
Abstract
Background
Nurses who work with COVID-19 patients may suffer high levels of work-related stress, anxiety, and depressive symptoms. These impacts raise concerns about the deterioration of their mental health during this time.
Objective
This study examines the relationships between psychosocial factors (health, behavior, social, and economic factors) and mental health on among nurses working in a COVID-19 ward in Japan.
Design
A cross-sectional questionnaire-based study design was adopted.
Methods
We randomly selected 41 general hospitals that had over 400 beds. The participants were nurses who cared for COVID-19 patients at five hospitals. The questionnaire was completed by 56 nurses (seven men and 49 women) (response rate 46.6%). The survey asked participants about their basic attributes (gender, age, years of experience). It also included the Japanese version of the Patient Health Questionnaire-9, the Japanese version of the Generalized Anxiety Disorder-7, the Japanese version of the Impact of Event Scale-Revised, and the Maslach Burnout Inventory-General Survey to measure depression, anxiety, trauma experience, and burnout, respectively. To determine psychosocial factors, perception of damage from harmful rumors, nurses’ intention to quit their jobs, working environment changes, and changes in daily life were measured.
Results
Intention to quit was specifically associated with “wanting to continue nursing,” the posttraumatic stress disorder (PTSD) symptom of avoidance, depression, anxiety, and burnout. Nurses who had experienced the impact of harmful rumors in the workplace had high levels of PTSD symptoms, including intrusion, avoidance, and hyperarousal, as well as depression, anxiety disorder, and burnout cynicism. Regarding changes in the working environment, significant differences were confirmed in PTSD symptoms including intrusion, avoidance, and hyperarousal, as well as depression. We also examined the relationship between changes in daily life and mental health. We found that answering affirmatively to “the family income has decreased,” “I’ve had family problems,” and “I cannot do housework” related to mental health disorders among the nurses.
Introduction
In December 2019, the first known case of pneumonia caused by a novel coronavirus was reported in Wuhan, China. On January 30, 2020, the World Health Organization (WHO) declared a Public Health Emergency of International Concern regarding the outbreak. Reports of a new type of pneumonia caused by a novel coronavirus (“Coronavirus Disease 2019” or “COVID-19”) that had spread both domestically and internationally continued to rise (WHO, 2020). As of June 27, 2022, 9,253,386 people were reported to have contracted COVID-19 in Japan, with 31,126 deaths (Ministry of Health, Labor and Welfare, 2022). Within this social context, experts have expressed concern regarding the impact of COVID-19 on mental health (Pfefferbaum & North, 2020).
Literature Review
The mental health of nurses caring for COVID-19 patients has been previously studied (Ohue et al., 2021). In China, a pioneer in COVID-19 medical care, Lai et al.'s (2020) report noted that healthcare professionals involved with COVID-19 patients in Wuhan experienced psychological burden and that, in particular, several female nurses and healthcare professionals working on the front lines suffered mental health deterioration and experienced posttraumatic stress disorder (PTSD), depression, anxiety, and sleep disorders. The review further indicated that frontline healthcare workers dread not only the possibility of spreading COVID to their families but also the highly stressful shifts that they work (Ruta et al., 2021). Such findings highlight the importance of workplace interventions to support staff members who work on the medical front lines. Cases of burnout have also been reported among healthcare workers caring for COVID-19 patients. In Iran, researchers found that the highly stressed front-line nurses had higher levels of burnout syndrome than other nurses, suggesting that work-related stress is an important factor influencing burnout syndrome among nurses (Sarboozi Hoseinabadi et al., 2020).
Shigemura et al. (2020) argued that although COVID-19 is a new infectious disease, and by regarding the pandemic as a type of chemical, biological, radiological, nuclear, and high-yield explosives disaster (CBRNE disaster), it is possible to apply the lessons learned during other CBRNE disasters to current cases. Shigemura et al. (2020) also discussed the impact of CBRNE disasters on a person's health (mental and physical health), behavior, and social and economic psychosocial factors. Accordingly, we sought to examine the impact of COVID-19 on nurses who care for COVID-19 patients in terms of health, behavior, and social and economic factors to deeper our understanding of the psychosocial effects. These psychosocial factors may be associated with mental health phenomena (PTSD, anxiety, depression, and burnout).
We aimed to conduct an exploratory analysis of the relationship between psychosocial factors and mental health among nurses who treat COVID-19 patients while working at a hospital ward in Hyogo, Japan.
Methods
Design
This study adopted an analytical cross-sectional survey-based design that was conducted from August 4, 2020, through October 26, 2020. An online structured survey was used. In this study, psychosocial factors were the independent variables, whereas mental health factors (i.e., PTSD, depression, anxiety, and burnout) were the dependent variables.
Research Question
This study explored the following research question: How are the psychosocial factors (i.e., health, behavior, society, and economy) of nurses caring for patients with COVID-19 related to mental health?
Sample
We randomly selected 41 general hospitals that had over 400 beds, operated respiratory medicine departments, and had infectious disease wards from among the 336 hospitals registered in Hyogo, Japan. We contacted the heads of nursing in each of these hospitals and obtained consent from 120 nurses at five hospitals. The sample size was 332, with tolerance (5%), response rate (30%), and confidence (95%). Notably, it was difficult to collect responses to the questionnaire owing to the impact of the pandemic. With a sample size of 56 and a response rate of 46.6%, a 90% confidence interval and 10.9% allowable error were calculated.
Inclusion/Exclusion Criteria
The inclusion criteria for participation in this study was being a registered nurse caring for patients with suspected or confirmed COVID-19 infection. Nurses caring for patients with moderate to severe COVID-19 were included, while those caring for those with mild infections were excluded. Registered nurses who were not caring for patients with suspected or positive COVID-19 or those who had only previously been involved with these patients were excluded. Nurses who already had mental health disorders were also excluded.
Instrument
Information on participants’ basic attributes was collected, including their gender, age, years of experience, department, marriage status, and presence/absence of children.
Mental Health Indicators
To measure PTSD, we used the Japanese-language edition of the Impact of Event Scale-Revised (IES-R). The reliability (Cronbach's α = .92) and validity of the IES-R were verified by Asukai et al. (2002). The IES-R is a self-administered questionnaire that measures PTSD levels. It was developed to match the diagnostic criteria for PTSD in the Diagnostic and Statistical Manual of Mental Disorders and comprises three subscales that include a total of 22 items, specifically intrusion symptoms (seven items), avoidance symptoms (eight items), and hyperarousal symptoms (seven items). Respondents evaluate the intensity of their symptoms during the past week on a five-point Likert scale. PTSD level is then measured by calculating the total points for each subscale or by the total of points across all subscales. The higher the score, the stronger the posttraumatic stress symptoms are reported.
The Patient Health Questionnaire-9 (PHQ-9), developed by Kroenke et al. (2001), aims to diagnose depression and assess the degree of its severity. We used Muramatsu et al.'s (2018) revision of Muramatsu's (2014) Japanese translation edition; the reliability and validity of this version have been confirmed, with kappa values ranging from 0.70 to 1.0 for major depressive disorder (Muramatsu et al., 2007). The PHQ-9 comprises nine items. Participants evaluate their symptoms on a four-point scale, from 0 = no days that apply whatsoever to 3 = almost every day. The total points are then calculated for this scale; the higher the total score, the stronger the respondent's depressive symptoms.
The Generalized Anxiety Disorder-7 (GAD-7) instrument, developed by Spitzer et al. (2006), is a questionnaire designed to assess generalized anxiety symptoms. We used the Muramatsu (2014) edition of the Muramatsu et al. (2010) Japanese translation; its reliability and validity, with a sensitivity of 89%, a specificity of 82%, and a high Cronbach's α value of .9, have been confirmed. Respondents are asked to evaluate their symptoms on a four-point scale, from 0 = no symptoms whatsoever to 3 = almost every day. Total points are then calculated for this scale; the higher the score, the greater the respondent's anxiety level.
The Maslach Burnout Inventory-General Survey (MBI-GS) was developed by Schaufeli et al. (1996). We used Kitaoka et al.'s (2011) translated edition; its reliability (α = .80) and validity (Correlation with CES-D r = −.24 to .62) have been verified. The MBI-GS includes three subscales: emotional exhaustion (five items), depersonalization and cynicism (five items), and professional efficacy (six items). Total points are calculated for the scale, with high emotional exhaustion and depersonalization/cynicism scores and low professional efficacy scores indicating burnout.
Psychosocial Factors
We referenced the psychosocial factors used by Shigemura et al. (2020) to analyze the impact of CBRNE disasters and included the following items that corresponded to the circumstances of the participating nurses. Since this framework is often used in the event of a disaster, we believe that validity and reliability have been ensured (Farhat et al., 2022).
Data Collection
We drafted the questionnaire using Google Forms software (paid version) and generated a QR code for it. We explained the objectives of our research to the hospital nursing department directors at 41 hospitals, both in writing and verbally, and obtained consent from five of them. We mailed a written explanation and questionnaire sheets with the QR code to the nursing department directors who had provided their consent. The nursing department directors then distributed the questionnaire sheets with the QR code to the targeted nurses. After receiving those documents, nurses who were able to participate in the research accessed the questionnaire using the QR code and answered the questions online.
Statistical Analysis
We examined how the psychosocial factors (health, behavior, society, and economy) of nurses caring for patients with COVID-19 infection were related to mental health. The significance level was set at p < .05. We used IBM SPSS Statistics 26 statistical software to perform the calculations.
We calculated descriptive statistics to identify participants’ basic attributes. Shapiro–Wilk test results, p < .05, confirmed that the participants did not follow a normal distribution pattern. As such, we used Spearman's rank correlation coefficient to investigate and analyze the relationship between participants’ mental health and their intention to quit their jobs, the relationship between experiences with the damage caused by harmful rumors and mental health, and the relationship between changes in the working environment and mental health. We used the Mann–Whitney U-test to analyze the relationship between changes in nurses’ daily lives and their mental health.
Ethical Considerations
This study was conducted after obtaining approval from the Hyogo University Ethical Review Board (No. 20004). A written research request was sent to the institution where the study was to take place. After obtaining approval, participants received written explanations of the research. Only participants who provided written consent were included in the study.
Results
Participants’ Basic Attributes
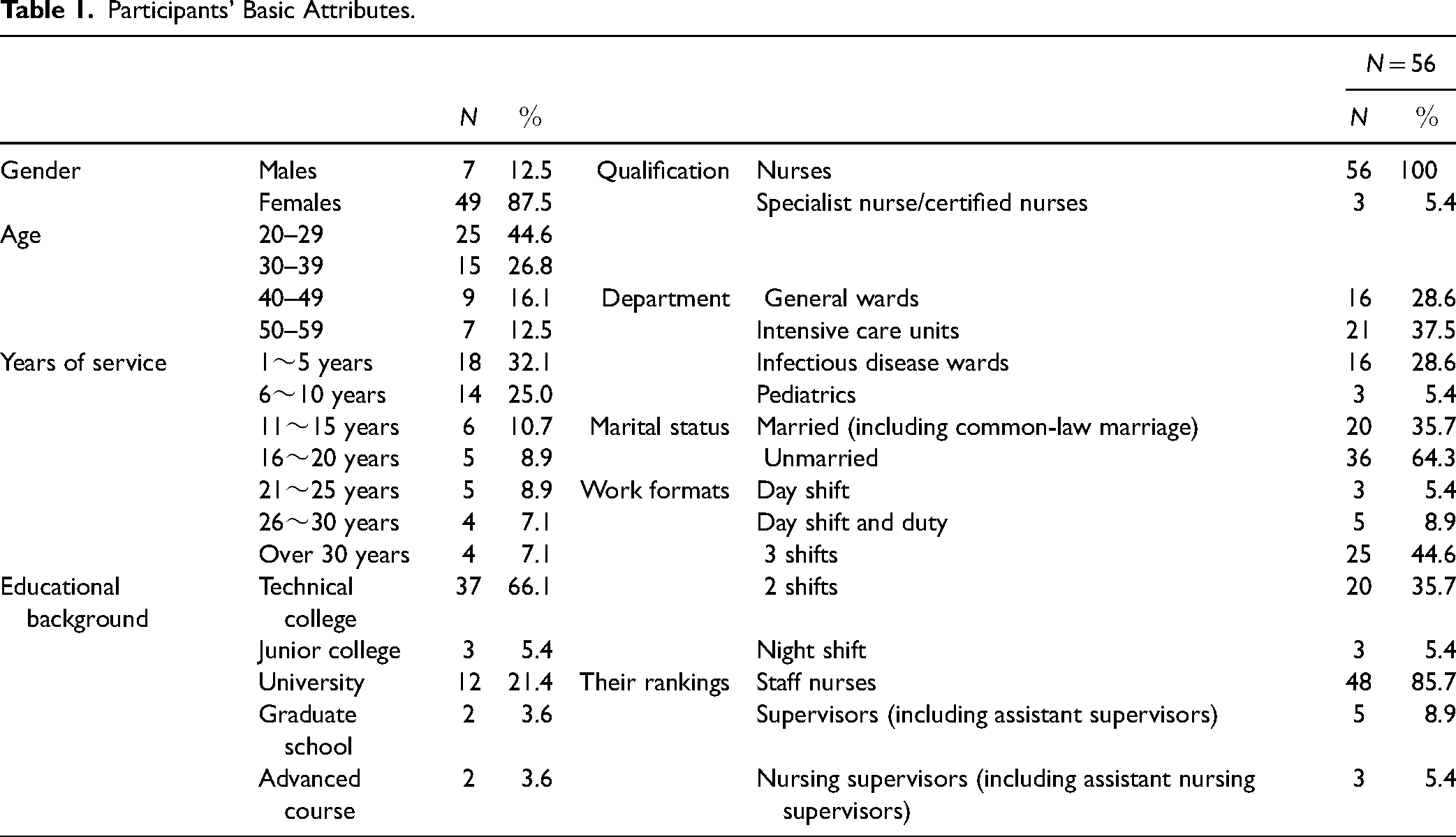
The participant group was comprised of seven men (12.5%) and 49 women (87.5%). Most participants were from 20 to 29 years old (n = 25; 44.6%), followed by 30–39 years old (n = 15; 26.8%). The highest percentage of the group had worked 1–5 years (n = 18; 32.1%), followed by 6–10 years (n = 14; 25.0%; Table 1).
Participants’ Basic Attributes.
Relationship Between Mental Health and Intention to Quit Job
Spearman's rank correlation coefficient was calculated to confirm the relationship between mental health (PTSD, depression, anxiety disorder, and burnout) and intention to quit (Table 2). The item “I want to quit my job as a nurse” had a positive significant relationship with cynicism and a negative significant relationship with professional efficacy. The item “I want to change my hospital and/or department” had a positive significant relationship with cynicism and a negative significant relationship with professional efficacy. Finally, the item “I want to continue working as a nurse” had a negative significant relationship with avoidance, depression and anxiety disorder symptoms, emotional exhaustion, and depersonalization/cynicism, and a positive significant relationship with professional efficacy.
Relationship Between Mental Health and Intention to Quit job.

Note. Spearman's rank correlation coefficient. IES-R = Impact of Event Scale-Revised; PHQ-9 = Patient Health Questionnaire-9; GAD = Generalized Anxiety Disorder-7; MBI-GS = Maslach Burnout Inventory-General Survey.
Relationship Between Awareness of Damage Caused by Harmful Rumors and Mental Health
We calculated Spearman's rank correlation coefficient to investigate the relationship between the participants’ awareness that harmful rumors can cause damage and their mental health (Table 3). The results confirmed positive relationships, with significant differences, between this awareness and PTSD symptoms such as intrusion, avoidance, hyperarousal, depression, and anxiety disorder, and with the depersonalization/cynicism burnout subscales.
Relationship Between Awareness of Damage Caused by Harmful Rumors and Mental Health.

Note. Spearman's rank correlation coefficient. IES-R = Impact of Event Scale-Revised; PHQ-9 = Patient Health Questionnaire-9; GAD = Generalized Anxiety Disorder-7; MBI-GS = Maslach Burnout Inventory-General Survey.
Relationship Between Changes in Working Environment and Mental Health
We calculated Spearman's rank correlation coefficient to investigate the relationship between changes in the working environment and mental health (Table 4). The results confirmed a significant positive relationship between changes in the working environment and PTSD, and between changes in the working environment and PTSD symptoms including intrusion, avoidance, hyperarousal, and depression. A negative significant relationship was confirmed between changes in the working environment and professional efficacy.
Relationship Between Changes in Working Environment and Mental Health.

Note. Spearman's rank correlation coefficient. IES-R = Impact of Event Scale-Revised; PHQ-9 = Patient Health Questionnaire-9; GAD = Generalized Anxiety Disorder-7; MBI-GS = Maslach Burnout Inventory-General Survey.
Relationship Between Changes in Daily Life and Mental Health
We performed the Mann–Whitney U-test using the participants’ change status (Yes/No) and various mental health factors to investigate and analyze the relationship between the changes in daily life and mental health (Table 5). We found that answering affirmatively to “the family income has decreased,” “I’ve had family problems,” and “I cannot do housework” was related to mental health disorders among the nurses.
Relationship Between Changes in Daily Life and Mental Health.

Note. IES-R = Impact of Event Scale-Revised; PHQ-9 = Patient Health Questionnaire-9; GAD = Generalized Anxiety Disorder-7; MBI-GS = Maslach Burnout Inventory-General Survey.
Discussion
Relationships Between Mental Health and Intention to Quit
In investigating the relationship between mental health and intention to quit, we found that (a) intention to quit was significantly related to the depersonalization/cynicism and professional efficacy factors in the burnout subscales, (b) wanting to change hospitals and/or departments was significantly related to the depersonalization/cynicism factors in the burnout subscales, and (c) wanting to continue working as a nurse was significantly related to depression and anxiety disorder and the emotional exhaustion, depersonalization/cynicism, and professional efficacy factors in the burnout subscales.
Ohue et al. (2021) reported a high incidence of mental health problems among nurses caring for patients infected with COVID-19. In this study, some of the nurses involved in treating COVID-19 patients may have transferred from other departments and may have had a strong sense of mission and motivation. This may be why, even with deteriorating mental health, the participants that wanted to continue working as nurses outnumbered those who wanted to quit. According to a report by the Japanese Nursing Association (2020a), 15.4% of all hospitals in Japan reported staff members resigning because of working environment changes related to COVID-19 countermeasures and infection risk. Notably, 21.3% of medical institutions designated for the treatment of infectious diseases reported similar staff resignations, which was higher than for other hospital types. These resignation behaviors can affect the nurses who continue to work, creating a vicious cycle of reduced organizational commitment and increased instances of burnout, leading to additional resignations (Wang et al., 2020).
As such, measures to discourage nurses involved with COVID-19 patients from quitting their jobs are necessary. Fear of the disease, serious resource shortages, social isolation, large-scale and expanding financial losses, and increased uncertainty are all related to wide-ranging psychological pain, and thus, nurses caring for COVID-19 patients face an increased risk of mental illnesses and behavioral disorders (Pfefferbaum & North, 2020). To further this point, various factors that have been found to influence one another can cause a declining mindset among nurses who were initially highly motivated, impacting their desire to continue working as nurses. Reinforcement of nurses’ mental health support systems is required to effectively prepare for future pandemics or other disasters.
Relationship Between Experience With Damage Caused by Harmful Rumors and Mental Health
We investigated the relationship between experiences with damage caused by harmful rumors and mental health. Our results indicate that nurses who experienced damage from harmful rumors had high scores for PTSD symptoms including intrusion, avoidance, hyperarousal, depression, and anxiety disorder, and the depersonalization/cynicism factors in the burnout subscales. According to Japan Medical Association (2021), nurses suffer from this type of damage more often than other professionals. Japanese Nursing Association (2020b) reported that healthcare professionals carry extremely heavy burdens at medical practice sites and when discrimination and prejudice are added, mental and physical exhaustion are further intensified. The Association further noted that these factors ultimately lead to healthcare professionals quitting their jobs, which places the entire medical system at risk of collapse. The present study confirms this finding.
There is a growing concern in Japan about healthcare professionals who work with COVID-19 patients suffering damage from harmful rumors associated with the circumstances, which perpetuate many anxiety-provoking. Matsui (2017) studied support activities carried out by psychologists in the wake of the Great East Japan Earthquake, and found that the harmful rumors that accompanied the major earthquake increased anxiety about the impact of radiation among members of the public, even those living far away from the disaster-stricken areas. However, Matsui (2017) concluded that such rumors can be suppressed through the dissemination of accurate information and by supporting attitudes that favor rational decision-making. Shigemura et al. (2020) argued that if people understand their psychosocial reactions to COVID-19 as “reactions that can occur with invisible disasters” rather than “strange and enigmatic reactions,” it may contribute to alleviating their anxieties. By acknowledging that psychosocial reactions to COVID-19 are “normal” reactions to invisible disasters and by releasing accurate information in a coordinated fashion, the damage to others from such harmful rumors can be minimized. More specifically, we posit the need to build a system that enables the release of accurate information and to create support systems that can contribute to alleviating the anxieties of residents of an area.
Relationship Between Working Environment Changes and Mental Health
In investigating the relationship between working environment changes and mental health, we observed a significant relationship between the working environment having “Changed dramatically” and total incidences of PTSD, as well as with PTSD symptoms such as intrusion, avoidance, hyperarousal, and depression. Participants also noted specific differences in the workplace environment, including “The makeup of the ward has changed” and “People around me such as my superiors and subordinates, etc., were transferred to other departments.” When admitting COVID-19 patients, hospitals were compelled to reorganize wards and change the nurses’ staffing. Sudden and drastic changes of this kind in the working environment have been found to affect nurses’ mental health. For example, Kunii et al. (2017) investigated events—although not a pandemic—during which nurses suffered mental health disorders. Among the nurses they surveyed, statements about working environment problems were more prevalent than statements on interpersonal relationship problems. This finding illustrates the influence of the working environment on mental health and may help explain why COVID-19-related working environment changes may have subjected nurses to considerable stress.
The most significant difference between nurses who experienced dramatic changes in their working environment and those who did not was found with respect to PTSD. McCarroll et al. (1993) reported that people who have witnessed numerous deaths and have seen people close to them die are at high risk of PTSD; thus, nurses with high PTSD scores in this study may have been confronted with the deaths of several patients who were infected with COVID-19. This may explain why nurses whose working environment had changed had higher PTSD scores than nurses whose working environment had not changed. Various other factors are involved, such as stress associated with environmental changes and a lack of support to ease the formation of new interpersonal relationships. We recommend that in preparation for future pandemics and disasters, support systems for coping with such changes in the working environment are established.
Relationship Between Daily Living Changes and Mental Health
We investigated the relationship between nurses’ daily living changes and their mental health. Our results suggest that the following items are related to mental health disorders, such as depression, anxiety disorder, and burnout: “I eat more than before,” “Food no longer tastes good,” “I’ve become constipated,” “I’ve become socially isolated,” ‘I have trouble sleeping,” “My skin has become rougher from wearing a mask all the time,” “Family income has decreased,” “I’ve had family problems,” and “I can no longer do housework.”
Shigemura et al. (2020) found that amid the looming COVID-19 state of emergency, manifesting intense emotional reactions such as extreme fear and anxiety place people at risk of developing wide-ranging mental health issues, including health-damaging behaviors (increased alcohol and cigarette intake and social isolation), mental diseases (PTSD, anxiety disorder, depression, and somatic symptom disorder), and a decline in the sense of subjective well-being. The present findings support these views. Specifically, digestive symptoms, such as eating more food, food no longer tasting good, and becoming constipated are the result of excessive stress on the autonomic nervous system and are considered symptoms of somatic symptom disorder. We suspect that nurses’ confirmation that their rougher-than-normal skin, another physical manifestation of the situation, was the result of being compelled to constantly wash their hands and wear face masks to prevent COVID-19 transmission during daily work.
As nurses continued living lives of self-restraint and self-quarantine owing to the pandemic, family-related problems tended to occur, as indicated by affirmative responses to “Family income has decreased,” “I’ve had family problems,” and “I cannot do housework anymore.” Problems among family members are known causes of increased stress (Holly et al., 2019). Complaints such as “I’ve become socially isolated” and “I have trouble sleeping” are related to depression, mental disorders, and avoidance symptoms of PTSD.
Strengths and Limitations
In the uncertain situation of a pandemic, nurses who answered our questionnaire may have found an outlet to express their worries. We saw this as a strength of our study. Another strength comes from the results of our questionnaire data, which demonstrated that nurses experienced mental health problems during the COVID-19 pandemic.
One limitation of this study is its small sample size. Although we sought a larger sample, many of the hospitals that admitted COVID-19 patients may have been reluctant to offer their cooperation in allowing us to collect data, perhaps as a measure of time protection for the hospital.
Implications for Practice
Ohue and Menta (2022) suggested cognitive behavioral therapy for reducing burnout and intent to quit among nurses. Incorporating such programs in daily operations may improve nurses’ mental health in the event of a future pandemic. Our results showed that the mental health of nurses caring for patients with COVID-19 infection was associated with psychosocial factors; thus, since it is also necessary to reduce psychosocial factors, a mental health support system for nurses should be established. Despite the small sample size, this study's results clearly imply that to prepare for future pandemics or other disasters, supportive communities to protect nurses from rumor damage must be built.
Conclusion
This study targeted nurses who worked at hospital wards and provided care to COVID-19 patients to investigate the impact of mental health on psychosocial (health, behavior, and social and economic) factors. Mental health factors and psychosocial factors were associated with nurses’ intention to quit. In addition, nurses who experienced rumor damage presented high scores for PTSD symptoms including intrusion, avoidance, hyperarousal, depression, and anxiety disorder and for the depersonalization/cynicism factor in the burnout subscales. These nurses also scored significantly higher for PTSD symptoms of intrusion, avoidance, hyperarousal, and depression than nurses whose working environment had only “changed somewhat” or “remained unchanged.”
Our findings suggest that deterioration in mental health was linked to the great upheaval in nurses’ personal and professional lives. The harmful rumors and changes in the working environment of nurses involved with COVID-19 patients affected their mental health and that their mental health, in turn, affected their intention to quit their jobs and their daily lives.
Footnotes
Acknowledgments
This study was carried out with funding from the Japan Association of Private Nursing Colleges 2020 Research Grant for Young Researchers. We wish to express our gratitude to the directors of the participating nursing departments and all the nurses involved for offering their support and cooperation in this research despite the demands of the coronavirus pandemic.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. This work was supported by the Japan Association of Private Nursing Colleges 2020 Research Grant for Young Researchers.