
Abstract
Introduction
Contraception has a clear impact on the health of women and families in developing countries. This study aims to identify multilevel determinants of nonuse of modern contraceptives among Ethiopian rural married women in their productive age group.
Method
The study relied on data from the 2016 Ethiopian Demographic and Health Surveys. A multilevel logistic regression model was used for analysis.
Result
In rural areas, nonuse of modern contraceptives is surprising high (81.7%), primarily due to fear of side effects (12.89%) and breastfeeding (8.2%). Among women aged 35 to 49 years (adjusted odds ratio [AOR] = 0.66; 95% confidence interval [CI]: 0.540.81), husbands with secondary and above education levels (AOR = 0.83; 95% CI: 0.7–1), those in the high wealth index (AOR = 0.61; 95% CI: 0.51–0.72), and those who have had 1 to 2 children in the past 5 years (AOR = 0.28; 95% CI: 0.24–0.33), there was a lower chance of not using contraception. Muslims are less likely to want to use modern contraceptives (AOR = 1.2; 95% CI: 0.96–1.4). Women living in Afar (AOR = 20.9; 95% CI: 9.6–44.7), Oromia (AOR = 1.5; 95% CI: 1.01–2.3), Somali (AOR = 71.1; 95% CI: 24.1–209.2), Gambela (AOR = 2.3; 95% CI: 1.4–3.9), Harari (AOR = 4.4; 95% CI: 2.24–8.72), and Dire Dawa (AOR = 3.2; 95% CI: 1.5–6.9), regional states, were less likely to want to use modern contraceptives as compared to those in Tigray.
Conclusion
Family planning interventions should target younger women, women living in rural areas, the poor, and Muslim women. In order to maximize the effectiveness of family planning promotion policies, it's important to address the reasons for nonuse of contraceptives identified in each region and contextual differences regarding women of reproductive age.
Introduction
The utilization of modern contraceptives plays an important role in fertility control around the world. Contraception clearly impacts the health of women, children, and families in developing countries (Say et al., 2014). Modern contraception is used by 842 million women worldwide to avoid unintended and unwanted pregnancies. The global population reached 7.7 billion by mid-2019, up 1 billion since 2007 and 2 billion since 1994. Global population is expected to reach 8.5 billion in 2030, 9.7 billion in 2050, and 10.9 billion in 2100. In the coming decades, sub-Saharan Africa will account for the majority of global population growth, while many other regions will begin to see population decline. Between 2019 and 2050, the global population is expected to grow by nearly 2 billion people, with sub-Saharan African countries accounting for 1.05 billion (52%) of that growth (Ahinkorah et al., 2021).
Unplanned pregnancy accounts for 90% of abortions, with an annual rate of 87 million cases; and it is associated with higher rates of adverse maternal and infant health and socioeconomic outcomes in women who continue their pregnancy. As such, it is one of the most insistent public health issues in the world (Yazdkhasti et al., 2015). Increased access to effective contraception, on the other hand, could aid in the prevention of unplanned pregnancy and its negative effects on women's health and wellbeing, as well as the health and wellbeing of their families and communities (Behrman et al., 2018).
Many women, including married women, use induced abortion to deal with unintended pregnancies. Higher levels of unmet contraception need may contribute to higher rates of unintended pregnancies in developing countries (Mandiwa et al., 2018). In sub-Saharan Africa, for example, only 17% of women of reproductive age use contraception. Similarly, the use of modern contraceptives is a common healthcare challenge in Ethiopia. Despite an increase in women's use of modern contraceptives, challenges remain. Disparities in the use of modern contraception are common across the country. When compared to Addis Abeba (50.1%), Somali region has the lowest rate of modern contraceptive use (1.4%) (CSA, 2016; Fenta & Gebremichael, 2021).
Ethiopia, Africa's second most populous country, had an average of 4.6 children per woman in 2016 (CSA, 2016). Ethiopia is among the countries with the highest fertility rates in the world. The majority of demand-side factors investigated were women's education, age, household wealth, and parity. The significance of supply-side factors has largely gone unnoticed. According to some studies, supply-side factors have an impact on contraceptive use. For example, the quality of family planning (FP) services and living near a FP facility were found to be significantly related to modern contraceptive use (Shah, 2016).
In Ethiopia, modern contraceptives are freely available in all health facilities, and efforts are being made to increase their use. Contraception in Ethiopia has traditionally focused on short-acting methods such as birth control pills and injectables, which have a high risk of discontinuation (Melka et al., 2015a; Shah, 2016). Fears of side effects, health concerns, a lack of knowledge about women, a lower educational level, men's (partner's) objection, male partner desire for more children, and a lack of women's decision-making power are all barriers to contraceptive use, particularly in long-acting and permanent methods (Gebeyehu et al., 2018).
Between 1990 and 2014, the global rate of unintended pregnancy decreased, but less sharply in developing countries than in developed countries. Ethiopia is a developing country with a high rate of unintended pregnancy (Bearak et al., 2018). In Ethiopia, more than one-third (38%) of pregnancies were unintended in 2014, slightly lower than the 42% in 2008. According to the 2016 Ethiopian Demographic and Health Survey (EDHS), 25% of all births in the past 5 years and current pregnancies were unintended. Furthermore, the 2016 EDHS report revealed that the overall difference between the desired fertility rate and the total fertility rate is one child, implying that Ethiopian women are currently having one child more than they want (CSA, 2016).
Despite the existence of numerous individual studies on identifying factors of modern contraceptive utilization among women of reproductive age, there is no single study that includes all regions in Ethiopia in terms of the prevalence and associated factors on nonuse of modern FP among women of reproductive age, as well as the explanatory variables (the individual-level and community-level variables). Thus, the current study aimed to identify multilevel determinants of nonuse of modern contraceptives among rural married women in their productive age group in Ethiopia using data from the 2016 EDHS. As a result, this study will fill many gaps in the previous studies, helping planners and policymakers develop effective strategies to address the overwhelming complications of unintended pregnancy.
Review of the Literature
Approximately 85% of the world's population is younger than 25 years old, and most of them reside in low-income and middle-income countries (Mehra et al., 2012). Young people's sexual behavior has become a major issue in terms of public health, especially with regard to unintended pregnancies. The number of unintended pregnancies worldwide is estimated to be 41%, with 39% occurring in Africa (Singh et al., 2010). Sub-Saharan Africa has a 1:22 lifetime risk of maternal mortality, with adolescents facing higher mortality and morbidity risks than older women, according to World Health Organization (WHO, 2019).
Women who do not use contraceptive methods may suffer adverse health effects. An important contributor to unintended pregnancy is the nonuse of contraception (Dunn et al., 2019). A study of the reasons for women not using contraceptive methods in low-income and middle-income countries based on demographics and health surveys says that on average 40.9% of women in need of contraception did not use any contraceptive methods to avoid pregnancy. Overall, “health concerns” and “infrequent sex” were the most common reasons for nonuse of contraceptives, although their prevalence varied greatly between countries. There was a higher prevalence of nonuse due to “opposition from others” among married women than among unmarried women; nonuse due to “lack of access” or “lack of knowledge” was about two times higher in rural areas than in urban centers. Nonuse is more prevalent among women with less education due to “lack of access” (Moreira et al., 2019).
Nonuse of contraceptive methods by people who need contraception has been linked to potential consequences at the individual, familial, community, and global levels (Desa, 2016). As part of raising awareness of maternal and child health indicators have been developed (Brown et al., 2014). Furthermore, several agencies and organizations around the world have joined forces to finance FP initiatives, particularly in low-income and middle-income countries (Moreira et al., 2019).
The failure of women who require contraception to use contraceptive methods may have an impact on their lives and FP. Unintended pregnancy and its potential consequences are examples. Several reasons for nonuse of contraceptive methods have been identified through research. However, studies have mostly only focused on women who are married or who live with a partner. The population of this study consisted of all rural women in reproductive age. Researchers developed a multilevel model that accounts for extra heterogeneity in the data in order to identify factors contributing to nonuse of modern contraceptives among Ethiopian rural married women of productive age. As a result, this study aimed to examine multilevel determinants of nonuse of modern contraceptives among Ethiopian rural married women.
Materials and Methods
Design
A cross-sectional secondary dataset from the EDHS of 2016 was used in this study. The EDHS 2016 survey was organized to allow estimates of key indicators for the country as a whole, for urban and rural areas separately, and for each of the nine regions and the two administrative cities. Each region was stratified into urban and rural areas, yielding 21 sample strata. Samples of enumeration areas (EAs) were selected independently in two stages in each stratum. In the first stage, based on the 2007 population and housing census (PHC), an independent selection was implemented in each sampling stratum involving a total of 645 EAs (202 in urban and 443in rural) with probability proportional to EA size. In the second stage, a fixed number of 28 households per cluster were selected through an equal probability systematic selection from the newly created household listings (CSA, 2016).
Research Questions
Is the nonuse of modern contraceptives related to the age of women?
Is the nonuse of modern contraceptives related to the education level of women?
Is the nonuse of modern contraceptives related to economic status of women?
Does the state of the women's region influence their lack of use of modern contraception?
Inclusion/Exclusion Criteria
In this study, all women of reproductive age (15–49) who resided in rural parts of the country were included. Even so, women living in urban areas and women with incomplete data were not included in this study.
Source of Data
After receiving approval from the DHS program office for the 2016 EDHS, the fourth comprehensive survey in the series, we obtained the dataset for this study from the MEASURE DHS database, accessible at http://dhsprogram.com/data/.
Study Variables
Dependent variable
The dependent variable was current nonuse of modern contraception among women of reproductive age. Women were classified as “1 = nonusers” if they did not use any modern contraceptive method or used folkloric and traditional methods, and “users = 0” if they used any modern contraceptive method.
Independent Variables
Previous research and the variable's availability in the 2016 EDHS dataset were used to determine the independent variables for nonuse of modern contraceptive methods. Variables were divided into two categories: individual-level and community-level variables associated for a multilevel logistic approach.
Individual-Level Variables
Age of women at the time of survey, husband age, educational level of women, educational level of husband, woman's occupation, wealth index, husband's occupation, religion, healthcare delivery, accessing healthcare, desire for more children, births in the past 5 years, hearing of FP messages through radio, watched FP on TV for the past few months, and read FP in newspaper/magazine for the past few months were included as individual-level variables.
Community-Level Variables
Regions were regarded as community-level variables obtained directly from EDHS.
Data Management and Analysis
SPSS software version 23 was used to extract and decode data, and STATA version 14 was used to analyze the decoded data. To describe the study respondents, descriptive statistics such as frequencies and percentages were used. A multilevel study design does not consider individual observations to be independent of one another. The women in this study were nested with EAs. The standard regression model is inapplicable in this situation. As a result, a multilevel logistic regression model was used to identify the associated predictors of nonuse of modern contraceptives among sexually active women in Ethiopia.
Four consecutive models were fitted in the multilevel analysis (Katz, 2011; Sciences et al., 2020). The first was the null model (Model I), which is fitted without any explanatory variable at the individual and community levels to detect the existence of a possible contextual effect. The second model fit by incorporating all individual-level data variables (Model II). This step evaluated the contribution of each individual-level explanatory variable, the significance of each predictor, and the changes in the first-level and second-level variance terms. The third model was created by incorporating all community-level variables (Model III). This model allows us to examine whether the explanatory variables at the community level explain the between-group variation in the dependent variable.
Multilevel Logistic Regression Analysis
The 2016 EDHS data is hierarchical in its structure and women are nested within EAs (communities). Hence, considering the hierarchical nature of the data, multilevel logistic regression models were applied to identify factors associated with women not using modern contraceptives (Hriţcu, 2015). The log of the probability of women unemployment was modeled using a two-level multilevel model as follows:


Result
Sample Characteristics
The proportion of rural married women who were not using modern contraceptives was 6116 (81.7%) due to concern about fear of side effects/health concerns (12.89%), breastfeeding (8.2%), and followed by fatalistic (7.1%) and postpartum (5.5%) (Table 1).
Reason for Not Using Modern Contraceptive Among Rural Married Women in Ethiopia, 2016 EDHS.
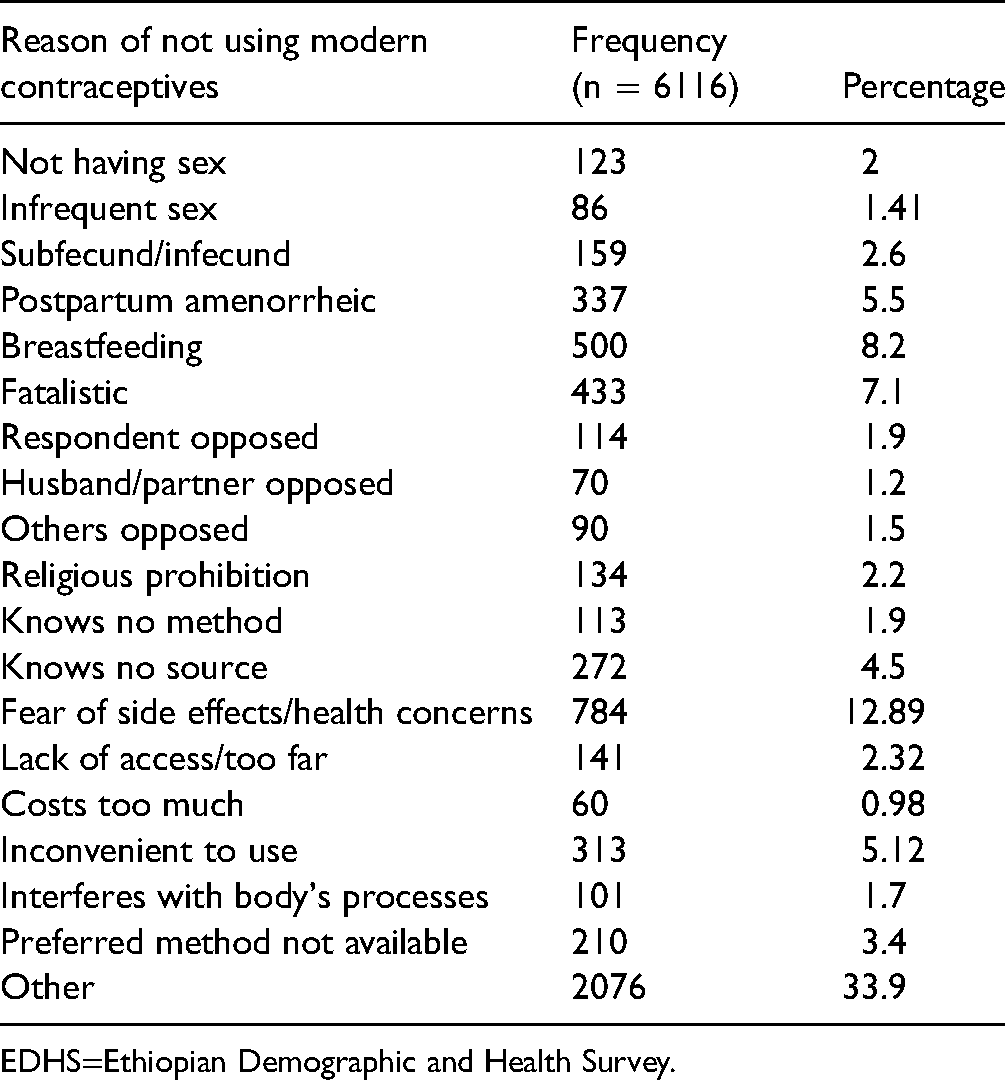
EDHS=Ethiopian Demographic and Health Survey.
Socioeconomic, Demographic, Maternal, and Obstetric Characteristic of Rural Married Women in Ethiopia
Women characteristic's dissemination based on demographic factors, parity, and wealth index can be seen in Table 2. Table 2 showed that most of the rural married women were 15 to 24 years (39.06%) and majority resided in Oromia (16.23%) region followed by Southern Nations, Nationalities, and People Region (SNNPR) (15.27%) region. More than half of the respondents had no education (59.17%). The employment status of respondents was not much different, 50.31% who work and 49.69% who do not work. According to economic status, 51.30% were classified as poor, while 32.3% were classified as wealthy. Though 39.54% of rural married women followed Christianity, 4729 (63.19%) are delivered at a health institution. Among rural married women, 5328 (71.2%) had no serious healthcare access problems and the majority gave birth to one to two children (50.52%).
Socioeconomic, Demographic, Maternal, and Obstetric Characteristic of Rural Married Women in Ethiopia, 2016 EDHS.

EDHS=Ethiopian Demographic and Health Survey; SNNPR=Southern Nations, Nationalities, and People Region.
After 2 years, 31.69% rural married desired additional children, whereas 35.68% wanted no more children. In rural areas, almost one in four rural married women (22.8%) reported hearing about FP on TV and radio during the past few months. Less than 10% of women (4.78%) have been exposed to FP in newspapers or magazines in the past few months (Table 2).
Research Questions Results
The results of the multilevel binary logistic regression model both individual-level and community-level variables were summarized in Table 3. The model comparison result revealed that model III was a better fit for the data as compared to other reduced models, since it had the smallest AIC, BIC, and DIC statistics. In this model all individual-level and community-level factors were included. Wealth index, education level of husband, age of women, religion, women births in the past 5 years, and region were factors significantly associated with nonuse of modern contraceptive method among rural married women (Table 3).
Result of Multilevel Logistic Regression for Predictors of Nonuse of Modern Contraceptive Use Among Rural Married Women in Ethiopia, 2016 EDHS.

*Significant at P value < .05.
**Significant at P value <.01.
***Significant at P value <.001.
AOR=adjusted odds ratio; CI=confidence intervals; EDHS=Ethiopian Demographic and Health Survey; SNNPR=Southern Nations, Nationalities, and People Region.
Individual-Level Factors
Women aged 25to 34 and 35 to 49 years were 0.67 (adjusted OR [AOR] = 0.67; 95% CI: 0.56–0.81) and 0.66 (AOR = 0.66; 95%CI: 0.54–0.81) times less likely to not use modern contraceptives compared to 15 to 24 years old, respectively. Husband attending the secondary and above educational level was 0.83 (AOR = 0.83; 95% CI: 0.7–1) times less likely to not use modern contraceptive method compared to not attending any formal education. Rural marriage women, in the middle wealth index status were 0.7 (AOR = 0.7; 95% CI: 0.56–0.83) times less likely to not use modern contraceptives than those women with poor wealth index status. Similarly, women with a rich wealth index were 0.61 (AOR = 0.61; 95% CI: 0.51–0.72) times less likely to not use modern contraceptives than women with a poor wealth index. The likelihood of being willing to use modern contraceptives among Muslim women was 1.2 (AOR = 1.2; 95% CI: 0.96–1.4) times less likely than that for Christian women. The odds of not using a modern contraceptive method among women who had one to two children in the past 5 years (AOR = 0.28; 95% CI: 0.24–0.33) were lower when compared to women who had no births in the past 5 years (Table 3).
Community-Level Factors
Women living in Afar (AOR = 20.9; 95% CI: 9.6–44.7), Oromia (AOR = 1.5 ; 95% CI: 1.01–2.3), Somali (AOR = 71.1; 95% CI: 24.1–209.2), Gambela (AOR = 2.3; 95% CI: 1.4–3.9), Harari (AOR = 4.4; 95% CI: 2.24–8.72), and Dire Dawa (AOR = 3.2; 95% CI: 1.5–6.9) regional states were more likely to not use modern contraceptives as compared to women living in Tigray region. However, women living in Amhara (AOR = 0.6; 95% CI: 0.4–0.8) were less likely to not use modern contraceptives as compared to women living in Tigray region (Table 3).
Random Effect Measures of Variation
The results of random effects indicated that there was a statistically significant variation in the use of modern contraceptives across the clusters (Table 4). In other words, the use of modern contraceptives was not similarly distributed across the clusters. The ICCs revealed that 32.76% of the variation in the not using modern contraceptives could be attributed to community-level factors. After adjusting for individual-level and community-level factors, there is a significant variation in the not using modern contraceptives among rural marriage women across communities or clusters. About 54.5% do not use modern contraceptives in clusters was explained in the full model. Moreover, the MOR confirmed that nonuse of modern contraceptives was attributed to community-level factors. The MOR for not using modern contraceptives was 3.42 in the null model, which indicates variation across communities. The unexplained community variation in the nonuse of modern contraceptives was reduced to MOR of 2.3 when all individual-level and community-level factors were added to the model. This indicated that when all factors are considered, the effects of clustering are still statistically significant in the full models (Table 4).
Measure of Variation on Individual-Level and Community-Level Factors Associated With Not Using Modern Contraceptive Among Rural Married Women in Ethiopia, 2016 EDHS.

AIC=Akaike's information criterion; BIC= Bayesian's information criterion; DIC=deviance information criterion; EDHS=Ethiopian Demographic and Health Survey; ICC=intra-cluster correlation coefficient; MOR=median odds ratio; PCV=proportional change in variance; SE=standard error; LL=log likelihood ratio.
Discussion
The nonuse of modern contraceptive methods among rural married women in Ethiopia was 81.7%, due to concern about fear of side effects/health concerns (12.89%), breastfeeding (8.2%), fatalistic (7.1%), and postpartum (5.5%).
Multilevel multivariable analysis showed that there were significant variables related to the nonuse of modern contraceptive method. Furthermore, for women of young age (15–24), their use of FP decreased. The women's age had a significant impact on their refusal to use modern contraceptive methods. This finding was in line with the findings of a Nepal (Adhikari et al., 2019), Nigeria (Asaolu et al., 2019; Ejembi et al., 2015), and Malawi (Mandiwa et al., 2018) study, which discovered that as women's ages increase, so does their likelihood of using modern contraception. Studies conducted in East Africa (Tessema et al., 2021), China (Wang, 2012), and Ethiopia (Gebeyehu et al., 2018; Mandiwa et al., 2018; Melka et al., 2015b; Mulugeta et al., 2022) found results that differed from the present study. The low contraceptive prevalence among women aged 15 to 24 years is most likely due to the fact that the majority of these women engage in unsafe sex, are newly married, and marriage is based on the institution of producing children. Access to modern FP services is likely to be difficult for a young mother. Another possible explanation is that the former group included women who had either finished childbearing or wanted to space their children, as opposed to the latter group, which included women who had not yet begun childbearing. Additional possible reason could be that youths were less likely to use FP services because of societal beliefs that they should not have premarital sex.
An increasing husband's educational level made women more likely to use modern contraception. This suggests that husband's education most likely has a positive effect on nonuse of modern contraceptives among women. It confirms previous study results (Mulugeta et al., 2022). There is a significant association between women's wealth status and nonuse of modern contraceptive method. Household wealth index negatively affects nonuse of modern contraceptive among rural marriage women in the current study. Because modern contraceptives are free in Ethiopia, the contribution of household wealth to contraceptive use is not explained by the ability to pay for the service. Relatively, it reflects the household's overall socioeconomic status (Abate & Tareke, 2019), which has a significant impact on health (Tessema et al., 2021). In developing countries, economic status has been shown to increase not only contraceptive use but also other maternal health services (Ahmed et al., 2010; Tessema et al., 2021). It may be due to the fact that women from rich families might be more educated and have careers that enable them to pursue their business agendas longer. Moreover, in our community, most rich women had one or two children throughout their lifetime, and this indicates that they are more likely to utilize modern contraceptive methods (Hounton et al., 2015; Muhoza Ndaruhuye, 2014; Wang et al., 2013).
Religion, according to the study's findings, was strongly associated with women's nonuse of modern contraception. Muslim women were more likely to not use contraception compared Christian women. This finding is consistent with the findings of Alomair et al., (2020). This is because, in Muslim societies, sexual and reproductive health issues are rarely discussed and are considered sensitive subjects. The majority of findings show that there are multiple levels of factors that influence Muslim women's sexual and reproductive health. Poor sexual and reproductive health knowledge and practices among Muslim women are a complex issue influenced by personal, community, cultural, and religious factors, as well as existing policies and regulations. There is a critical need for interventions that address modifiable barriers to sexual and reproductive health education and services in order to improve knowledge, informed choice, and access to services, thereby facilitating better sexual and reproductive wellbeing for Muslim women. It is important to note that, we recognize that significant differences exist within every culture and religion (Fenta & Gebremichael, 2021; Towriss & Timæus, 2018).
Women who had given birth in the past 5 years were less likely to use modern contraception than women who had not given birth. This result is in agreement with other previous studies (Adhikari et al., 2019; Fenta & Gebremichael, 2021; Tessema et al., 2018). There may be a link between nulliparous women's desire to have a child and their less likely use of contraception, because most nulliparous women have no desired childbearing capacity (Behrman et al., 2018; Tessema et al., 2021).
Moreover, the nonuse of modern contraception methods varied by region. Women in Afar, Somali, Gambela, Harari, and Dire Dawa were less likely to use modern contraception methods than women in Tigray, but Amhara region had a lower rate of nonuse. Contraceptive methods are inaccessible, resulting in Ethiopia's highest under-five mortality rate (Fenta & Gebremichael, 2021; Sciences et al., 2020; Tegegne et al., 2020).This implies that having access to contraceptive methods will reduce child and infant mortality and add to the health complications of mothers. The possible reason for this regional disparity is that there are differences in the implementation of FP services across regions.
Strengths and Limitations
This analysis may have some limitations despite being based on a nationally representative, large-scale dataset like EDHS. During the survey, participants were asked to recall events from the past 5 years, and some details may have been forgotten. As a result, causal relationships between exposure variables and outcomes cannot be identified due to the cross-sectional nature of the data. Due to the fact that these estimates are taken from a nationally representative sample, they may change over time as a result of these limitations. Despite this, the Centers for Disease Control and Prevention used a global framework to develop and deploy EDHS, which is a nationally representative dataset. In spite of these limitations, the results can still be generalized throughout the country. International comparisons are also possible due to the use of similar instruments across countries.
Implications for Practice
The health of women's sexual and reproductive systems can be adversely affected if they do not use contraceptive methods. Women with no use of modern contraceptives were extremely prevalent in this study. Fear of side effects/health concerns and breastfeeding were the most common reasons for not using modern contraceptives. In order to prevent unwanted pregnancy and sexually transmitted infections, it is necessary to listen to women's beliefs and opinions, provide women with more information about the importance of using contraceptives, inform them of the contraceptive methods available and their side effects, and provide them with greater access to contraceptives.
Conclusion
In the current study, the magnitude of nonuse of modern contraceptive utilization among rural currently married women in Ethiopia was unexpectedly high (81.7%). The most common reasons of nonuse of modern contraceptives were fear of side effects/health concerns and breastfeeding. Both individual-level and community-level factors can influence nonuse of modern contraception. Among individual-level factors, aged women, educated husbands, and women who had at least one birth in the past 5 years, were negatively associated with nonuse of modern contraceptives, but poor women and Muslim women were positively associated with nonuse of contraceptives. In Ethiopia, community-level factor, region was significantly associated with nonuse of modern contraceptives. This finding suggested that the government and other stakeholders must provide educational opportunities, raise awareness about the use of modern contraceptives, and provide valuable counseling services to those women who may be avoiding modern contraceptives.
Footnotes
Abbreviations
Acknowledgments
We would like to thank the Ministry of Health and Central Statistical Agency, Government of Ethiopia, for making the data freely available for research purposes.
Availability of Data and Materials
Authors’ Contributions
SSM carried out the data extraction, performed the data analysis and interpretation, and drafted the manuscript. MWM, ATB, MMY, and SBA performed the data analysis and interpretation, and drafted the manuscript, and also conducted the writing and revision of the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
A secondary dataset from the EDHS was used in the study, which was approved by the Ethiopian National Ethics Committee and the Institutional Review Board of ICF. A data request was approved by the DHS program and the data were accessed and used in accordance with the data agreement. Individual identifying information is not contained in the publicly available data.