
Abstract
Aim
To determine the effectiveness of topical sesame oil in preventing phlebitis at peripheral IV cannula sites in adult patients within a cardiovascular and cardiothoracic department of a tertiary hospital.
Design
A double-blinded randomized controlled trial was conducted.
Methods
Participants were randomly assigned into control (liquid paraffin oil) and treatment (sesame oil) groups. Randomization was carried out using a Microsoft Excel generated randomized-number table using the RANDBETWEEN function. Five drops of sesame oil or mineral oil was applied to the IV cannula site at 12-h intervals, for a maximum duration of 72 h. A modified Visual Infusion Phlebitis (VIP) scale was utilized to assess for phlebitis severity before every application.
Results
A total of 263 participants were recruited. Six withdrew and seven were excluded after recruitment. 250 participants had their data analysed (121 in the treatment arm and 129 in the control arm). Three participants developed itching after the application of liquid paraffin oil and had their interventions discontinued. Results showed a lower phlebitis incidence in the treatment group (9.1%) compared to the control group (15.5%), though it was not found to be statistically significant (p = 0.12). Additionally, participants who received topical sesame oil experienced phlebitis scores no higher than 2, whereas in the control group, two participants recorded phlebitis scores of 3.
Conclusion
While this research suggests the potential benefits of topical sesame oil in preventing and reducing the severity of phlebitis, further investigation is crucial for more conclusive evidence and broader applicability.
Keywords
Implications
A 12 hourly application of topical sesame oil may be able to halve the incidence and reduce the severity of phlebitis experienced by patients with IV cannulas. This will aid in promoting patient comfort, reducing delays in IV therapy, and reducing healthcare costs, for both patients and healthcare institutions worldwide.
Impact
This study will benefit patients in the area of phlebitis prevention at intravenous cannula sites which is increasingly prevalent in hospitals today. This study found that topical sesame oil reduced the incidence and severity of phlebitis at IV cannula sites which will aid in improving patient satisfaction and lowering healthcare costs incurred by patients and healthcare institutions worldwide.
Reporting method
EQUATOR guidelines and CONSORT checklist were adhered to.
Patient or public contribution
Patients were involved in receiving the treatment and control interventions, and had the presence and severity of phlebitis at their intravenous cannula sites recorded. The data collected from the patients were then analyzed and reported in this study.
What does this paper contribute to the wider global clinical community?
Through this paper we demonstrated the usefulness of topical sesame oil in possibly reducing the risk of phlebitis development at intravenous cannula sites. This illustrates the potential of complementary and alternative medicine in improving the clinical outcomes of patients.
Summary statement
Peripheral intravenous (IV) cannulas are extensively used for administering medications and fluids in hospitals, providing convenience but posing risks such as phlebitis. Phlebitis is a common occurrence in patients undergoing IV therapy and it can lead to many complications and increase healthcare costs. While several topical and systemic therapies have been proposed in literature throughout the years, there is a lack of conclusive evidence on the prophylaxis of phlebitis in clinical practice. This research explores the potential of topical sesame oil, known for its anti-inflammatory and antimicrobial properties, in preventing or reducing phlebitis severity. Prior studies show promising results in specific patient groups receiving IV chemotherapy and IV Amiodarone, but its efficacy in an inpatient cardiac ward setting remains unexplored. A double-blinded randomized controlled trial was conducted on 250 participants with peripheral venous cannulas. Participants were randomly divided into control (liquid paraffin oil) and treatment (sesame oil) groups. Five drops/0.25 mls of sesame oil or mineral oil was applied to the IV cannula site at 12-h intervals, for a maximum duration of 72h. A modified Visual Infusion Phlebitis (VIP) scale was utilised to assess for phlebitis severity before every application. Participants receiving topical sesame oil experienced phlebitis scores lower than that of the control group, thus suggesting that sesame oil could be effective in reducing the severity of phlebitis. A hazard ratio of 0.56 was also obtained, which suggests that at any given time, a subject would be half as likely to experience phlebitis if topical sesame oil is applied to the IV cannula site as opposed to the placebo, liquid paraffin oil. However, although results showed a lower phlebitis incidence in the treatment group (9.1%) compared to the control group (15.5%), it was not found to be statistically significant. In conclusion, A 12 hourly application of topical sesame oil may be able to halve the incidence and reduce the severity of phlebitis experienced by patients with IV cannulas. This could thus aid in promoting patient comfort, reducing delays in IV therapy, and reducing healthcare costs, for both patients and healthcare institutions worldwide. However, while this research suggests the potential benefits of topical sesame oil in preventing and reducing the severity of phlebitis, further investigation is crucial for more conclusive evidence and broader applicability.
Background
The insertion of peripheral intravenous (IV) cannulas for the administration of medications, fluid and blood products is commonplace in hospitals today. 1 Peripheral IV cannulas are minimally invasive and offer physicians and nurses the convenience of administering IV therapy as necessary. 2 However, despite the many therapeutic benefits that IV cannulas offer, they can lead to complications such as infiltration, extravasation, bleeding, bruising, infection and phlebitis.2,3 Of all the complications, phlebitis is one of the most common and has been found to affect 5 to 75% of patients undergoing IV therapy in hospitals.4,5 Phlebitis refers to the inflammation of the venous tract and its surrounding tissues.5,6 It can be caused by mechanical trauma, chemical irritation or infectious microorganisms.5,7 Mechanical phlebitis results when the inserted IV cannula moves within the vein, causing friction and subsequently inflammation. 8 Chemical phlebitis is caused by solutions that are hypertonic (osmolality >500 mOsm/litre) or are too acidic or alkali in nature (pH < 5 or pH > 9). 9 Infective phlebitis results when bacteria penetrate the vein, from the time of insertion or the initiation of IV therapy, and colonise the site, leading to inflammation and in serious cases, systemic sepsis. 10
The signs and symptoms associated with phlebitis include varying degrees of one or more of the following: erythema, pain, oedema, warmth, palpable venous cords, and purulent drainage. 4 Although phlebitis is not a fatal diagnosis, it can cause permanent damage to the venous endothelium, thereby reducing the possibility of administering IV therapy via the damaged vein in future. 11 It has also been found that patients diagnosed with phlebitis after their first IV cannula insertion were 5.1 times more likely to develop post-infusion phlebitis with subsequent cannulations. 12 Additionally, the development of phlebitis often leads to the early withdrawal and reinsertion of the peripheral IV cannula. 6 It can cause a disruption in IV therapy, added stress and discomfort to patients, lengthened hospital stays, 13 and an increase in healthcare costs. 14 As such, the development of a protocol that aids in preventing or reducing the severity of phlebitis in hospitals, is of utmost importance.
While several topical and systemic therapies have been proposed in literature throughout the years, there is a lack of conclusive evidence on the optimal management of phlebitis in clinical practice. 15 Regardless of cause, inflammation of the venous tract and its surrounding tissues will lead to the development and progression of phlebitis-related symptoms at the IV cannula site. As such, the use of anti-inflammatory agents in preventing and treating phlebitis have been widely studied and recommended.16,17
Topical non-steroidal anti-inflammatory drug (NSAID) preparations have been found to be effective in the prevention16,18 and treatment of phlebitis. 17 The use of topical NSAID preparations have been accompanied by reports of adverse effects though,19,20 and being drug-based formulations, they might even be contraindicated for use in certain populations. These may thus not be the most ideal option for use in the prevention of phlebitis.
In contrast, the use of complementary and alternative medicine, has been gaining popularity among medical specialists and the general population worldwide, 21 as a natural and potentially safer form of therapy compared to the use of drugs. Sesame oil is one such example. Extracted from the seeds of the plant species Sesamum indicum L., 22 sesame oil is widely used in traditional medicine in countries such as Iran 23 and Taiwan, 24 due to its anti-nociceptive, anti-inflammatory, anti-bacterial and antioxidant effects.24–26 To date, there have been multiple studies and systematic reviews, exploring the effectiveness of sesame oil in preventing phlebitis27–30 and reducing pain.30–32
A study 27 conducted on patients undergoing chemotherapy, found that phlebitis was eight times more frequent in the control group, where no topical agent was applied, than in the intervention group, where topical sesame oil was applied twice a day. Another study 28 found that sesame oil was effective at reducing the prevalence and severity of phlebitis, for patients on IV Amiodarone. 78% of patients in the control group developed phlebitis with the application of a placebo, as compared to 39% of patients in the treatment group with the application of sesame oil at the IV cannula site. 28 Of these, 6%, 28% and 44% of patients in the control group developed grade 2, 3 and 4 phlebitis respectively, while 17% and 22% of the patients in the treatment group developed grade 2 and 3 phlebitis respectively. A third study 29 compared the effectiveness of sesame oil, Vitamin E and Sanyrene oil on preventing phlebitis. It was found that only 37% of patients who had sesame oil applied at the IV cannula site had developed phlebitis, as compared to 43% of patients who received Vitamin E, and 76% of patients who received Sanyrene oil. Sesame oil was thus found to be twice as effective at preventing phlebitis at IV cannula sites, as compared to Sanyrene oil. 29 To further support these findings, a recent systematic review and meta-analysis of 8 randomized controlled trials (RCT) also reported a 46% lower risk of infusion-related phlebitis (IRP) in treatment groups that received a topical application of sesame oil, compared to that of the control groups. 30 Overall, the systematic review concluded that the coadministration of topical sesame oil alongside routine care, could significantly reduce the incidence, progression and pain severity of IRP. 30
Additionally, a GRADE-assessed systematic review and meta-analysis of 4 RCTs evaluated the use of topical sesame oil on patients with acute limb trauma, and similarly reported that the administration of topical sesame oil, when applied alongside standard treatments, resulted in a significant reduction of pain scores. 31 While the context and patient population of this systematic review differ, these findings seek to reinforce the potential role of topical sesame oil in managing pain and inflammation, which are key components of phlebitis pathology.
It is suggested that the anti-nociceptive, antioxidative, anti-inflammatory and antimicrobial effects of sesame oil, are attributed to the lignans (sesamol, sesaminol, sesamolin, and sesamin), tocopherols and fatty acids it contains.30,32,33 Sesame lignans have been found to hinder the propagation of inflammatory mediators and inflammatory cytokines, 34 and the proliferation of both Gram-negative and Gram-positive bacteria. 35 These properties in turn, conceivably contribute to the effectiveness of sesame oil, in preventing or reducing the severity of phlebitis at IV cannula sites.
Though there are no topical agents to date that have been proven to be effective at completely preventing or treating phlebitis, the evidence on sesame oil leads us to believe that it is a safe, readily available, low-cost, and effective agent, that can be used to prevent or reduce the severity of phlebitis at IV cannula sites. Previous studies have only been carried out on patients receiving IV Amiodarone or chemotherapy. The effectiveness of sesame oil on the general population of patients in an inpatient cardiac ward, however, has never been evaluated – hence the purpose of this study.
Methodology
Study design
This was a double-blinded randomized controlled trial. The aim of this study was to determine the effectiveness of topical sesame oil in preventing phlebitis at peripheral IV cannula sites in adult patients within a cardiovascular and cardiothoracic department of a tertiary hospital.
Ethical considerations
This study was conducted in accordance with the ethical principles outlined by the World Medical Association Declaration of Helsinki. Ethical approval was obtained from the Singhealth Centralized Institutional Review Board (CIRB) on the 24th of February 2022 [CIRB reference number 2021/2804]. Written informed consent was obtained from all study participants prior to enrolment.
Study population
A total of 263 participants who possessed a peripheral venous cannula and were from an inpatient ward within The National Heart Centre Singapore (NHCS) were recruited from April 2022 to November 2022. Recruitment was stopped once the target sample size was met. Participants were recruited, after verbal and written informed consent, if they; were 21 to 80 years of age, spoke and understood either English or Mandarin, and had an IV cannula on the upper extremity that had been inserted a maximum of 12 h prior and showed no signs of phlebitis. Participants were excluded if they possessed: a medical history of allergies to sesame or liquid paraffin oil, venous insufficiency, coagulopathies, cognitive or sensory impairments (due to medical conditions or pharmacological treatments) that would inhibit their ability to rate their pain via a numerical rating scale, or skin conditions that would cause their skin to be red or swollen, and might affect the investigator’s ability to assess for phlebitis. IV cannulas that had been inserted and used for resuscitation were also excluded.
Sample size estimation
The sample size was estimated based on previous studies.27,28 Using a power of 80%, a difference of 15%, and accounting for a 25% attrition rate, a sample size of 250 participants would be required for this study.
Statistical analysis
Clinical and demographic data of the participants were collected. These included: age, gender, ethnicity, size of IV cannula inserted, site of IV cannula insertion and the department in which the cannula was inserted. The STATA software (v.17) was used for data analysis. Descriptive statistics such as frequencies for categorical data, mean and standard deviation for continuous data are presented. Fisher’s exact test was used to compare categorical data between treatment and controls. The cumulative incidences of phlebitis against time-intervals are shown using Kaplan-Meier methods. Log-rank test was also used to test the difference of cumulative incidence of phlebitis between treatment and controls.
Visual infusion phlebitis (VIP) scale
The Visual Infusion Phlebitis (VIP) scale, first developed by Jackson in 1998, 4 then modified by Gallant and Schultz in 2006, 36 was used to assess for the presence and severity of phlebitis at IV cannula sites. It is a numerical scale ranging from zero to five: zero indicating no signs of phlebitis, one indicating the presence of slight pain or redness, two indicating the presence of any two of these symptoms – redness, pain or swelling, three indicating the presence of pain, redness and swelling, four indicating the presence of pain, redness, swelling and a palpable venous cord, and five indicating the presence of pain, redness, swelling, pyrexia and a palpable venous cord. 4 For use in this study, the recommended action corresponding to the VIP score was modified to match the hospital policy in minimising harm to patients - IV cannula sites found to show possible early signs of phlebitis (Grade 1) were advised to be resited instead of observed, thus reducing the risk of developing severe phlebitis. This tool was found to be a valid and reliable instrument in assessing the severity of phlebitis at IV cannula sites. 36 Inter-rater reliability was measured by having 10 nurses independently assess the IV cannula sites of six patients, using the VIP scoring tool. The Cohen’s Kappa coefficient was found to be ≥0.89 which was comparable to the value of ≥0.85 obtained by Gallant and Schultz, 36 and 0.93 which was obtained by Nekuzad et al. 27 Content validity was established by six expert nurses, who have had more than 10 years of experience with assessing phlebitis at IV cannula sites, within inpatient cardiac units.
Treatment allocation
Recruited participants were randomly allocated into two groups via a Microsoft Excel generated randomized-number table using the RANDBETWEEN function, by one unblinded member of the research team. The randomization list was kept under lock and key by this unblinded member, and no other member of the team had access to it.
Intervention
Participants in the control group received topical liquid paraffin oil, while participants in the treatment group received topical sesame oil every 12 h. Liquid paraffin oil (also known as mineral oil) was the choice of control due to it being inert and having no systemic, antifungal, antimicrobial, or anti-inflammatory effects. 37 Apart from the participant number, all treatment and control oil bottles were labelled in the same manner to ensure blinding of both the participants, and the investigators involved in the data collection process. Both oils were colorless, similar in consistency and had no discernable scent.
Five drops, or 0.25 mls of 100% pure organic sesame seed oil or liquid paraffin oil were applied to the participants’ IV cannula site, from three centimeters above the insertion point to 10 cm along the vein, with a width of two centimeters on either side. The participants were instructed not to wash or wipe the topical agent off. At the start of the study, and at 12-h intervals, an investigator would observe for signs of phlebitis using the VIP scoring tool, before the application of the treatment or placebo. To minimize variation, all investigators were trained to apply the oils and assess IV cannula sites in the same manner. Oil applications and assessments for signs of phlebitis were conducted at IV cannula sites, at 12-h intervals for a maximum of 72 h.
IV cannulas were removed when no longer required for medical therapy, upon dislodgment, upon the end of the 72-h observation period, or at the first signs of the development of phlebitis. The VIP scoring tool was used to determine the severity of phlebitis according to the symptoms observed. Participants were also withdrawn from the study if they developed adverse reactions from the application of the topical sesame seed or liquid paraffin oil.
Results
A total of 263 participants were enrolled into the study. Of which, six participants withdrew before any intervention was carried out and the data of seven participants were later excluded from analysis, after they were found to possess medical conditions within the exclusion criteria (Figure 1). Out of the 250 participants that had their data analyzed, three participants developed itching after the application of liquid paraffin oil and thus had their interventions discontinued (Figure 1). No adverse effects were experienced by the participants with the application of sesame oil. The demographic and medical data of the participants are summarized in Table 1. There were no significant differences found between the two groups in the comparison of age, gender, ethnicity, position of IV cannula, size of IV cannula, and the location in which the IV cannula was inserted. CONSORT flow diagram. Mean, standard deviation and comparison of demographic variables.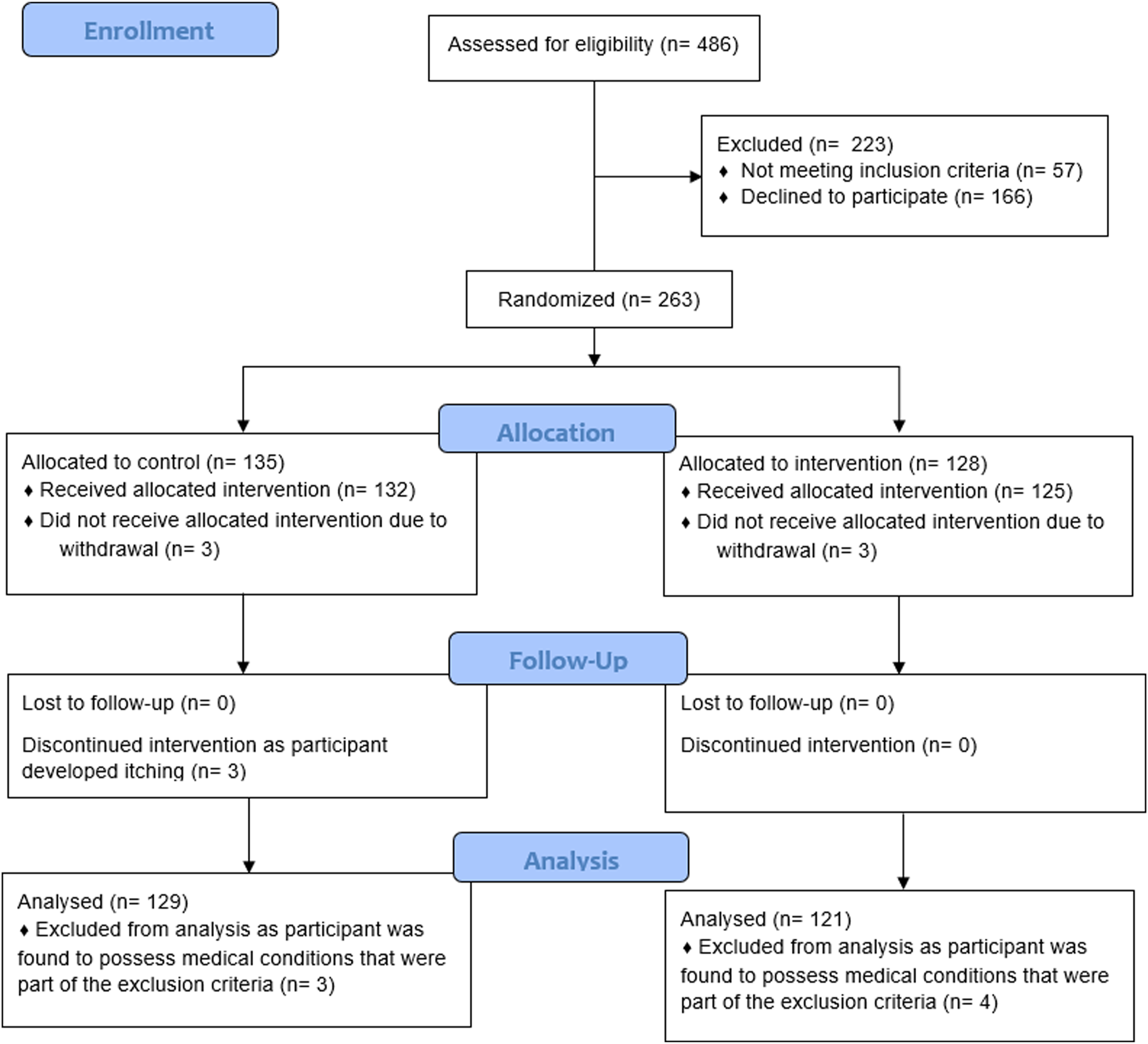

The age of the participants ranged from 33 to 80 with a mean of 64 and mean standard deviation (SD) of 10.3. Most of the participants were male (n = 174, 69.6%) and were of Chinese ethnicity (n = 172, 68.8%) (Table 1).
Comparison of phlebitis incidences using Pearson’s Chi-square test.

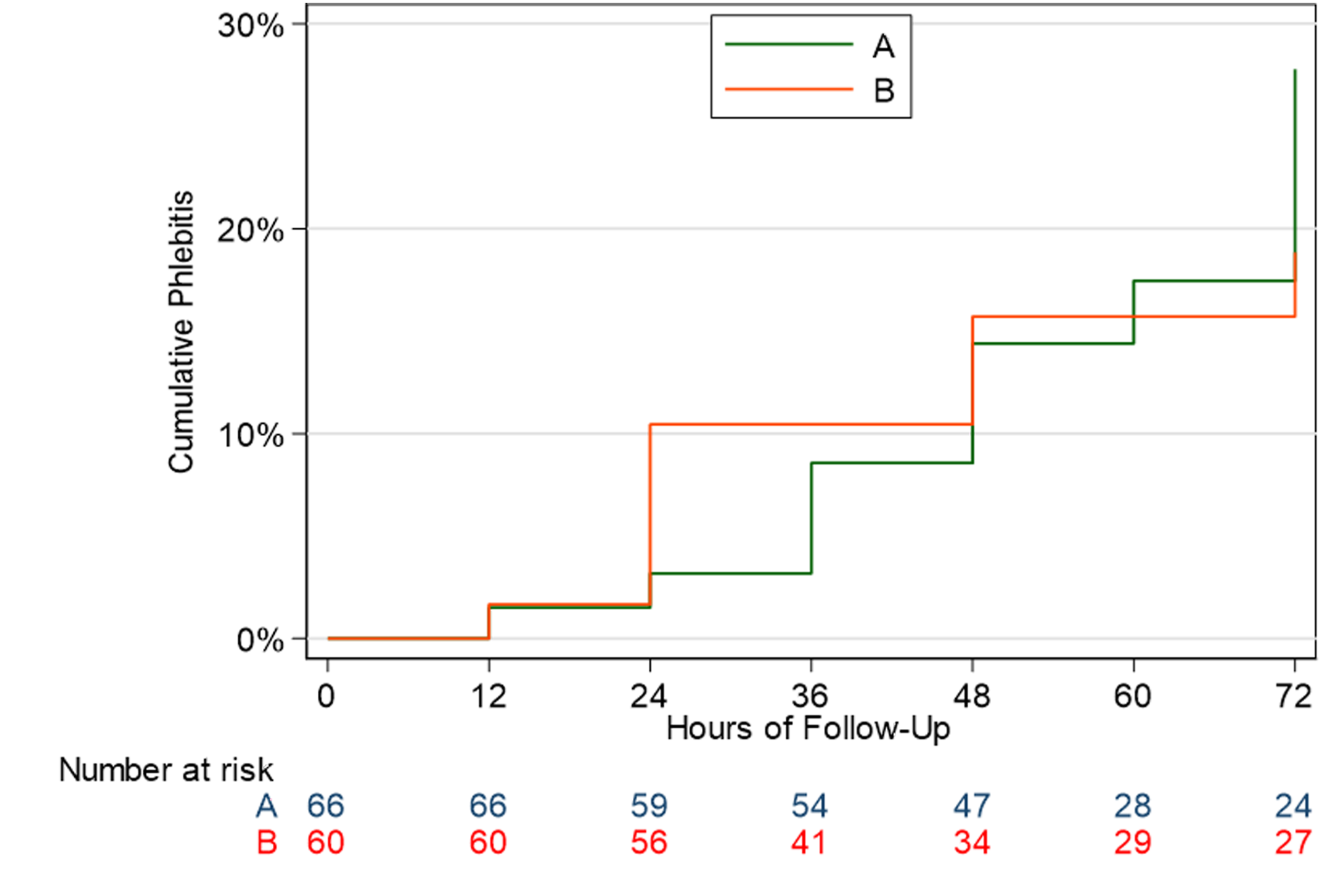
Using Kaplan-Meier survival analysis (Figure 2), we observed an increasing effect size after 36 h of intervention and obtained a hazard ratio of 0.56. However, there was no statistically significant difference (p = 0.128, 95% CI [0.27, 1.17]) between the cumulative incidences of phlebitis in both groups. Survival analysis of the cumulative incidences of phlebitis against time-intervals.
Correlation between cannula insertion site and phlebitis score using Fisher’s Exact test.

A subgroup-analysis of the male and female gender, and ages above 64 and 64 or younger was also performed. While no statistically significant association was found between the topical application of sesame oil and the development of phlebitis within each of the groups, a larger effect size was observed in females (Figure 3) compared to males (Figure 4), and in participants aged above 64 (Figure 5) compared to those 64 or younger (Figure 6). Survival analysis of the cumulative incidences of phlebitis against time-intervals in female participants. Survival analysis of the cumulative incidences of phlebitis against time-intervals in male participants. Survival analysis of the cumulative incidences of phlebitis against time-intervals in participants aged above 64. Survival analysis of the cumulative incidences of phlebitis against time-intervals in participants aged 64 and younger.


Phlebitis incidences by VIP score.

Discussion
In this study, 15.5% of the participants in the control group developed phlebitis compared to 9.1% of that in the treatment group. Though there was a higher incidence of phlebitis in participants who received liquid paraffin oil as compared to sesame oil, the difference was not found to be significant. This could be attributed to the relatively low incidence rate of phlebitis experienced in this study, as the sample population consisted of patients who possessed varying degrees of phlebitic risk within a cardiac inpatient ward. Previous studies obtained higher incidences of phlebitis by focusing only on patients with a high risk of developing chemical phlebitis, namely those receiving Amiodarone or chemotherapy.27,28,38 Unlike that of previous studies, the current study did not limit patient recruitment by medical therapy, hence giving the results more generalizability. However, we do recommend that future studies be conducted on a larger scale, to reduce the likelihood of the results being due to chance.
A hazard ratio of 0.56 was also obtained, which suggests that at any given time, a subject would be half as likely to experience phlebitis if topical sesame oil is applied to the IV cannula site as opposed to the placebo, liquid paraffin oil. These results support that of similar studies,27,28,38 where sesame oil was found to be effective at reducing the incidence of phlebitis.
It has been suggested in another study that the probability of developing phlebitis increases by 5% for every 24 h that the IV cannula remains inserted. 39 Despite this, we observed an increasing effect size with the use of sesame oil in the treatment group after 36 h, suggesting that sesame oil could be more effective when repeatedly applied over longer periods.
The cannula insertion site was found to be moderately associated with the development of phlebitis (p = 0.047). While the forearm (n = 11) and dorsum (n = 10) of the hand accounted for the highest absolute number of phlebitis cases, a closer examination reveals that the wrist site, despite recording only 5 cases of phlebitis, had a notably smaller number of cannulations (n = 20) compared to the other sites. This translates to a phlebitis incidence rate of 25% at the wrist, which is the highest among all insertion sites evaluated. Thus, this suggests that cannulas sited at the wrist may carry a relatively higher risk of phlebitis compared to other anatomical locations on the arm. Though this study did not delve into the exact reasons for this, it is supported by the results of a systematic review 40 which found that the development of phlebitis seemed to be influenced by the site of insertion, particularly at the joints. Cannulation at the wrist predisposes the development of thrombophlebitis due to it being a mobile joint. 40 It is postulated that the bending motion at joint areas with an IV cannula in place, traumatizes the vessel intima, thus resulting in inflammation, which then causes phlebitis.41–43 Hence, it is recommended that cannulations at the wrist be avoided, and splinted if a cannulation at this area is unavoidable. 40
Through this study we found a greater effect size in female participants compared to male participants, and in participants aged above 64 compared to those aged under 64. While some studies have shown a greater prevalence of IV cannula-related phlebitis in females,44,45 and amongst older patients,45,46 the reason that sesame oil seemed to be more effective at preventing phlebitis in these populations has not been studied in detail through this study. Future studies could consider exploring the possible reasons behind the association between gender, age, and the effectiveness of topical sesame oil in the prevention of phlebitis.
The absence of phlebitis scores above two in the treatment group suggests that the topical application of sesame oil at IV cannula sites may be effective at reducing the severity of phlebitis. This finding aligns with previous research 28 and may be attributed to the ability of sesame lignans in inhibiting inflammatory mediator and cytokine propagation, 34 and suppressing bacterial proliferation. 35 The excellent anti-bacterial and anti-inflammatory properties of sesame oil47,48 could make it useful in combating infective, chemical and mechanical phlebitis at IV cannula sites.
Limitations
This study was conducted on patients in a hospital specialized in treating cardiovascular disorders. As most patients that were recruited possessed cardiovascular disorders and were being treated with IV medications that were specific to their cardiac conditions, this might limit the generalizability of the results to other patient populations.
The incidence rate of phlebitis that was obtained in this study was also lower than that of similar studies. Previous studies evaluating the effects of sesame oil had been performed on patients who only received IV Amiodarone or Chemotherapy. This placed the participants at a greater risk of experiencing phlebitis. The current study, however, was conducted on the general population of patients in an inpatient cardiac ward, irrespective of the IV medications that were being prescribed and administered. A majority of patients recruited, therefore had a lower risk of developing phlebitis compared to the participants in other studies who received phlebitis-inducing IV medication like Amiodarone or chemotherapy. This could be the main reason for the observation of a lower incidence rate of phlebitis in this study.
Conclusion
The results of this study suggest that topical sesame oil could be an effective and safe method in preventing phlebitis and reducing the severity of phlebitis experienced at IV cannula sites, the lack of statistically significant results make it difficult to eliminate the possibility that these results could have been obtained by chance. Therefore, we recommend that larger studies be conducted in future, to better test this hypothesis.
Footnotes
Author note
This study was completed while the corresponding author Jia Xing Jasmine Tan was working at the National Heart Centre Singapore.
Acknowledgements
We would like to extend our heartfelt appreciation to everyone from the National Heart Centre of Singapore who had assisted us in seeing this study through to the end despite the many obstacles encountered – Ms Tay Ai Liu and Ms Kwek Koon Roan for supporting this study, Dr Fong Meng Kum and Dr Teo Lee Wah for providing research advice, Roslinda Binte Mohamed Idris, Liew Siok Moey, Low Huiling, Ong Xiang Yun Charmaine, Wee Shao Chun Venassa, Ng Jing Wei, Bte Syed Shiekh Sharifah Nur Dhabitah, Gowri N, Haziqah Bte Idris, Kang Yunfang, Lim Yok Yen and Tan Phaik Ting for assisting with data collection, Biostatistician Gao Fei for assisting with the analysis of data and all nurses of wards 44, 47 and 56 for helping out in one way or another.
ORCID iDs
Ethical considerations
Ethical approval was obtained from the Singhealth Centralized Institutional Review Board (CIRB) on the 24th of February 2022 (CIRB reference number 2021/2804).
Consent to participate
Written informed consent was obtained from all subjects before the study.
Author contributions
The lead author researched literature and conceived the study. All authors’ were involved in protocol development, gaining ethical approval, patient recruitment and data analysis. The lead author wrote the first draft of the manuscript. All other authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Lim Suh Fen Cardiovascular Research and Education Fund under the Cardiovascular Science Academic Clinical Programme of the National Heart Centre of Singapore [grant numbers 07/FY2021/EX/91-A145(a) & 07/FY2021/EX(SLP)/91-A145(b)]. The funder had no role in the design of the study, data collection, analysis and interpretation of the data, or in the writing of this manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All available datasets and analysis are available from the corresponding author.
Trial and protocol registration
NCT06216522.