trimesters (30th, 34th, 36th, 38th, and 40th weeks of gestation) (WHO, 2016). When the number of contacts between a pregnant woman and a healthcare provider increases, may also increase the satisfaction of the mother with ANC services (Ekholuenetale, Benebo, et al., 2020; Ekholuenetale, Nzoputam et al., 2020). However, the proportion of pregnant women who attended the recommended eight contacts in Africa is still low. For example, the prevalence of eight or more ANC contacts in the Republic of Benin is 8.0% (Ekholuenetale, Nzoputam et al., 2020). Another study conducted in 15 countries found a pooled prevalence of 8 or more ANC contacts was just 13.0% (Ekholuenetale, 2021).
Before the introduction of the new prenatal guideline of eight ANC contact, there was another guideline of the FANC model launched by WHO in 2002 (WHO, 2002). The model package is goal-oriented with a reduced number of antenatal visits. The model recommends four visits for an uncomplicated pregnancy, where a pregnant mother should attend one visit in each of the first and second trimesters and two visits in the third trimester. The recommended services in this model include therapeutic interventions, screening, and health education. It was also suggested the availability of all services at the ANC unit, including rapid tests that are easy to perform. The integration of services in the FANC model is intended to address some of the barriers to the utilization of ANC in developing countries (WHO, 2002).
Tanzania adopted the FANC model in 2002 and the proposed timing was the first ANC visit before 16 weeks (ideally before 12 weeks but no longer than 16 weeks), second visits at 20–24 weeks, the third visit at 28–32 weeks, and the fourth visit at 36 weeks of pregnancy (Ergo et al., 2011; Magoma et al., 2013). Despite the reduced number of visits, only 51% of pregnant women make four or more visits during their entire pregnancy, and only 24% of women made their first ANC attendance before the fourth month of pregnancy. In Simiyu Region, only 39.1% of women attended four or more visits which are lower than the national average (MoHCDGEC et al., 2016).
Review of Literature
ANC is an effective healthcare strategy to improve maternal and newborn health and survival during pregnancy, delivery, and the postpartum period. Several studies have been conducted to investigate the determinants of FANC utilization. Previous studies conducted in Tanzania (Gross et al., 2012; Rwabilimbo et al., 2020), Ethiopia (Basha, 2019), and Ghana (Sakeah et al., 2017) showed that women with primary, secondary, and higher education were more likely to utilize a minimum of four ANC services compared to women with no education. Other studies indicated that women who were not involved in household decision-making were less likely to utilize FANC services as recommended (Chol et al., 2019; Rwabilimbo et al., 2020). Moreover, the literature showed different factors affecting the utilization of ANC services including maternal age, marital status, number of pregnancies, place of residence, planned pregnancy, distances to the health facilities, and cultural practices (Basha, 2019; Mgata & Maluka, 2019; Okedo-Alex et al., 2019; Simkhada et al., 2008).
However, determinants of FANC utilization are not the same across different cultures and socioeconomic statuses within a society. To improve maternal health services, it is important to assess the determinants of FANC service utilization in different settings. Therefore, this study aims to assess determinants for FANC utilization among women in the Simiyu Region Tanzania.
Methods
Design
This was a cross-sectional study that used secondary data collected in the Simiyu region by Amref health from May to June 2021. The Simiyu region is divided into five districts and is located in northwest Tanzania. In comparison to the national fertility rate (5.2 children per woman), the region has a higher fertility rate of 7.5 children per woman. Furthermore, the region has the lowest (39.1%) rate of women receiving four or more ANC visits in the country which was lower than the national average of 51% (MoHCDGEC et al., 2016).
A multi-stage cluster sampling design was used, with the first stage employing a random sampling strategy to select clusters from the 2012 Tanzania Census enumeration areas in the Simiyu region. A total of 51 clusters were selected. In the second stage, a proportionate sampling strategy was used to calculate the number of households to include in each cluster from the total number of households indicated during the enumeration's household listing. All eligible women residing in the selected household were included in the study yielding a total of 2020 women of reproductive age to be interviewed.
Research questions
Is focused antenatal care utilization related to maternal education? Is focused antenatal care utilization related to decision-making in the family? Is the level of health facility related to focused antenatal care utilization? Is planned pregnancy related to focused antenatal care utilization?
Sample, Inclusion, and Exclusion Criteria
The data set used has a total of 2020 women of reproductive age residing in the Simiyu region. The study excluded 1043 women who had not given birth within the previous 2 years and 192 women who had no information on the outcome variable (number of ANC visits). As a result, 785 women were included in this study.
Data Collection Tools and Methods
The interviewer-administered questionnaire was used for data collection. The questions were adopted from the Demographic and Health Survey and Multiple Indicators Cluster Survey. The questionnaire was translated into Swahili and installed on an android tablet using Open Data Kit. The tool was pretested in one of the villages from the Simiyu Region before the actual data collection process. A village used for pre-testing was not included in the study.
Study Variables
The dependent variable was the FANC utilization categorized into two categories “less than four visits” and “four visits or above.” The independent variables include maternal age (15–24, 25–34, 35 + ), an education level (no formal education, primary education, secondary education), employment status (employed and not employed), area of residency (rural, urban), marital status (single, married, cohabiting), husband escort to the ANC clinic, intended pregnancy, the decision of ANC utilization (personal decision, jointly with husband, relatives), and level of health facility (hospital, dispensary, health center).
Statistical Analysis
Data cleaning and analysis were done by using Stata version 15. In the descriptive analysis, continuous variables were summarised into mean and standard deviation while categorical variables were summarized into frequency and percentage. The chi-square test was used to compare the proposition of FANC uptake and the independent variables. To assess for the determinants of FANC visits, a generalized linear model, the Poisson family, with a log link was used instead of logistic regression to estimate the prevalence ratio because the prevalence of four or more ANC visits was not uncommon (thus greater than 10%). Variables with a p-value of less than or equal to .05 were considered to be statistically significant determinants of FANC visits.
Results
Sample Characteristics
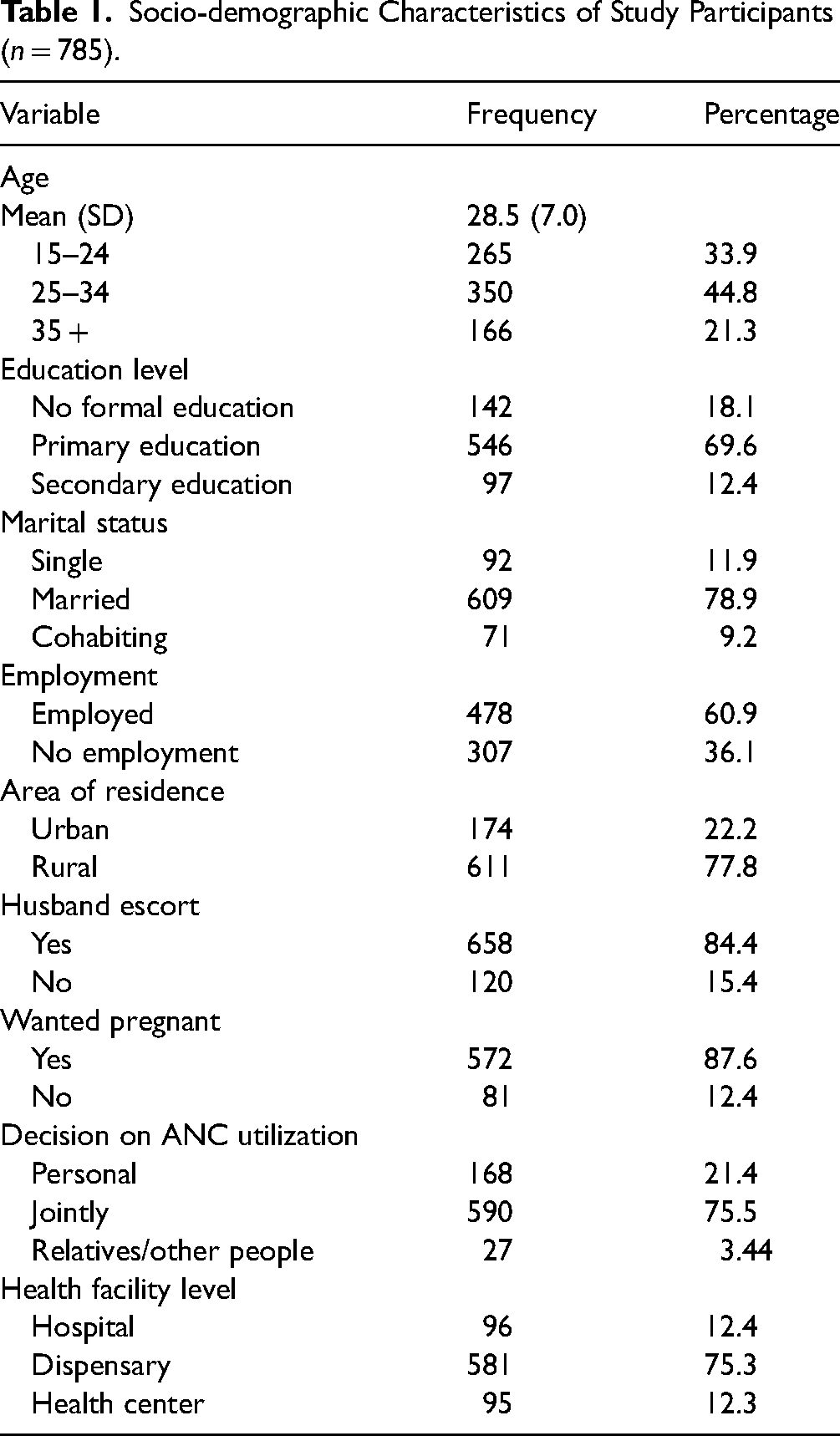
The average age of women was 28.5 ± 7 years, with 44.8% of women aged 25–34 years, 69.8% having primary education, more than half of the women (60.7%) employed, 84.4% being escorted to ANC clinics by their partner, and the majority, 75.5%, having made a joint decision with her husband on ANC utilization (Table 1).
Socio-demographic Characteristics of Study Participants (n = 785).
ANC Utilization and Components
All 785 women analyzed reported having at least one ANC visit, with 259 (34%) having four or more visits and only 40 (5.1%) having eight or more visits.
The study looked at the percentage of women who received ANC components. Among the six components evaluated, 712 (92.5%) women received malaria prophylaxis, 679 (86.8%) women received tetanus vaccination, and blood sample tests were reported among 753 (95.9%) women, 567(72.2%) women had their urine sample tested, iron supplementation was given to 576 (76.1%) women, and blood pressure was measured among 590 (75.2%) women (Table 2).
Proportion of ANC Components Among Women (n = 785).

FANC Utilization by the Characteristics of Study Participants
ANC uptake varies significantly by study participant characteristics, with 70% of women aged 25–34 years having four or more ANC visits. Among women who made a joint decision with their husbands to attend ANC, 65.4% had four or more visits, and 67.3% of women who reported having planned for the pregnancy had more than four ANC visits (Table 3).
Optimal ANC Uptake by the Characteristics of Study Participants (N = 785).

Determinants of FANC Utilization
In bivariate analysis, women aged 25–34 years had 20% less prevalence of utilizing FANC services than those aged 15–24 years (CPR = 0.80; 95%CI = 0.642–1.004). Women with secondary education had a 43% higher prevalence of utilizing FANC services than women with no formal education (CPR = 1.43; 95%CI = 0.998–2.041). Also, women who made a personal decision on ANC utilization had 26% less prevalence of utilizing FANC services than those who made a joint decision with their husbands (CPR = 0.74; 95%CI = 0.559–0.980). Furthermore, women who visited a dispensary had a 23% lower prevalence of utilizing FANC services than those who visited a health center (CPR = 0.77; 95%CI = 0.594–1.005) (Table 4).
Factors Associated With Optimal ANC Utilization.

CPR = crude prevalence ratio; APR = adjusted prevalence ratio.
In multivariable analysis, the decision on ANC utilization and the level of health facility were the factors significantly associated with FANC utilization. Women who made a self-decision had a 30% prevalence of utilizing FANC services than those who made a joint decision with their husbands (APR = 0.70; 95% CI = 0.501–0.978). In addition, women who sought services at the dispensary had 27% less prevalence to utilize FANC services than those who sought services at health centers (APR = 0.73; 95%CI = 0.540–0.982). However, education level and planned pregnancy were both marginally significantly associated with FANC uptake (Table 4).
Discussion
FANC is one of the key indicators of safe motherhood which provides an opportunity to offer a variety of services to pregnant women. The objective of this study was to assess the determinants of utilization of FANC among women in the Simiyu Region. Although the WHO guideline for FANC recommends pregnant women with no pregnancy complications to attend four or more ANC visits with skilled health care providers, only 259 (34%) of women attended four or more visits. Among those who attended four or more ANC visits only a very few 40 (5.1%) women attended eight or more contact in the study area according to new WHO guidelines which clearly shows that maternal health service during pregnancy was underutilized. A similar finding was observed in the study conducted in Ethiopia which showed that 36.2% of mothers had utilized a minimum of four and more ANC visits (Basha, 2019). A study conducted analyzing 54 priorities countries of low and middle countries found that 28.3% received 1–3 contacts and 11.3% achieved eight or more contacts during pregnancy (Jiwani et al., 2020). Again, findings from multi-country nationally representative data also showed a low prevalence of eight or more ANC contacts. For example, the prevalence of eight or more contacts in Senegal and Uganda was only 1% while in Albania and Ghana was 30.0% and 43.0%, respectively (Jiwani et al., 2020).
The observed low coverage of FANC use could be due to inadequate healthcare services in these poor-resource countries. Previous studies from low-and-middle income countries have reported the challenges of inadequate provision of maternal and child health care services due to different factors including inadequate infrastructure, lower levels of education, and poverty (Ayamolowo, 2013; Berhe et al., 2019; Workineh & Hailu 2014). Sometimes when the services are available in the facilities women may require to pay out-of-the-pocket (Kalu-Umeh et al., 2013; Meda et al., 2019) because most of them have no health insurance coverage (Ekholuenetale, Benebo et al., 2020; Nwosu & Ataguba, 2019; Tessema et al., 2022). Therefore, improved health system infrastructure, women empowerment, and universal health coverage health especially for women of reproductive age are needed to increase maternal healthcare utilization in resource-poor countries like Tanzania.
Regarding the determinants of FANC utilization, this study revealed that women who made a self-decision on ANC utilization were less likely to complete four or more ANC visits compared to those who made a joint decision with their husbands. This finding concurred with previous studies conducted in Nepal which showed that the influence of women's involvement in decision-making regarding ANC attendance or skilled delivery care, was weak, while joint discussion with spouses was linked to an increased likelihood of receiving skilled ANC attendance and delivery care (Furuta & Salway, 2006). Another study conducted in Kenya showed that utilization of maternal health services during delivery was not improved by women's overall autonomy, decision-making, or freedom of movement. Again, the decision-making of the husband only was negatively associated with ANC use and skilled delivery care compared with the joint decision-making of husband and wife (Fotso et al., 2009).
Previous studies of household decision-making accentuate that joint decision-making between husbands and wives may yield better reproductive health outcomes than women making decisions without input or agreement from their partners (Ghose et al., 2017; Hou & Ma, 2013; Mullany et al., 2005; Story & Burgard, 2012). Husbands’ involvement in decision-making is predominantly important in Africa because men dominate the culture in most household decisions including maternal healthcare utilization (Ganle et al., 2015; White et al., 2013). The observed positive associations of joint decision-making infer that couple communication and shared negotiation strategies can improve maternal health utilization. Thus, programs intended to improve women's health must consider the dynamics and ramifications of including or excluding males in their efforts. Involving husbands and encouraging couples’ joint decision-making in reproductive and family health may provide an important strategy in achieving both women's empowerment and women's health goals.
The finding from this study also showed that women who visited the dispensary had 27% less prevalence of utilizing FANC services than those who sought services at health centers. This could be due to health system-related challenges, especially in the rural setting. The underlying principle of the FANC model is the integration of care through health promotion, prevention of diseases, screening and treatment, and birth preparedness. These services are provided at the primary health facilities (dispensaries and health centers) by nurses and midwives but when pregnant women need special care are referred to higher levels (district hospital) (Chamani et al., 2021). A previous study shows that, during screening, laboratory tests missing at the dispensary are requested from a health center or hospital (Konje et al., 2018). This challenge could decrease the likelihood of women utilizing four or more ANC services at the dispensary level. Although the FANC implementation manual suggests all services are provided at the ANC unit where rapid and easy-to-perform tests should be available, it was not feasible in Tanzania especially in the rural settings due to different challenges including a shortage of drugs and supplies, skilled health workers, and long waiting times at the health facilities (Gross et al., 2011; Kanyangarara et al., 2017; Mahiti et al., 2015; Nyamtema et al., 2012). This call for the government through health facilities management committees to strengthen facilities infrastructure by arranging logistics for drug supplies and equipment, especially in a rural setting to improve ANC utilization.
Regarding education level, the likelihood of attending four or more ANC visits increased as the level of education among women increased. It was found that women with secondary education had a 43% higher prevalence of utilizing FANC services than women with no formal education. The possible explanation could be that when women are educated they become more aware of the benefit of ANC services on their health and the health of their newborn babies. Previous scholars elsewhere (Basha, 2019; Ponna et al., 2017; Tsawe et al., 2015) have documented the same finding regarding education and more appreciation of the importance of ANC among women. Also, it has been reported that education empowers women in deciding to seek health care and enables them to identify the danger signs of pregnancy (Yehualashet et al., 2022).
Moreover, a previous scholar has indicated that inadequate educational status was a major cause of health inequality in ANC coverage (Say & Raine, 2007). It has been shown that educated women were more likely to utilize four or more ANC visits and initiate ANC early within the first trimester of pregnancy compared with uneducated women (Say & Raine, 2007; Tekelab et al., 2019). This can be assumed that educated women are more employed in the formal sectors, financially independent, and better informed on the importance of ANC to the mother and baby (Gross et al., 2012; Say & Raine, 2007). Although maternal health services are provided for free in Tanzania, women still pay out of pocket for some direct medical and non-medical costs such as laboratory investigation, medication, and transport costs which may pose financial barriers to ANC services utilization among pregnant women (Gross et al., 2012).
Planned pregnancy was another factor associated with FANC utilization. Pregnant women who plan to have a pregnancy were more likely to utilize four or more ANC visits than their counterparts. It can be assumed that women with an unplanned pregnancy can give low value to the child and hence not seek reproductive health services during pregnancy. This result is in line with the finding of other studies (Basha, 2019; Sakeah et al., 2017) which showed that pregnant women who reported that the pregnancy was not planned did not utilize the FANC services. The findings from previous scholars also have shown that women whose pregnancies were planned and desired were significantly more likely to use ANC services at least once and at least four times compared with those with unplanned/undesired pregnancies (Khan et al., 2020; Tekelab et al., 2019). The finding also concurred with the results of a study conducted in Kenya revealed that women with unwanted pregnancies were less likely to attend four or more ANC visits as compared to those with wanted pregnancies (Ochako & Gichuhi, 2016). Often, most unplanned pregnancies are identified later than planned pregnancies which could result in less time to receive FANC (Gross et al., 2012; Khan et al., 2020). Again, women who have an unplanned pregnancy may have psychological problems such as depression or anxiety which could arise from less favorable behaviors either from their partners or their family members (Khan et al., 2019). Therefore, to encourage FANC utilization more effort should be done to increase the uptake of family planning resulting in securing only desired pregnancies.
Strengths and Limitations of a Study
The study presented evidence on determinants of FANC services utilization and the status of eight or more ANC utilization according to the new WHO recommendation which could be used locally and at the policy level as an input for interventions for improving reproductive health. However, the study has some limitations as well as it may be affected by recall bias since the number of ANC visits was reported by women. However, only women who give birth within 2 years before the survey were included in the study.
Implication for Practice
ANC visit is a key entry point for a pregnant woman to the health care system to receive health intervention for improving the health of a woman and that of her unborn baby. In this study, the prevalence of FANC visits among women is still low. Discussing the determinants of FANC utilization is vital to ensure improved service utilization. Therefore, healthcare providers need to enhance women's health education regarding ANC utilization and encourage couples’ joint decision-making in reproductive health as an important strategy in achieving both women's empowerment and women's health goals. It s also expected that the current findings will help the government and other health stakeholders to address the determinants of inadequate ANC utilization in the study area.
Conclusion and Recommendation
The majority of pregnant women do not adequately use four and more ANC visits. Among those who attended four visits very few of them attended eight or more ANC contacts according to a new WHO recommendation. Joint decision-making between husband and wife and the level of health facility were the determinants of FANC utilization of four or more visits. Level of education for women and planned pregnancy were also associated with FANC utilization. Therefore, it is recommended that healthcare providers enhance health education to women and their spouses on the importance of attending four or more visits and for the government to improve the quality of maternal health services, especially in the rural setting to facilitate the utilization of ANC among women in the study area. However, further study can be conducted employing a qualitative approach to explore lived experiences of women regarding determinants of FANC services in the study area.
Footnotes
Acknowledgment
We acknowledge Amref Health Africa's - Tanzania for their support and engagement in data collection to make this work possible. Sincere gratitude goes to the Regional and District Medical Officers of Simiyu Region as well as village leaders for permitting this study to be conducted in their area. We also wish to thank all research assistants, participants, and community leaders for their cooperation during data collection.
Author Contributions
AFN contributed to the study design, data collection, data analysis, and drafted the manuscript. JLS contributed to the data analysis and revised the manuscript. FNN, SM contributed to data collection, data analysis, and revised the manuscript. All authors read, commented on, and approved the final manuscript.
Availability of Data and Materials
The datasets used and/or analyzed during the current study are available from the authors upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval for this study was obtained from MUHAS RESEARCH ETHICS COMMITTEE (REC) number MUHAS-REC-09-2021-840. Permission to conduct the study was obtained from the Regional and District Medical Officers as well as village leaders. Written informed consent was obtained from each participant and was assured the right to withdraw from the study at any time whenever they felt like it. Participants were assured of confidentiality and only identification numbers (ID) were used to identify participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.