
Abstract
Introduction
Contraceptive switching from a more effective to a less effective method is a concern, especially in developing countries with high unmet needs for family planning. Indeed, the lack of understanding regarding the reasons behind contraceptive switching behavior in the study area poses a significant challenge in effectively addressing this issue.
Objective
This study aimed to assess the magnitude and factors associated with long-acting contraceptive switching in Mizan-Aman town, southwest Ethiopia.
Methods
A community-based cross-sectional study was conducted, involving 345 women randomly selected from the population of married women in their reproductive age group. Data collection was conducted through interviewer-administered questionnaires. Bivariate and multivariable logistic regression analyses were employed to ascertain factors linked with contraceptive method switching status. Statistical significance was determined at a P-value of less than .05.
Results
Out of the 345 participants interviewed, the prevalence of switching from long-acting to short-acting contraceptives was 28.4%, 95% CI (13.6%, 33.2%). Upon adjusting for confounding variables, factors significantly associated with contraceptive switching included women aged 31–35 [adjusted odds ratio (AOR) = 0.58; 95% CI (0.36, 0.74)] and aged 41–49 [AOR = 0.54; 95% CI (0.48, 0.82)], those with formal education [AOR = 0.79; 95% CI (0.52, 0.87)], those desiring future pregnancy [AOR = 2.12; 95% CI (1.98, 3.38)], experiencing complications from previous method use [AOR = 3.67; 95% CI (2.57, 7.40)], and encountering stockouts of their preferred contraceptive choice [AOR = 2.01; 95% CI (1.39, 3.24)].
Conclusion and recommendation
The study area exhibited a notable prevalence of switching from long-acting contraceptives. Complications arising from prior method use and the unavailability of preferred contraceptive options emerged as significant factors influencing this switching behavior. Thus, it underscores the importance of providing counseling and ongoing support to women, ensuring access to safer and more effective modern contraceptive methods.
Introduction
Family planning is defined as “the ability of individuals and couples to anticipate and achieve their desired number of children, as well as the spacing and timing of their births” (Alemayehu Gonie et al., 2018). It plays a crucial role in addressing reproductive health challenges, such as preventing unplanned and mistimed pregnancies, which are vital for achieving Sustainable Development Goals 3.7 (ensuring universal access to sexual and reproductive health services, including family planning) and 3.1 (reducing maternal mortality by preventing unwanted pregnancies and ensuring women's access to contraception) (United Nations, Department of Economic and Social Affairs, 2019; World Health Organization, 2018).
Family planning has been shown to reduce maternal and child mortality rates by 32% and 10%, respectively (Mutowo et al., 2014; Tilahun et al., 2014). However, the uptake of modern contraceptives among women varies globally (United Nations, Department of Economic and Social Affairs, 2015). While Northern America reports the highest utilization at 75%, sub-Saharan Africa exhibits the lowest at 33% (United Nations, Department of Economic and Social Affairs, 2015). Despite the high efficiency of Long-Acting Reversible Contraceptives (LARCs), their utilization remains limited in many countries (Ferreira et al., 2014).
Unplanned pregnancies are most prevalent in sub-Saharan Africa (Sedgh et al., 2014). Reports indicate that approximately 24% of women in sub-Saharan African countries have never utilized any modern contraception method despite their desire to postpone or avoid pregnancy (United Nations, Department of Economic and Social Affairs, 2015). In Ethiopia, contraceptive usage was only at 41.4% in 2019 (Ethiopian Public Health Institute and ICF, 2019), which contributes to the high incidence of unintended pregnancies, estimated at 30% in the country (Bekele & Fekadu, 2021).
Research from 36 countries indicates that approximately 30% of unintended recent births were due to contraceptive discontinuation (Jain & Winfrey, 2017), highlighting the importance of increasing contraceptive use among Ethiopian women. Factors such as education, marital status, women's age, income level, number of children, lack of knowledge about modern contraception, attitudes, social support, and the availability and accessibility of modern contraceptives have been identified as key factors influencing modern contraception utilization (Bekele et al., 2021; Debebe et al., 2017; Geremew & Gelagay, 2018). Perceptions of contraceptive side effects, ease of use, and cost are strongly associated with rational patterns of contraceptive method switching (Yuli Amran et al., 2019).
Literature Review
The most effective reversible contraceptive methods include intrauterine devices and contraceptive implants, commonly referred to as LARCs (The Committee on Practice Bulletins—Gynecology and the Long-Acting Reversible Contraception Work Group, 2017). Adolescents opting for LARC tend to report higher efficacy, continuation rates, and satisfaction levels compared to those using short-acting contraceptives (The American College of Obstetricians and Gynecologists’ Committee, 2018). Factors such as the user's educational level significantly influence the success of short-acting contraceptives (Leevan Tibaijuka et al., 2017), suggesting that in resource-limited settings where educational levels may be low among women seeking contraception, short-acting methods may be less effective (Alemayehu & Wondifraw, 2014). Promoting awareness of LARC methods is crucial as their effectiveness often hinges on user awareness (Caetano et al., 2020).
The challenge of contraceptive switching from more effective to less effective methods has become pronounced, particularly in developing countries like Ethiopia, contributing to high rates of unintended pregnancies (Bekele et al., 2015). Studies have found that women who discontinue contraception often switch to less effective methods (Abou Coulibaly et al., 2020). Predictors of method switching include women's age, educational status, income level, and parity (Alia et al., 2014). In Ethiopia, research indicates that 35% of women discontinue their contraceptive methods, with 6% switching to another method (Central Statistical Agency and ICF, 2016). Additionally, studies conducted in Jimma, southwest Ethiopia, reported a contraceptive switching rate of 9.6% (Yideta et al., 2017). Furthermore, contraceptive switching rates were reported at 27.6% in Dilla (Kelborea et al., 2020), 40% in Dire Dawa (Atnafe et al., 2016), and 30.2% in Hadya (Bereku et al., 2022) studies conducted in Ethiopia.
While previous studies conducted in health facilities (Atnafe et al., 2016; Bereku et al., 2022; Kelborea et al., 2020) have touched on the subject, they have not adequately captured the full extent of contraceptive method switching among women. Health facility studies often focus on women who have already discontinued a method and sought a new one at a clinic. This misses women who switch methods without going to a healthcare provider, potentially underestimating the true prevalence of switching. This study aims to fill that gap by focusing on assessing this issue within the community. Furthermore, prior research has often encompassed women of reproductive age regardless of marital status (Bereku et al., 2022; Tesfa & Gedamu, 2018; Yideta et al., 2017). However, married women are consistently the primary users of modern contraceptives (United Nations, Department of Economic and Social Affairs, 2015) and have been shown to be significant predictors of contraceptive method switching (Kelborea et al., 2020). To our knowledge, no previous research has specifically assessed the prevalence and factors associated with long-acting contraceptive switching among married women only. Therefore, the aim of this study is to investigate the prevalence and determinants of long-acting contraceptive switching among married women in southwest Ethiopia.
Methods
Study Design
A community-based cross-sectional study was conducted.
Study Settings
The study was conducted in Mizan-Aman town, which serves as the administrative center of the Bench-Sheko zone in southwest Ethiopia. Positioned 585 km southwest of Addis Ababa, Mizan-Aman comprises five kebeles and has a population of approximately 52,210 individuals, with 18,625 males and 33,585 females. The town is supported by five public health facilities, including two health posts, two health centers, and one teaching hospital, alongside numerous private clinics. Most of these facilities offer modern family planning services. The study was conducted between October 10 and November 15, 2019.
Populations
The source population included all married women of reproductive age, while the study population comprised randomly selected married women within this age range. Eligible participants were married women aged 18 years and above, residing in selected households within the study area for at least six months. Exclusions were made for individuals unable to communicate due to severe illness or unwillingness to participate.
Sampling Design
The required sample size was calculated using the single population proportion formula, considering the previous study's findings of long-acting contraception switching at 30.2% in the Hadya zone, southern Ethiopia (Bereku et al., 2022), with a 95% confidence level and a 5% margin of error:

Data Collection Tools, Procedures, and Quality Control
Data collection was conducted using an interviewer-administered questionnaire, adapted, and modified from the Ethiopian Demographic and Health Survey (Central Statistical Agency and ICF, 2016). The questionnaire encompassed sociodemographic characteristics (such as age, ethnicity, education, marital status, occupation, monthly income, residence, and religion) as well as obstetric characteristics (including childbirth history, number of live children, desire for children within 2 years, and discussions with a partner about fertility desires). Initially drafted in English, the questionnaire was translated into Amharic and then back into English to ensure consistency. Face validity was evaluated by a reproductive health expert, and reliability was confirmed with a robust Cronbach's alpha coefficient (0.88). A pretest on 5% of the sample size was conducted in Bonga town prior to data collection, and comprehensive training was provided to data collectors and supervisors to ensure uniformity and clarity in administering the questionnaire.
Study Variables
The study's dependent variable was contraceptive method switching, defined as transitioning from more effective LARCs (specifically, intrauterine contraceptive devices [IUCDs] and implants) to less effective short-acting contraceptives (including Depo-Provera injections and oral contraceptive pills). Independent variables included sociodemographic factors (age, education, occupation, religion, ethnicity, monthly income, residence, and marital status) and obstetric characteristics (childbirth history, number of live children, desire for children within 2 years, and discussion with a partner about fertility desires).
Statistical Analysis
The data were entered into EPI data version 4.2.0.1 and analyzed using SPSS version 23. Results were summarized and presented in mean, standard deviation, frequency, percentage, tables, and figures. Bivariate and multivariable logistic regression analyses were conducted to identify factors associated with contraceptive method switching. Variables with P value < .25 in bivariate analysis were included in multivariable logistic regression. Multicollinearity was assessed using the variance inflation factor (VIF < 2), with correlations between independent variables deemed tolerable. The Hosmer-Lemeshow test confirmed the model's goodness of fitness. Results were interpreted using crude and adjusted odds ratios (AORs), along with their corresponding 95% confidence intervals. Statistical significance was set at P value < .05.
Results
Sociodemographic Characteristics
In the study, 345 women participated, resulting in a response rate of 97%. The mean age of the participants was 32 ± 6.7 years. Nearly half of the respondents identified as Bench ethnicity (52.2%) and Protestant by religion (48.7%). Moreover, more than half (53.3%) of the respondents were housewives (Table 1).
Sociodemographic Characteristics of the Study Participants (n = 345).

Obstetric Characteristics
Nearly all participants (97.9%) had experienced childbirth, with an average of 2.7 ± 1.7 live births per woman. The mean desired number of children stood at 1.7 ± 0.7, ranging from 1 to 12 children. Furthermore, over half of the participants (54.5%) expressed no desire to have a child within the next two years (Table 2).
Obstetric Histories of the Study Participants (n = 345).

Magnitude of Contraceptive Switching
Among the 345 participants surveyed, 28.4% (95% CI: 13.6%–33.2%) switched from long-acting to short-acting contraceptives. Among the 98 participants who made this switch, the highest rate (53.1%) was observed from implant to Depo-Provera, followed by implant to pills (28.6%) and IUCD to Depo-Provera (10.2%) (Figure 1).
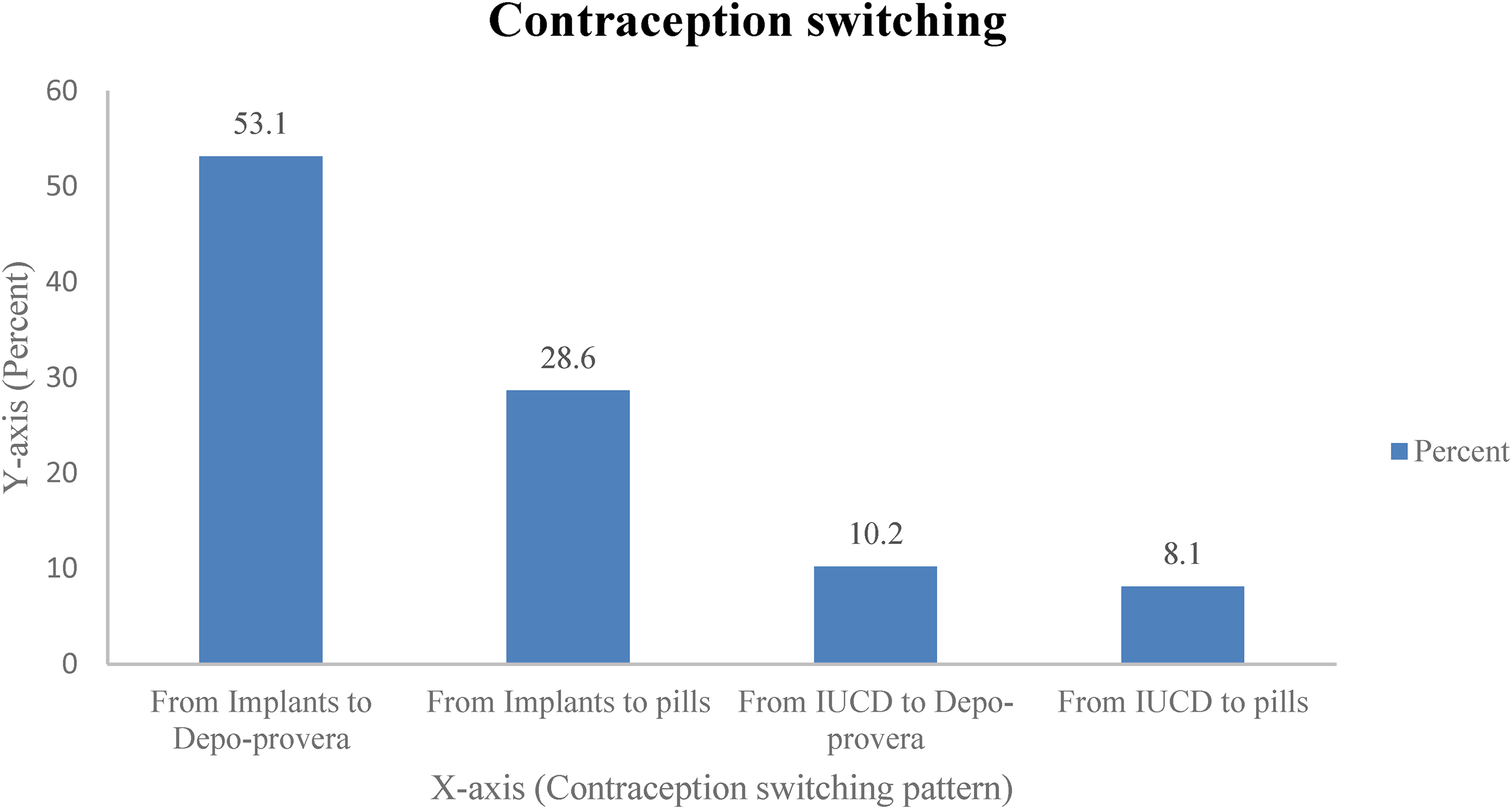
Switching from long-acting contraceptive to short-acting contraceptive among the study participants (n = 98).
Factors Associated with Contraceptive Switching
In bivariate analyses, factors such as age group, education, desire for future pregnancy, method availability, and past complications were linked to method switching. After adjusting for confounding variables, women aged 31–35 [AOR = 0.58; 95% CI (0.36, 0.74)] and 41–49 [AOR = 0.54; 95% CI (0.48, 0.82)], those with formal education [AOR = 0.79; 95% CI (0.52, 0.87)], expressing a desire for future pregnancy [AOR = 2.12; 95% CI (1.98, 3.38)], experiencing complications from previous method use [AOR = 3.67; 95% CI (2.57, 7.40)], and encountering contraceptive stockouts [AOR = 2.01; 95% CI (1.39, 3.24)] remained significantly associated with contraceptive switching (Table 3).
Factors Associated with Contraceptive Switching among Study Participants (n = 345).

Note. AOR = adjusted odds ratio; CI = confidence interval; COR = crude odds ratio; Ref = Reference; *P value < .25, **P value < .05.
Discussion
This study aimed to evaluate the prevalence and determinants of long-acting contraceptive method switching among married women in southwest Ethiopia. The prevalence of contraceptive switching was 28.4%, 95% CI (13.6%, 33.2%). This figure aligns with rates reported in Dilla, Ethiopia (27.6%) (Kelborea et al., 2020) and Nigeria (13.8%) (Awoyesuku et al., 2021), but surpasses rates observed in Jimma, Ethiopia (9.6%) (Yideta et al., 2017) and the US (19%) (Darney et al., 2023). Nonetheless, it falls below rates documented in Dire Dawa, Ethiopia (40.4%) (Atnafe et al., 2016) and the US (31.7%) (Simmons et al., 2019). The disparities could stem from differences in methodology and study demographics. Despite all studies involving women in their reproductive age group, discrepancies, such as including a health institutions participants (Atnafe et al., 2016) and using a 6-month (Simmons et al., 2019) and 4-year follow-up time (Darney et al., 2023) for prevalence measure, contribute to inconsistencies in the findings. Like our study, Yideta et al. (2017) used a 12-month prevalence measure, but because participants were more educated, the prevalence of switching found to be lower than our finding. This hints at a possible link between education and contraceptive switching behavior, with the significant variance in switching rates possibly tied to the participants’ high literacy rate. The elevated prevalence of contraceptive method switching in this study raises concerns about reproductive health risks such as unwanted pregnancies and abortions linked to less effective short-acting contraceptives. Therefore, it is crucial to counsel women about the option of transitioning to more effective long-acting modern methods. Due to issues such as menstruation problems, side effect concerns, and health considerations, the IUD showed a high discontinuation and switching rate. Women considering this method should undergo thorough counseling regarding expected outcomes and potential side effects associated with its use (Barden-O'Fallon et al., 2018).
Age was statistically linked with contraceptive switching. Women aged 31–40 years and 41–49 years were 42% and 46% less likely, respectively, to switch contraceptive methods compared to those aged less than 20. This finding is consistent with prior research (Amran et al., 2019; Mahumud et al., 2015), indicating that older women may have decreased desires for children, resulting in a reduced likelihood of switching methods.
The educational status of women significantly influenced contraceptive switching. Those with formal education were 21% less likely to switch contraceptive methods compared to those without formal education. While this aligns with a study in Bangladesh (Mahumud et al., 2015), indicating uneducated women are more likely to switch, it contradicts findings from other studies (Alia et al., 2014; Barden-O'Fallon et al., 2018), suggesting more educated women are more prone to switching.
This study revealed a significant association between women's desire for children and contraceptive switching. This finding aligns with studies conducted in Ethiopia (Atnafe et al., 2016; Bereku et al., 2022), indicating that women without a desire for children were less likely to switch contraceptive methods compared to those desiring children. This suggests that women aiming to have children in the future may be more inclined to switch contraceptive methods.
This study found a significant association between previous method complications and contraceptive switching. Women who experienced side effects from their previous method were 3.7 times more likely to switch contraceptives. This suggests that women may switch methods due to side effects, complications, or medical indications specific to their condition. Similar findings have been reported in other studies (Atnafe et al., 2016; Bereku et al., 2022; Mrwebi et al., 2018), where complications such as bleeding, weight loss, and arm numbness were cited as reasons for switching methods (Atnafe et al., 2016). Additionally, method-specific side effects were identified as the primary reasons for contraceptive discontinuation and switching (Bereku et al., 2022). Therefore, it is crucial to assess women's overall health and monitor side effects to minimize the risk of unintended pregnancies and related issues stemming from method switching and discontinuation.
The stockout of preferred contraceptive choices was significantly linked to contraceptive switching. Women whose preferred contraceptive was unavailable were twice as likely to switch methods compared to those with available options. This finding underscores the impact of stockouts on women's contraceptive decisions, as they may opt for alternative methods readily available in health facilities. Muhoza et al. (2021) also supported this, indicating that stockouts and limited method availability constrain contraceptive choice, leading individuals to select methods that may not align with their preferences and needs. Thus, it is imperative for health facilities to ensure immediate availability of contraceptive choices by collaborating with government agencies and local nongovernmental organizations.
Strengths and Limitations
The strengths of this study include its community-based approach and the representativeness of the sample selection strategy. However, limitations arise from the cross-sectional nature of the study, which precludes establishing causality. Additionally, recall bias may have been introduced, potentially impacting the accuracy of the observed switching patterns.
Implications for Practice
The shift from long-acting to short-acting contraceptives presents a significant public health concern. Practice nurses are well-positioned to play a crucial role in counseling clients and providing them with their preferred contraceptive options. It is vital to educate women about all available forms of contraception and ensure they have access to qualified nurses who can address their inquiries effectively.
Conclusions and Recommendation
The study revealed a high prevalence of switching from long-acting contraceptives in the study area, indicating that contraceptive switching is a public health concern. Complications arising from previous method use and contraceptive choice stockouts were identified as significant modifiable factors associated with switching. Therefore, it is crucial to provide counseling and follow-up to women to ensure they have access to better and safer modern contraceptive methods.
Footnotes
Acknowledgments
The authors acknowledge the study participants for their valuable participation and the Bench-Sheko Zone health department bureau for their full collaboration and support by providing important data during the study. The authors would like to acknowledge data collectors and supervisors for their valuable contributions during data collection.
Authors Contributions
MT: Conceptualization; methodology; investigation; data curation; resources; funding acquisition; writing – original draft; writing – review and editing. AD and NS: Methodology; investigation; formal analysis; project administration; supervision. TY: Conceptualization; methodology; software; validation; investigation; data curation; formal analysis; writing – original draft; writing – review and editing. All authors read and approved the final manuscript.
Availability of Data and Materials
The datasets used during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Ethical approval was obtained from Mizan-Tepi University Ethical Review Committee (MTU-ERC) before data collection. An official letter of cooperation was obtained from the zonal health bureau. Participants were informed of the study's objectives, their right to refuse participation, and the confidentiality of their information. Written informed consent was obtained from all participants.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix
STROBE Statement—Checklist of items that should be included in reports of cross-sectional studies.