
Abstract
Background
Ethiopia has still suffered the highest burden of neonatal morbidity and mortality. The World Health Organization's practical guide for the thermal protection of newborns recommends delaying the bathing of newborns for at least 24 h following delivery, as it is crucial to prevent neonatal mortality and morbidity and to achieve 2030 sustainable development goals. However, little is known about delayed newborn bathing practices in Ethiopia. Therefore, the purpose of this study was to assess early baby bathing practices and associated factors among postpartum women.
Methods
A mixed community-based cross-sectional study was conducted among a total of 582 postnatal mothers. A multistage sampling technique was used to select study participants. A pre-tested and structured questionnaire was used to collect data. The data was entered into Epi-Data version 4.2.0 and exported into SPSS version 23 for analysis. Three focus group discussions with postnatal mothers were used for qualitative data. A purposive sampling method was used. Thematic analysis was used for qualitative data. Bivariate and multivariate logistic regression analyses were used in the analysis. To declare statistically significant, p-values of .05 were used.
Result
This study revealed that 250 (43%) mothers were practicing early newborn bathing. Early baby bathing was associated with antenatal care (ANC) follow-up (AOR = 5.1 = .95% CI = (2.6–9.9)), having no recent complications during birth (AOR = 1.9 = 95% CI = (1.02–3.6), having information about the time of baby bathing (AOR = 6.02, 95% CI = (3.9, 9.3)), knowledge of hypothermia (AOR = 3.3 = 95.6% CI (1.9–5.8), and poor knowledge about neonatal danger signs.
Conclusion and Recommendation
ANC follow-up, recent complications during birth, having information, knowledge about hypothermia, and neonatal danger signs were significantly associated with early baby bathing. Continuous health education on the appropriate time of baby bathing and neonatal danger signs and enhanced ANC service utilization are recommended.
Keywords
Introduction
The World Health Organization (WHO) practical guide for the thermal protection of newborns recommends delaying the bathing of newborns for at least 24 h following delivery (Lunze & Hamer, 2012). Delaying bathing immediately after birth to prevent neonatal hypothermia, contributes to neonatal morbidity and mortality (Dickson et al., 2014; Partnership for Maternal & Health, 2011; Victor et al., 2013). The first bath aims to remove residues of the skin as blood and meconium on the newborn's body and to provide hydration to the stratum cornea of the newborn's skin to maintain skin integrity, body temperature, and barrier function property (Kuller, 2014). The first bath should be delayed until the newborn is thermally stable because bathing is related to a significant loss of heat (Ruschel et al., 2018). Newborns are unable to maintain their body temperature without thermal protection, particularly preterm and low birth weight babies at risk (Ringer, 2013). Hypothermia due to early bathing contributes to global neonatal mortality either directly or indirectly and major causes of death if concurrently occurred with, such low blood sugar levels, respiratory distress, abnormal clotting, jaundice, pulmonary hemorrhage, and increased risk of developing infections (Children, 2004). A newborn's first bath removes vernix and maternal bacteria, interrupts skin-to-skin contact which causes, hypothermia, and hypoglycemia, and may inhibit the crawling reflex which causes potentially reducing the time to effective breastfeeding (Bergström et al., 2005; Kuller, 2014). Globally case fatality rate of neonatal hypothermia at hospitals and at home range from 32% to 85% and 11% to 92%, respectively (Lunze et al., 2013). In Africa, the prevalence of neonatal hypothermia is high, ranging from 44% to 85% (Kambarami & Chidede, 2003; Lunze et al., 2013). To protect a newborn from such consequences of hypothermia, delaying baby baths is essential. Qualitative studies have also shown that newborn bathing practices varied across studies, but cultural and traditional beliefs are still contributing to the practice of early newborn bathing (Adejuyigbe et al., 2015; Waiswa et al., 2008). Uneducated, no knowledge of hypothermia, being Primi para, have no antenatal care (ANC), poor knowledge about newborn danger signs, living in areas, vaginal mode of delivery, and whose birth were not attended by skilled birth attendants (SBAs) were found to have a positive influence on the practice of early baby bathing practice (Abebe et al., 2021; Alem et al., 2020; Brhane et al., 2017; Welay et al., 2020). Conversely, an earlier study in India found that ANC visits and birth that were not attended by SBA were not significantly associated with the baby bathing practice. Even though there is enough evidence to support the benefits of delayed newborn bathing, it is the most poorly practiced component of the essential newborn care package, especially in sub-Saharan Africa like Ethiopia. Therefore, this study aimed to assess early baby bathing practices and their associated factors among postpartum mothers.
Literature Review
Proportion of Baby Bathing Practice
Bathing time for newborns, education on newborn care, and neonatal danger signs are parts of routine education of the every mother after delivery in Ethiopia. Delaying baby bathing is a vital intervention to be maintained immediately after birth to prevent hypothermia, which contributes to neonatal morbidity and mortality (World Health Organization & Newborn Health/Safe, 1997). The consequences of early bathing are not limited to hypothermia. It is also associated with low blood sugar levels, respiratory distress, abnormal clotting, jaundice, pulmonary hemorrhage, and an increased risk of developing infections (Kambarami & Chidede, 2003). WHO recommends that the first bath be given only once the infant has achieved vital signs/cardiorespiratory, and thermal stability (WHO, 2013).
A study conducted in India shows that 82.6% of women gave baths to babies immediately after delivery (Rahi et al., 2006). A study conducted in Nepal showed that 75.5% of newborns had bathing during the first 24 h(Khanal et al., 2014). In Pakistan, 86% of respondents reported that the first bath of their newborns was within 24 h of delivery (Gul et al., 2014). Another study was done in Pakistan; 37.2% of women gave baths to the baby immediately, 77.8% within 6 h, and 18.3% within 7–24 h.
A study in Sub-Saharan Africa found that over 50% of newborns were bathed within 6 h of delivery (Bee et al., 2018). Studies in Malawi and Bangladesh showed that bathing practices varied in the two settings; in Malawi, only 26% were bathed after 24 h, but 87% were cleaned after the same period (Khan et al., 2018).
A study conducted in Ghana showed that 93% of mothers bathed their newborns before 24 h (Hill et al., 2010). In another study conducted in Ghana, only 22.6% of mothers bathed their newborn babies after 24 h of delivery, whereas 74.4% bathed their newborn babies before 24 h of delivery (Alem et al., 2020).
In a study conducted in Tanzania, 45% of babies born at a health facility and 19% born at home were bathed six or more hours after birth (Shamba et al., 2014). A study conducted in four regions of Ethiopia showed that 74.7% of mothers bathe newborns during the first 24 h of life (Callaghan-Koru et al., 2013).
The study was done in west Guje, SNNP. About 84% of women bathed their newborns within less than 6 h of delivery (Wako & Beyene, 2020). A survey in Harar showed that 35.4% of mothers bathed their newborn before 24 h of delivery (Welay et al., 2020). A study conducted in Jimma showed that 32.5% of mothers bathed their newborn within the first 24 h of delivery (Kebede et al., 2022).
Factors Associated With Early Neonatal Bathing
A study done in Nepal shows that less educated mothers, mothers who did not attend ANC visits, and whose births were not accompanied by skilled workers were significant factors in early baby bathing (Khanal et al., 2014). A study conducted in Bangladesh shows that low parental education, low utilization of ANC services, the absence of SBAs, higher birth order, and the mother's age at birth were significant factors affecting early baby bathing (Khan et al., 2018).
A study conducted in Sub-Saharan Africa found that unemployed mothers who had home delivery and made their first antenatal visit in the third trimester were significant factors in early baby bathing (Ayete-Nyampong & Udofia, 2020). A study conducted in a rural community in Ghana showed that the level of education, place of delivery, ethnicity, and socioeconomic class were significant factors affecting baby bathing (Alem et al., 2020).
A study conducted in South West Ethiopia showed that being an urban resident, attending ANC visits, and having immediate postnatal care (PNC), were significantly associated with neonatal bathing (Abebe et al., 2021). A study conducted in Mekele showed that the gestational age of the newborn and the status of health providers who attended the delivery were statistically significant with baby bathing (Brhane et al., 2017).
A study conducted in East Gojjam showed those women who have primary and above educational status, quick PNC visits, advice about birth preparedness during ANC visits, and information about baby bathing had statistically significant associations with baby bathing practice. A study done in Harar shows that being uneducated, having no knowledge of hypothermia, being Primi, and not utilizing a newborn bed net were statistically significant factors of the early neonatal bath. A study done in Jimma showed that mode of delivery, lower educational status, poor knowledge about danger signs, and mothers not knowing about hypothermia were significantly associated with early neonatal bathing practice (Kebede et al., 2022).
Methods
Study Area and Period
This community-based mixed study was conducted in Gurage Zone from April 1, 2022 to June 1, 2022. The Gurage zone is one of the administrative zones in South Ethiopia. It has 16 districts and five town administrations. Wolkite town is the capital of the Gurage zone area. It is 153 km southwest of Addis Ababa, the capital of Ethiopia. According to the 2007 national household census, the Gurage zone has a population of 1,279,646, of which 657,568 are women and, 622078 are men (“CSA of Ethiopia. Statistical Reports of the Census for Southern Nations, Nationalities and Peoples Region”, 2007).
Study Design and Population
A community-based mixed cross-sectional study design was conducted from April 1, 2022 to June 1, 2022. The source population was all mothers who gave birth in the last month before the study period in Gurage Zone. All women who gave live birth within the first months of postpartum during the data collection period were included in the study. Postnatal mothers who were unconscious, or seriously ill, newborns with abdominal defects, newborns who delivered on transportation and contaminated, and mothers who delivered a dead baby and had known mental illness were excluded.
Sample Size Determination
The sample size was determined by using the single population proportion formula, with the following assumptions: proportion (p) of a population early baby bathing practice to be 35.4% as estimated from the study conducted in Harar, confidence interval (CI) of 95%, and 5% of marginal error (d), making non-response rate 10%, % to the larger sample size which was 388. Then, consider the 1.5 design effect. The final sample size was
Sampling Techniques and Procedures
For quantitative data, a multi-stage sampling method was used to draw the final sample size. Purposive sampling was used for the qualitative data. The Gurage zone has 16 districts and five town administrations. First, from those districts and town administrations, the researchers selected six districts and two town administrations by simple random sampling technique. Postnatal mothers in each District are 338 in Cheha, 158 Abashge, 260 in Gumer, 314 in Azha, 181 in Meskan, and 125 in Enor Ener, and also in each town 29 in Emdebir and 156 in Wolkite. Second, 40 Kebeles were selected out of 114 Kebeles of the District and four kebele were selected out of seven kebele of town administration by simple random sampling. Total of 1376 postnatal mothers were living in 40 selected districts Kebeles and 185 postnatal mothers living in four selected towns of Kebeles. Then, the possible number of respondents in each of the kebele was allocated proportionally based on one monthly report of postnatal mothers. Finally, systematic random sampling was used to select the study participants in each kebele as K = N/n = 1561/582 where K is the skipping interval which is three from the sampling frame found from records of health extension workers (HEWs) of the kebele (Figure 1).
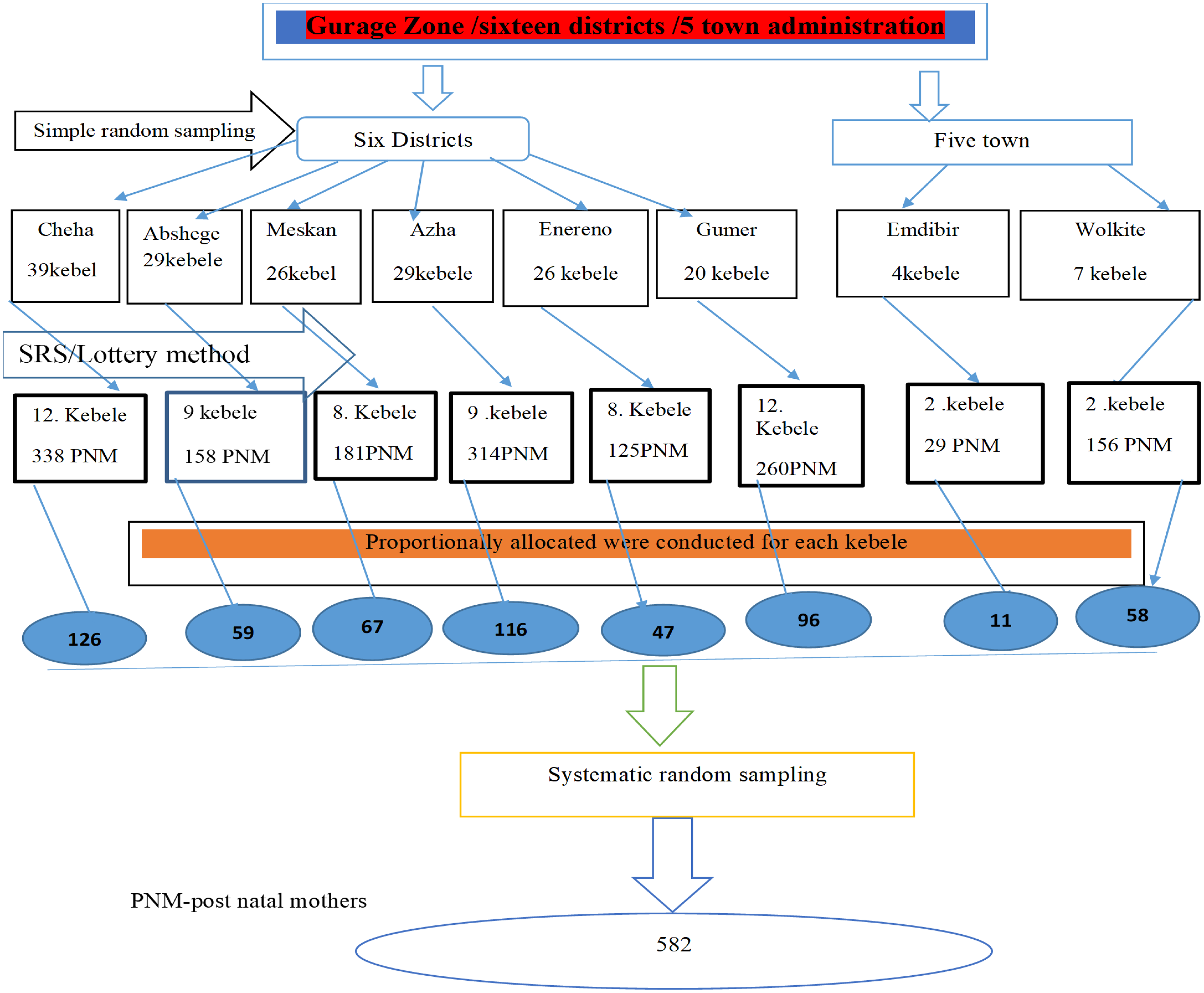
Schematic representation of sampling procedure for early baby bathing practice and associated factors among mothers who give birth within the past one month at Gurage Zone, SNNPR, Ethiopia, 2021/2022.
Study Variables
Operational Definitions
Data Quality Management
To ensure quality, experts translated the questionnaire into the local language (Amharic). Finally, before data collection, it was re-translated back to the English language to verify consistency. Before starting the actual data collection, three days of extensive training were given to the data collectors and supervisors. A pre-test for the appropriateness and feasibility of the tool was conducted and all necessary modifications and amendments were done accordingly. The data collection team communicated and discussed with principal investigators if they faced any challenges during the data collection period. After data collection before analysis, all collected data were checked for completeness.
Statistical Analysis
After ensuring the completeness of the questionnaire, the data were checked, cleaned, coded, and entered into EPI data 4.2 statistical packages and analyzed using SPSS version 23 software. The audio-taped qualitative data were transcribed into the English language. Then, codes or terms were identified and tallied to come up with some categories, which were later used to establish themes based on the objective of the study. Finally, a thematic analysis was done, and the findings were triangulated with the quantitative one. Binary logistic regressions were employed to identify the relationships between the predictors and the outcome variable and select variables with a p-value less than 0.2 at a 95% confidence interval as a candidate for multivariable logistic regression analysis. The goodness-of-model fitness was checked by Hosmer-Lemeshow and its value was above 0.05.
In multivariable analysis, a multivariable logistic regression model was done to control the confounders. Multicollinearity was checked to see the linear correlation among the associated independent variables by using the variance inflation factor (VIF). The VIF of the data was <10 and no sign of multicollinearity is detected. The direction and strength of statistical association were measured by an odds ratio with 95% CI. Adjusted odds ratio along with 95% CI was estimated to identify predictors for early baby bathing practice. In this study, p-value < .05 was considered to declare a result as a statistically significant association. Proper coding and categorization of data were maintained for the quality of the data to be analyzed.
Ethical Considerations
Ethical clearance will be obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Wolkite University College of Health and Medical. Participants will be informed clearly about the purpose and benefits of the study and written informed consent were obtained from the participants. Those who are signed written consent only participate in the study and the confidentiality of respondents was maintained throughout the research process by giving codes to participants. Personal privacy was respected. The respondents had the right not to participate in the study or withdraw from the study at any time or stage of the interview.
Results
Socio-Demographic Characteristics
In this study, 582 participants responded to the questionnaire, with a total response rate of 100%. The majority of the respondents were in the age group 20–34 and the mean age of study participants was 28.37 (±5.28 SD). Of the respondents, the majority were married 556 (95.5%), and lived in rural locations constitutes 361 (62%). Orthodox Christianity was the dominant religion 343 (58.9%) among study participants (Table 1).
Socio-Demographic Characteristics of Study Participants in Gurage Zone, Southern Ethiopia, 2022 (n = 582).

Maternal and Child Health Service
This study showed that half of the mothers, 311 (53.4%) had a parity of two to four. Of the respondents, 494 (84.9%) had ANC follow-up, out of them two-hundred and ninety-nine (58.9%) had four and more visits. During ANC follow-up two-third of the respondent 328 (65.5%) were getting counseling about birth preparedness and complication redness. The majority 564 (96.9%) of the mothers gave birth at a health facility. Five-hundred sixty-three (95.7%) study participants gave birth through vaginal delivery. Of the respondents, 558 (95.9%) were assisted by health-SBAs. The remaining women 9 (1.5%), 3 (0.5%), 9 (1.5%), and 3 (0.5) were assisted by traditional birth attendants (TBAs), HEW, family/relative, and without any assistance respectively 153 (26.3%) of mothers had PNC in recent baby births. Only 97 (16.7%) mothers had faced complications recently (Table 2).
Maternal and Child Health Service of Study Participants in Gurage Zone, Southern Ethiopia, 2022 (n = 582).

Health Facility-Related Characteristics
Out of the respondents, 85 (14.6%) stated that hospitals were available nearby, 243 (41.8%) had access to health canter, and 254 (43.6%) had access to health posts. Five-hundred sixty-nine (97.8%) stated that these health care institutions create awareness about essential newborn care. Several healthcare providers were involved in creating awareness including 388 (66.7%) HEWs and health 156(26.8) nurses/midwives, and 25 (4.3) public health officers. Out of the study participants, 406 (69.8%) stated that the distance to healthcare institutions was less than 5 km. The majority of the FGD discussants stated that HEWs in home-based sessions create awareness about when to bath the newborn, when to initiate breastfeeding, cord care after delivery, and about immunization. Before the prevalence of HEWs, the majority of mothers partook in traditional practices which can predispose the newborn to complications.
Maternal Knowledge About Neonatal Danger Sign
Knowledge of newborn danger signs was low as only 208 (35.7%) of respondents were knowledgeable (who are mentioned greater than or equal to the mean value). Furthermore, 459(78.9%) mentioned fever and 455 (79.9%) mentioned diarrhea, and 337 (57.9%) mentioned vomiting (Figure 2).

Maternal knowledge of neonatal danger sign in Gurage Zone, Sothern Ethiopia (n = 582).
Timing of Newborn Bath
Regarding the time of bathing of newborn, of the respondents, 250 (43%) with 95% CI (39%, 46%) of respondents bathed their newborn within the first 24 h of birth (Figure 3).

Time of bathing among mothers in Gurage Zone, Southern Ethiopia, 2022 (n = 582).
The majority of 471 respondents (80.9) washed the child with hot water for the first time after birth, whereas 111 respondents (19.1%) bathed the newborn for the first time with cold water. Additionally, only one-hundred fifty-five (26.6%) of women knew about hypothermia.
The qualitative finding also supported the quantitative one in that there are still problems with the baby bathing practice.
The majority of the discussants reported that either the TBA or families who attended the birth bathed the baby immediately with warm water after birth. This shows a lack of understanding of the value of delaying bathing.
A 26-year-old FGD participant said, “I gave birth to my child two weeks ago with the assistance of a traditional birth attendant. She washed my infant and me with hot water as soon as the placenta was removed and live me in a very hot house, heated by firewood. The other important thing is to keep the newborn from cold fresh butter was put on the head and covered by plant leaf, then a small cloth was wrapped around the head. To me, this is what women do in our society….”
On my way to the hospital, I gave birth in the street. When we got home, my family bathed the infant while I awaited the delivery of the placenta.
However, some moms claimed that community HEWs and medical professionals had given them health education or understanding about the value of postponing baths. As a result, they no longer bathe newborns immediately after birth.
In the FGD, every mother concurred that immediate bathing of newborn babies was the norm when a mother gives birth at home. A few mothers who argued for changing this practice cited information they learned from community HEWs or recent health education workshops they attended about delaying bathing. However, there were differences in the mothers’ opinions regarding how long bathing should be postponed, with replies ranging from 2 to 24 h following birth. As a result, although aware of the delay in bathing, moms were unsure about how long the delay should be.
The reason why we bathe the newborn is to prevent the child from smelling bad, so that when visitors come they will be very eager to pick up the baby, and also to prevent the baby from body odor.
The reason why I normally bathe the baby is to ensure its comfort as well as its health and well-being. As I bath the baby very well, she's going to feel rested and can sleep o.k. she will feel refreshed and will sleep very well. The baby will also appear neat and clean. In all sites, there was a desire for the baby to be clean, neat, comfortable, and presentable to visitors and this was a key factor in early bathing when it did happen.
Health workers’ actions or recommendations, a fear of the cold, particularly if the baby was delivered at night, and the absence of an evident vernix were all reasons for delaying bathing: “He can get cold, so he is right away wrapped in cloth with stuff he was delivered with still on him, He will get cold, therefore he will be immediately wrapped in cloth with the stuff he was delivered with still on him, however, if the baby is delivered at day time, he is bathed with lukewarm water right away” (29-year-old mother).
Factors Associated With Early Newborn Bath
In the bivariable logistic regression, educational level, complications during recent birth, ANC follow-up, PNC follows up, distance from the health facility, knowledge of hypothermia, knowledge of danger signs, and previous information about the time of baby bathing were candidate variables. Also, the multivariate analysis revealed that no complications during recent birth, no knowledge about hypothermia, poor knowledge about neonatal danger signs, no ANC, and no information about the time of baby bathing were the most statistically significant factors that determined early newborn bathing.
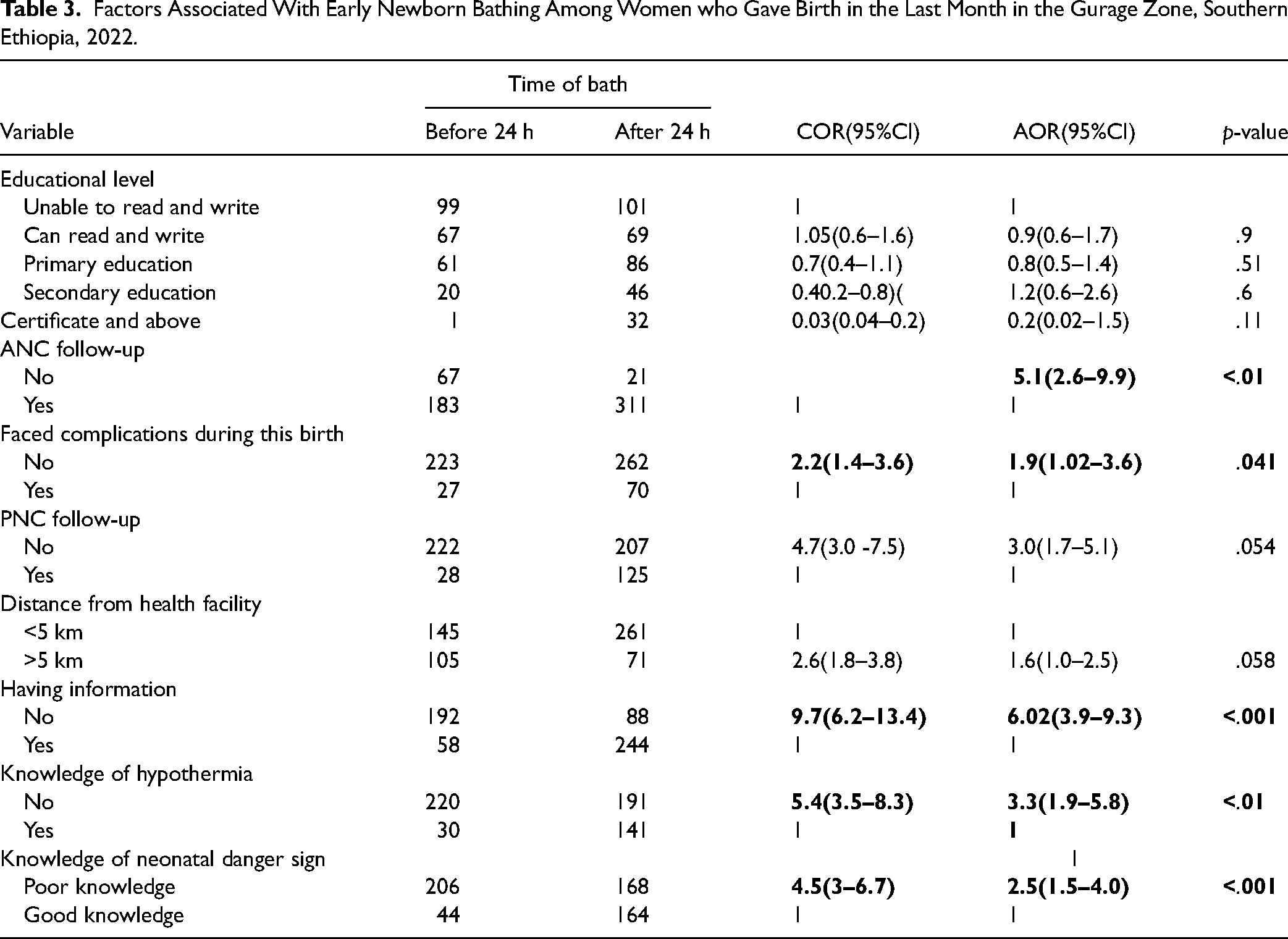
Mothers who attended ANC services were found to have a statistically significant association with the baby bathing practice. Those who didn’t attend ANC visits at all were 5.1 times more likely to practice early baby bathing as compared with those women who visit ANC at least once for the current delivery (AOR 5.1 = .95% = (2.6–9.9). Mothers who have no complication with recent birth were 1.9 times more likely to practice early baby bathing when compared to counterparts (AOR = 1.9 = 95%-(1.02–3.6). Mothers who have no information about the time of baby bathing were 6 times more likely early baby baths when compared to those who had information about baby bathing time (AOR = 6.02, 95% CI = (3.9, 9.3)). Mothers who had no knowledge of hypothermia were 3.3 times more likely to early bath their newborn when compared to those who had knowledge about hypothermia (AOR = 3.3 = 95% = (1.9–5.8)). In addition, knowledge of mothers about neonatal danger signs was also another factor that had a positive association with baby bathing practices. Those who had poor knowledge were 2.5 times more likely to practice early baby bathing compared to those who had good knowledge of neonatal danger signs (AOR = 2.5, 95% CI = (1.5, 4.0)) (Table 3).
Factors Associated With Early Newborn Bathing Among Women who Gave Birth in the Last Month in the Gurage Zone, Southern Ethiopia, 2022.
Discussion
Delaying baby bathing is an essential component of thermal care to be maintained immediately after birth that has a crucial role in reducing neonatal hypothermia, which contributes to neonatal morbidity and mortality. Hence, the WHO recommended that new-born baby is not supposed to be bathed until after 24 h of delivery.(WHO, 2013). In this study, overall early baby bathing practices was 43% with 95% CI = (39%–46%).
This result is higher than study conducted in Bangladesh (13%) (Khan et al., 2018), Harar, region Eastern Ethiopia (35.4%) (Welay et al., 2020), and Jimma (Kebede et al., 2022), which was 32.5%. This discrepancy may be due to inadequate prenatal, perinatal, and postpartum counseling, insufficient understanding of the value of delayed bathing, or both; low awareness about the importance of delayed bathing and maybe a lack of proper advice before, during, and after birth. Additionally, this may be attributed to the level of community acceptance of the health extension program as well as the specific professional competencies of those working in both settings. Poor PNC, counseling, and insufficient home visits may be a part of the current issue. Poorly informed mothers are more likely to engage in harmful customs that could harm the health and growth of their unborn children. The present national and international aim is to reduce newborn mortality by 2030 (Nations, 2016).
However, this study's finding is lower than studies conducted in Nepal (75.5%) (Khanal et al., 2014), Malawi (74%) (Khan et al., 2018), Ghana (74.4%) (Alem et al., 2020), four regions of Ethiopia (74.7%) (Callaghan-Koru et al., 2013), and Guji (84%) (Wako & Beyene, 2020). This finding discrepancy might be due to the differences in sociodemographic characteristics of mothers, and the difference in time and also might be due to Ethiopia's health extension program, which has increased women's access to prenatal care and PNC in the research area.
In this study, mothers who didn’t attend ANC visits at all were 5.1 times more likely to practice early baby bathing as compared with those women who visit ANC at least once for the current delivery. This is in line with a study conducted in Nepal (Khanal et al., 2014) and Bangladesh (Khan et al., 2018). This may be due to the possibility of getting information about hypothermia and the importance of delaying baby bathing from healthcare providers during ANC.
Mothers who have no complications with recent birth were 1.9 times more likely to practice early baby bathing when compared to their counterparts. This may be because women who have just given birth without complications may have left the hospital earlier and may engage in early bathing than mothers who have faced complications and stay longer in the hospital since health professionals can educate and follow early baths in the hospital.
Mothers who have no information about the time of baby bathing were 6 times more likely early baby baths when compared to those who had information about baby bathing. The other reason might be women had got information about baby bathing, improving knowledge along with increasing self-efficacy or empowerment in making better decisions regarding delayed baby bathing practice. In addition, those who had information may change their belief, perception, miss rumor, and practice of individuals.
Mothers who had no knowledge of hypothermia were 3.3 times more likely to early bath their newborn when compared to those who had knowledge about hypothermia. This study was consistent with studies done by Harar (Welay et al., 2020) and Jimma (Kebede et al., 2022).
In this study, mothers who had poor knowledge about neonatal danger signs were 2.5 times more likely to practice early baby bathing compared to those who had good knowledge about neonatal danger signs. This finding was in line with study done in Jimma (Kebede et al., 2022). This result might be explained by the fact that women who had a positive awareness of neonatal danger signs experienced how to practice thermal care. Many developing nations, like Ethiopia, now face a serious problem related to neonatal risk. In this regard, the health-seeking behavior of mothers for neonatal care highly relies on their knowledge of neonatal danger signs, and it has been hardly investigated.
This study may have its limitations. The quantitative findings relating to baby bathing practice were based on reports by mothers that might have introduced some biases and could have been under- or over-reporting. Therefore, this limitation must be considered in interpreting the findings of this study.
Strengths and Limitations of the Study
The researchers used a mixed-method study design.
For generalizability, a representative sample of recently delivered women is selected using a multistage, random sampling strategy for both the quantitative household surveys and the qualitative in-Focus group discussion.
Quantitative findings relating to baby bathing practice were based on reports by mothers that might have introduced some biases and could have been under- or over-reporting.
Social desirability bias.
Implication for Practice
The findings from this study have several implications for improving early baby bathing. This study revealed that factors that have a significant association with the early baby bathing practice and, it provides important information for Zonal health offices and their respective districts to improve baby bathing practice should promote strong community-based behavior change communication on the importance of delaying baby bathing practices to change the early baby bathing practice in the study area. Health facilities should enhance linkage with health posts to increase ANC and PNC service utilization and HEWs should promote and give health education about early bathing and their complication and newborn danger.
Conclusion and Recommendations
The overall early baby bathing practice in this study was 43%. This implies that many mothers continue to practice in contravention of WHO guidelines, and more work is needed to promote late newborn bathing both in healthcare institutions and at home. ANC follow-up, having no information /awareness about the time of baby bath, no faced complications during recent birth, knowledge about hypothermia, and having poor knowledge about neonatal danger were significantly associated with the early baby bathing practice. Continuous health education on the appropriate time of baby bathing and neonatal danger signs and enhanced ANC service utilization are recommended.
Footnotes
Abbreviations
Acknowledgment
We would like to thank Wolkite University, for giving us the chance to conduct this research. We also want to thank the study participants, data collectors, supervisors, health institutions administrate, data clerks, and others who directly or indirectly contributed to this work for their kind cooperation.
Author Contributions
ABD MOG, MDS, and SAS conceived the study and wrote the original draft of the manuscript. Analysis and interpretation of data were made by ABD, HAW, FE, BT, and SAS; they supervised the proposal development, data collection, analysis, and interpretation of data. FE, MOD, ABD, YY, SAS, and MDS reviewed the draft manuscript for intellectual content and participated in the revision. All authors have read and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval for this study was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of Wolkite University, College of Medicine and Health Sciences (Ref. No. : IBRERC/07/2022). Participants in the study were briefed about the objectives and aims of the study in detail. Participants were informed that their participation was purely voluntary and was assured of the confidentiality of all information. After all, informed, voluntary, written, and signed informed consent was obtained from study participants before the study. Confidentiality of the data was assured throughout the study.
Data Availability
Data that support the findings are available from the corresponding author on a reasonable request.
Informed Consent
Written and verbal consent was obtained from all subjects.