
Abstract
Introduction
Emotional stress and anxiety during COVID-19 pandemic has gained a lot of attention. The capacity to withstand from the manipulated thinking and COVID-19 related stress and anxiety depends on the resilience level of an individual. Cognitive behavioral therapy (CBT) has patronizing benefits for people affected with altered mental health. Relieving COVID-19 related anxiety using CBT has beneficial impact on health and improves quality of life of people.
Objective
Aimed to relieve the anxiety of Omani population during COVID-19 pandemic using CBT.
Methods
This research utilized a pre-experimental one group pre-test post-test design. A non-probability convenient sampling technique was used to select 96 Omani people who fulfilled the inclusion criteria. The pre-anxiety level was assessed using CAS (Corona virus Anxiety Scale). The participants who scored above nine in the scale were given three sessions of CBT. Post-anxiety level was assessed using CAS after three CBT sessions.
Results
The study revealed that the level of anxiety reduced during post-test (6.35) after intervention when compared to pre-test (13.22). The CBT intervention was effective in reducing the anxiety in the post-test at p ≤ .000.
Conclusion
CBT is effective in reducing COVID-19 related anxiety among the Omani population. Therefore, this strategy is highly recommended in people having mental health issues.
Introduction/Background
The world is facing unprecedented times due to COVID-19 pandemic and struggling to recover from the impact of this deadly infectious condition as new variants keep emerging (Tabish, 2020). In the month of March 2020, the World Health Organization (WHO, 2020) declared COVID-19 to be a pandemic as greater number of cases with significant mortality rates were recorded worldwide (Cucinotta & Vanelli, 2020). Even though COVID-19 vaccine from different companies is on the go, still new cases are being confirmed daily across different countries (Organisation for Economic Co-operation and Development, 2021). As we are in the midst of the pandemic, most people are concerned, worried, and feel anxious about the uncertainty around us. There has been loss of lives, impaired health and wellbeing, loss of business and finance, loss of jobs, restrictions to travel and social gatherings and on the whole loss of freedom to live to some extent. People around the world have trouble to adjust and react to these sudden changes (Pietrabissa & Simpson, 2020).
COVID-19 outbreak documented stressors including boredom, fear, and frustration, lack of information, inadequate supplies, stigma, and financial loss (Brooks et al., 2020). Sheltering people in isolation resulted in mental health issues secondary to stress and anxiety related to COVID-19 (Son et al., 2020). Higher levels of anxiety and depressive symptoms are reported among general population during this pandemic (Nelson et al., 2020). Additionally, psychological and mental health effects were notably seen in college students in China. There has been a global prevalence of anxiety and depression in 25% of public (WHO, 2022). Population based studies from India, Italy, Japan, China, America, Turkey, Spain, Greek, and Singapore demonstrated a total prevalence of anxiety symptoms as 32.60%. Furthermore, the prevalence of anxiety (63.90%) and depression (55.40%) was higher in suspected and confirmed patients with COVID-19 (Liu et al., 2021).
Review of Literature
COVID-19 threatens the physical health of people to a greater extent. In the same way, it has led to mental health impact (Berg-Weger & Morley, 2020; Dubey et al., 2020; Usher et al., 2020). Mental health problems increased due to COVID-19 pandemic secondary to financial instability, social isolation, inability to meet basic needs, and fear of the disease. More and more cases of depression and anxiety are on the rise and the pre-existing mental illness has been aggravated (Surmai & Duff, 2022).
The major negative mental health issues reported during COVID-19 pandemic were anxiety and depression (Chen et al., 2020; Choi et al., 2020; Wang et al., 2020). The prevalence of anxiety in health workers accounted for 32.7%; whereas the prevalence of anxiety in the public accounted for 29.5% (Liu et al., 2021). In Oman, 27.9% of the healthcare workers experienced moderate to severe anxiety. Moreover, the higher proportion affected (32.0%) were Omanis compared to 22.2% non-Omanis (Khamis et al., 2020). In Oman, 38.1% of physicians and 61.9% of nurses were affected with moderate to severe COVID-19 anxiety (Badahdah et al., 2021). Moreover, higher levels of anxiety have been reported by the public in Oman (Alaloul et al., 2021).
In addition, many studies have documented lifestyle disruptions including lack of sleep, exercise, impaired social distancing, and disrupted mental health (Adams-Prassl et al., 2020; Allcott et al., 2020; Banks & Xu, 2020; Beland et al., 2020; Brodeur et al., 2021; Brooks et al., 2020; Ong et al., 2021; Proto & Quintana-Domeque, 2020). Moreover, decline in physical activity was associated with higher rates of depression during the pandemic (Giuntella et al., 2021). Considering the major mental health impact of the pandemic, the WHO in collaboration with International non-governmental organizations, United Nations agencies, Red Cross and Red Crescent Societies worked to promote integration of psychosocial support to people across the world (WHO, 2022).
Several psychological intervention programs have been developed to reduce the mental health problems in people with COVID-19. Online and telephone psychological interventions were carried out in earlier research (Liu et al., 2020; Zhang et al., 2020). In addition to online and telephonic interventions, in-person psychological individual and group interventions were provided (Shechter et al., 2020; Muller et al., 2020; Rodriguez-Menéndez et al., 2021). Comparing to online psychological interventions, in-person interventions have been generally accepted by the people (Cuijpers et al., 2019; Shechter et al., 2020). However, either in-person or online, these interventions enhance the emotion regulation skills and prevent the incidence of mental disorders. Moreover, mental health interventions shall be developed in collaboration with national and international agencies (Priede et al., 2021).
Although various psychological interventions have been tried to relieve anxiety, cognitive behavioral therapy (CBT), which is an evidence-based psychotherapy, has been used across the world to prevent and treat physical and psychological issues (Chan et al., 2018; Schure et al., 2019). CBT aims to help the person to identify his/her level of stress and anxiety and modify his/her beliefs and behavior through behavioral changes, social support, and cognitive restructuring (Beck, 1979). CBT helps in reducing or eliminating symptoms of psychological distress and assist the individual to return to normal day-to-day life. The people received CBT had shown significant reduction in anxiety levels, enhancement of quality of life, and improvement in psychological status and somatic symptoms (Hartley et al., 2016; Tang & Kreindler, 2017; Yang et al., 2014).
Purpose
Considering the benefits of CBT and higher prevalence of COVID-19 related anxiety among the public, the investigators proposed to determine the efficacy of virtual CBT on the COVID-19 pandemic related anxiety among Omani population. The investigators believe that CBT as an evidence-based intervention would be effective and efficacious in the management of COVID-19 related anxiety and would bring beneficial patient reported outcomes. The study hypothesized that there is no significant difference between the pre- and post-interventional level of COVID-19 related anxiety among the Omani people.
Theoretical Framework
The investigators adopted Pender's health promotion model (1996) (Alligood, 2017) as a theoretical framework to guide us in the study. The investigators utilized this model as it assisted in understanding the major determinants of COVID-19 related anxiety among Omani people. In addition, it acted as a basis for designing CBT for the Omani people affected with COVID-19 related anxiety.
Methods
Research Design
A one group pre-test post-test pre-experimental design was adopted in this study.
Research Questions
Is virtual CBT effective on the COVID-19 pandemic related anxiety among Omani population?
Setting
The study was conducted in North Batina, South Batina, Sharqiya, and Muscat Governorates in Oman. As it is a national study, and to have representative samples in Oman, these four governorates were randomly selected. The study was conducted through virtual mode.
Sample
To calculate sample size, the researchers considered the sample selection criteria. The researchers selected adults aged 18–60 years who are willing to undergo CBT. Hence, the accessible population was selected with a confidence level of 95% and confidence interval of 10. The calculated sample size is 95.
Sampling Strategy
Convenient sampling technique was used in selecting the participants of the study.
Inclusion and Exclusion Criteria
Omani population from Northa Batina, South Batina, Sharqiya, and Muscat Governorates in the age group of 18–60 years, who can read and write English or Arabic and who were suffering from anxiety due to COVID-19 (based on CAS [Corona virus Anxiety Scale] scores) were included in the study. The score above 9 in total or high in one individual item is considered as anxiety. The researchers considered this age group as they were considered as adults who can follow the steps of CBT. Adult men and women in the medical field were excluded from the study.
Ethical Considerations
The informed consent was obtained (Implied consent) when the participants responded to the demographic data and CAS tool. The study purpose was explained to the participants of the study. None of the participants were forced to participate in the study. None of their identifying information was collected. They were given the freedom to withdraw their participation from the study at any point of time during the course of the study. The collected data was stored in a password protected file. Only the investigators had access to the collected data.
Description and Interpretation of Data Collection Instrument
The data was collected using a self-administered questionnaire. The questionnaire has the following parts.
Section 1
Demographic Data of the Participants
The demographic data included age, marital status, educational status, number of children, and occupation.
Section 2
Corona Virus Anxiety Scale
CAS is a seven-item scale used to assess the COVID-19 related anxiety. The scale indicates 0 = not applicable to me, 1 = hardly ever applicable to me, 2 = sometimes applicable to me, and 3 = very applicable to me. The score above 9 in total or high in one individual item is considered as anxiety. The content validity coefficient of the tool is 0.97 (Lee, 2020).
Pilot Study
Pilot study was done with 10 samples. The study was practicable and feasible; hence no changes were done on the tool or method of data collection.
Description of Intervention
The CBT was developed in consultation with the clinical psychologist and counsellors. A standard checklist was used while developing the intervention. The intervention followed all the steps stipulated in the standard practice guidelines of delivering CBT. It included the following major steps: cognitive conceptualization (establishing rapport, checking mood, providing information on CBT techniques and its benefits and maintaining a CBT dairy, expectations from the patient and counsellor, collecting any relevant or additional information to plan for upcoming session, information on automatic thoughts, their situation, related behaviors, and emotions due to COVID, and any physical responses they experience, demonstrating deep breathing techniques, relaxation techniques and mindfulness, instructions to do the techniques daily and summary and feedback from patient); structuring and shifting thoughts (checking mood and dairy maintenance to bridge previous session, working on thoughts and beliefs, talking about Holy Quran and prayers, guided discovery of thoughts and fears relating to COVID, deactivation techniques to neutralize their thoughts from COVID, continuation of demonstrating deep breathing techniques, relaxation techniques and mindfulness, summary and feedback from patient); termination session (review of goals, checking patient's improvement, discussion of outcomes and summary and feedback from the patient).
The CBT was delivered to participants via virtual mode. Three sessions of CBT each lasting for 30–50 min was delivered. After the first session, the second CBT session was done on the 7th day and the 3rd session was delivered on the 14th day. On the same day after session 3, the post-test was conducted using the same CAS scale. The CBT sessions were offered by the researchers who are professionally trained counsellors to offer CBT sessions. Practice of all these measures every day till the next meeting was emphasized. All these techniques were demonstrated by the researchers and got the re-demonstration done by the participants.
The participants had various kinds of fear related to COVID-19. Therefore, the authors facilitated the expression of fears by the participants and they were grouped. For example, the participants had a fear of losing loved ones as they came across many deaths in their neighborhood. The counsellors emphasized that there was no scientific rationale for their fear. Participants were encouraged to stay away from overuse of social media news relating to COVID 19, which was verbalized as a major stress and anxiety by the respondents.
Adolescents had difficulty following social distancing which was a major concern among the participants in this group. Fear of vaccination and its effects was another major cause of stress and anxiety from social media messages. Participants had questions on side effects of the vaccination and protection it offered. The counsellors focused on these and proceeded with the discussion. Bringing the client to the “now” or “present” was the focus. The researchers used Balushi/Arabic language depending on the language, the participants spoke. Women were more enthusiastic than men to attend the CBT sessions. Participants were hesitant to accept any intervention at the start of the study. However, the participants eagerly participated later. There was no compensation provided for participating in the study. However, the participants and their family were briefed on the benefits of participating in CBT session.
Data Collection Procedure
An invitation to participate in the study was sent to the Omani public through Facebook and What's app. The interested participants communicated to the researchers of their interest in participating in the study. An implied informed consent was given by the participants by accepting to fill the questionnaire. Google form comprising of the informed consent, information sheet, demographic data sheet, and CAS tool was sent through e-mail/What's app. Participants who had a score of greater than 9 in total or high score in any one component of the CAS were chosen as a study participant.
The CBT intervention was delivered by the investigators of the study who are certified in delivering CBT. The CBT intervention was structured and validated by experts. A total of three sessions of CBT lasting for 30–50 min were given. The post-test was conducted using the same CAS scale. The participants who had CAS score above 9 after three CBT sessions were referred to Sultan Qaboos University Hospital (SQUH) for further follow-up. Only one participant was refereed to SQUH for further management.
Data Checking and Cleaning Procedure
The investigators ensured that only the potential participants of the study responded to the survey. The investigators invited the participants who responded to the survey for a virtual meeting and confirmed their responses. Moreover, the willingness of the respondents to participate in the CBT session was confirmed during this virtual meeting. This strategy eliminated the bias in the study. Since the CAS was a five-item scale and took short time for the response, there were no incomplete responses. However, we had six dropouts as they did not attend all three CBT sessions. These dropouts were replaced with additional samples to meet the sample size requirements.
Statistical Analysis
The data were analyzed using descriptive and inferential statistics. The data were entered into SPSS (Statistical package for social sciences) version 19. Percentage and graphs were used to interpret the demographic data. Chi-square test, and paired ‘t’ test were used to compare the selected demographic data with the pre- and post-levels of COVID related anxiety.
Results
Sample Characteristics
The demographic data of the participants are presented in Table 1. Majority of the study participants (58.9%) were in the age range of 31–60 years. A large number (68.4%) of participants were married. Most (53.7%) of them had 1–5 children. Of the participants, 47.4% of them had completed their undergraduate education.
Demographic Variables of the Participants.

The respondents who are more than 60 years of age had higher levels of anxiety, followed by the respondents in the age group between 18 and 30 years of age. The respondents who had their post-graduation had lower levels anxiety followed by respondents who had their secondary education. The respondents who were part time employees had lower anxiety level than the respondents who were working full time.
Research Question Results
A Chi-square test which compared the marital status and level of anxiety before and after the intervention showed that there was no relationship between marital status of the respondents and pre-test anxiety level (0.215). Meanwhile, relationship existed between post-test level of anxiety and their marital status (.003). This means that the Omani respondents who were married had lower anxiety (46.45) after intervention.
The test of significance between age of respondents and level of anxiety before and after the CBT revealed that there is no significant difference between the age of the respondents and pre (.001) and post-test (.004). Before the CBT, the respondents who were between 31 and 60 years of age had higher anxiety towards the pandemic (13.52), followed with the respondents from the age group between 18 and 30 (12.88) and respondents more than 60 years of age (12.43). However, after the CBT, the respondents who were more than 60 years of age had higher anxiety towards corona (6.71), followed by the respondents in the age group between 18 and 30 years of age (6.47) and between 31 and 60 years (6.23). This means that after CBT, the younger generation had a better understanding of the pandemic and were able to cope up with COVID-19 anxiety.
However, the analysis done to compare the number of children of the respondents and their level of anxiety before and after CBT indicated that there was a significant difference between the number of children of the respondents and pre-test (.704) and post-test (.880). This means that the respondents who had more children and a larger family size had higher anxiety than others as they were concerned if their family would suffer if they contracted the COVID-19 infection.
The authors also compared the educational qualification of respondents and their level of anxiety before and after CBT and showed that there was a significant difference between educational qualification of the respondents before and after CBT. Meanwhile, relation exists between educational qualification of the respondents and post-test values after intervention at .000 level. After the CBT, the respondents who had post-graduation (5.20) had lower anxiety followed by respondents who had secondary education (6.22), UG (6.53), and primary education (6.62) (Table 2).
Comparison Between Educational Qualification of the Respondents and Level of Anxiety During Pre-test and Post-test.

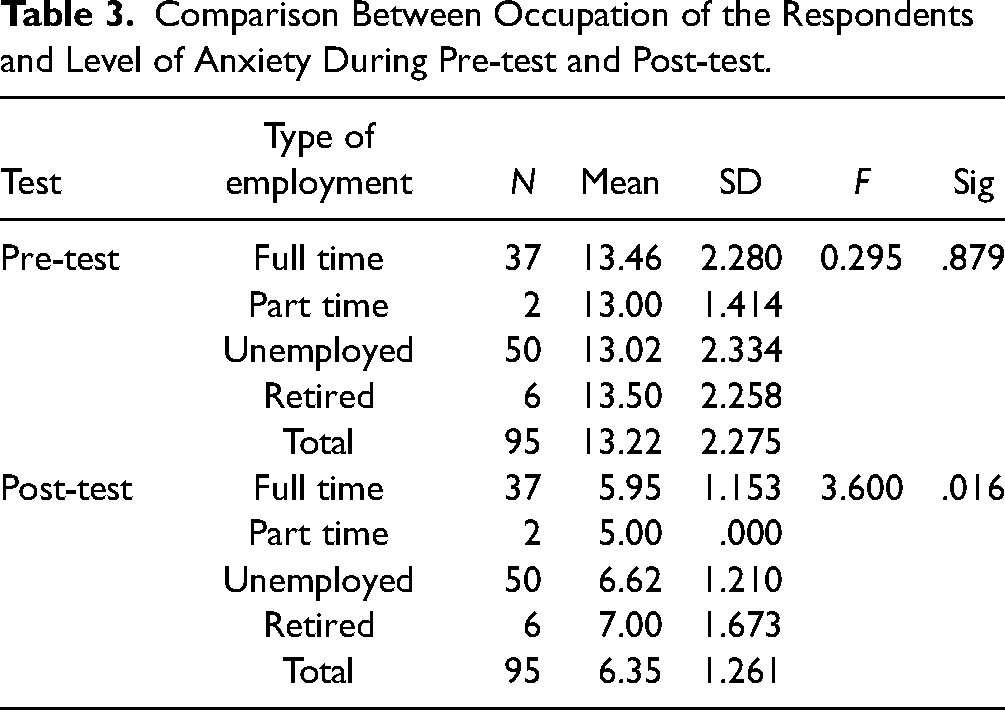
The occupation of respondents and their level of anxiety before and after interventions revealed that there was a significant difference between type of occupation of the respondents before and after CBT therapy (.879). Meanwhile, relation exists between type of occupation of the respondents and post-test (.016). After CBT therapy the respondents who were part time employees (5.0) had lower anxiety than respondents who were working in full time (5.95), who were unemployed (6.62) and who were retired (7.0) (Table 3).
Comparison Between Occupation of the Respondents and Level of Anxiety During Pre-test and Post-test.
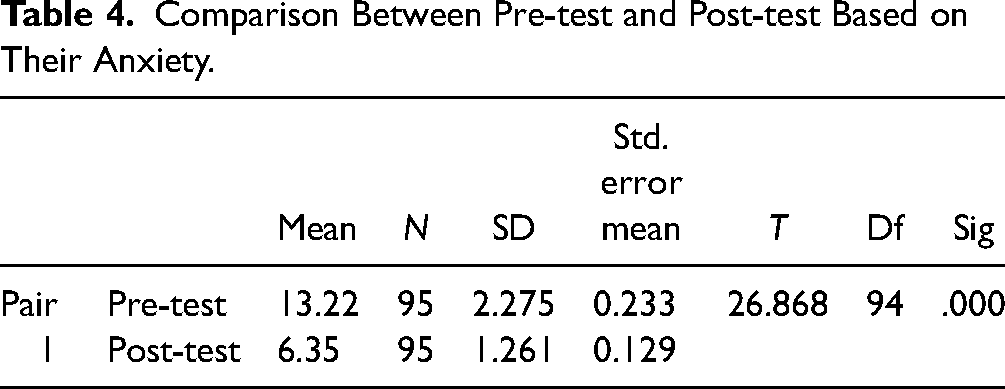
A paired ‘t’ test before and after the CBT revealed that a relationship exists between pre- and post-test conducted among the respondents (.000 with value at 26.868). It reveals that the level of anxiety reduced after CBT (6.35) compared to pre-test (13.22) (Table 4).
Comparison Between Pre-test and Post-test Based on Their Anxiety.
Discussion
In the present study, the participants who are more than 60 years of age had higher levels of anxiety followed by the respondents in the age group between 18 and 30 years of age. In consistent to this study findings, few other study findings showed that the anxiety level was higher among people less than 25 years of age and people who are aged more than 60 years (Gambin et al., 2021; Nwachukwu et al., 2020; van den Besselaar et al., 2021). Younger adults may be exposed to more information through social media, which may increase their level of anxiety. Moreover, the loss of social connection with their friends may increase the vulnerability to anxiety (Gao & Zheng, 2011). Likewise, the older adults may be at risk of developing higher levels of anxiety as greater levels of mortality have been reported among elderly (Qiu et al., 2020).
In the current study, the respondents who had their post-graduation and were part time employees had lower level of anxiety than the respondents who were working full time. In consistent to this study finding, another study reported that people with increased resilience and emotional wellbeing will be able to cope up with this pandemic related stress and anxiety better than others (Beckstein et al., 2022). This citation can be correlated with the present study findings that Omani population with a post-graduate education and who worked part time had lower anxiety and coped better than the other participants, assuming that these populations might have had increased resilience and wellbeing due to their educational and occupational status. However, a research conducted in Vietnam showed a contrasting result about educational level of participants and COVID-19 related anxiety. In this cited research, participants who had high educational level had more anxiety as they have invested more on their education and were worried about their loans to be paid off, getting a new job and so on (Le et al., 2020). Likewise, another study conducted in United Kingdom found that higher education poses greater financial stress and worst mental health outcomes (McCloud & Bann, 2019). Thus, these contradictory findings should be explored further to understand the role of educational status on COVID-19 related anxiety.
The results in the current study indicated that the larger family size and respondents who had more children experienced higher level of anxiety than others. This finding is in par with the research carried out, where participants who had a larger family size experienced more anxiety and depression rates than others (Le et al., 2020). The reason could be that they are worried about their family members contracting the disease or will need to isolate. Earlier research also showed that social isolation and loneliness would likely to be seen in older, divorced, people with low educational status, un-employed, and people living with more number of children (Ge et al., 2017). Future studies are recommended to understand more on the relationship between larger family size and higher levels of anxiety in particular during this COVID-19 pandemic.
CBT is a flexible method to manage a range of mental health conditions due to the COVID-19 pandemic (Surmai & Duff, 2022). Moreover, the goal of CBT is to build and restore resiliency (Apolinário-Hagen et al., 2020; Craske, 2021; Paredes et al., 2021). As cited, the investigators delivered CBT sessions to the participants identified to have COVID-19 related anxiety to enhance their mental wellbeing. The present study revealed that COVID-19 related anxiety significantly reduced after the CBT intervention. Thus, the null hypothesis formulated in the current study was rejected as the virtual CBT showed significant difference between the pre- and post-intervention.
CBT has superior benefits and improves sleep, relieves fatigue, enhances confidence, and improves quality of life in people with pandemic related anxiety. CBT is more effective for people who are under social isolation and receiving virtual health care (Surmai & Duff, 2022). Considering the enormous benefits of CBT, the researchers delivered the CBT intervention virtually to people who were suffering from moderate to severe anxiety. Web-based psychological interventions and internet-based CBT interventions are beneficial in addressing mental health issues (Cheng et al., 2019; Rose et al., 2013). These supportive literatures are in support to the present study that virtual CBT shall be a best strategy in dealing people with mental health issues.
In support to the current study finding, several other studies indicate that CBT improved the mental health outcomes in different population. Significant decrease in depression, anxiety, and stress were found after CBT intervention. The study found that the overall psychological health improved in the patients (Li et al., 2020). In medical students, CBT intervention showed significant improvement in mental health status, enhanced physical activity level, and longer sleeping hours. Moreover, these students had lower levels of depression, anxiety, and social dysfunction after the CBT intervention (Hanani et al., 2022).
Additionally, online CBT was found to be a best strategy in managing COVID-19 related psychological issues in adults experiencing depression and anxiety. Likewise, virtual CBT is very effective for patients who are reluctant to participate in the treatment in the clinical setting due to stigma (Mahoney et al., 2021). This makes it very clear that CBT is a highly effective mental health intervention that promotes the psychological wellbeing of people experiencing COVID-19 related anxiety and other associated mental health conditions. These findings propose that adequate attention must be paid to the mental health of the people during the pandemic crisis and virtual CBT programs can be used for the management of mental health problems.
Strengths of the Study
This was the first interventional study carried out in the Sultanate of Oman to reduce COVID-19 related anxiety among people who were in lock down, socially distanced, and working from home. As it was conducted virtually, it enhanced the participation among the people with COVID-19 related anxiety.
Limitations of the Study
The limitation in this study was that it was difficult to carry out face-to-face CBT sessions, which would have otherwise increased more participant interaction during the study. In this interventional study, one of the methodological limitations was non-randomization of participants, which limits the representativeness of the sample. The counsellors faced network and connectivity issues while the CBT sessions were offered virtually.
Implications for Practice
The authors recommend conducting similar studies in future considering more representative sample across the Sultanate of Oman. Age-specific CBT sessions shall be designed and their efficacy on COVID-19 anxiety shall be tested. The nursing educators shall consider including the integration of virtual counselling sessions for people with various psychological disorders in the nursing curriculum. This will make the people with psychological disorders feel comfortable approaching the nurses as they don’t feel stigmatized visiting the healthcare facilities for psychological issues. The policy makers shall encourage the healthcare facilities to initiate telenursing facilities, which would encourage the people with psychological issues reaching out to the telenursing facilities on time and their psychological wellbeing shall be preserved and quality of life shall be enhanced. Additionally, public messages and communication on the use of CBT for COVID-19 anxiety can be encouraged by Government and policy makers. The policy makers shall work with community partnership groups to integrate CBT sessions in the healthcare delivery system to relieve anxiety among people.
Conclusion
The study proved that virtual CBT reduced COVID-19 related anxiety among Omani population to a greater extent. The results also highlight the need for integrating CBT intervention in managing the psychological issues. The study findings recommend developing planned CBT using mobile technology, which would benefit the whole Omani population. Additionally, telenursing facilities shall be initiated in the healthcare facilities, which will enhance the accessibility and affordability of mental health services by the people with psychological health needs.
Footnotes
Acknowledgments
We would like to thank the Omani population from various governorates of Oman who participated in the study. We appreciate the help and thank the mental health counsellors who volunteered to support our study. A special thanks to Noora Nasser Ali Al Souli who is a clinical psychologist who helped us in the conduct of this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical committee approval was obtained from RERAC, Ministry of Health, Oman (MOH/DGPS/CSR/PROPOSAL/APPROVED/81/2020 dated 13.10.2020).