
Abstract
Background
COVID-19 pandemic has a high impact on the health of pregnant women and healthcare providers worldwide.
Objective
This study aims to assess midwives’ knowledge and preparedness in providing maternity care during COVID-19 pandemic.
Methods
A cross-sectional analytical hospital-based study that included 116 midwives, who were working in labor ward, was conducted in the Dodoma region of Tanzania from March to June 2021. The Chi-square test and Fisher's exact test were used to assess the association between the categorical variables. The predictors of midwives’ knowledge and preparedness were determined using binary logistic regression analysis. Statistical analysis was performed using SPSS version 23.0; p < .05 was considered to be significant.
Results
Of the midwives studied, 63 (54.3%) had adequate knowledge about COVID-19 and only 30 (25.9%) were adequately prepared on provision of maternal care. Having diploma/bachelor level of education (AOR = 2.62, 95%CI = 1.08–6.36, p = .033), being trained on COVID-19 (AOR = 3.65, 95%CI = 1.11–12.00, p = .033) and working in urban health facilities (AOR = 3.65, 95%CI = 1.17–13.98, p = .002) were the significant determinants of midwives’ knowledge on COVID-19. Working at a health center (AOR = 0.19, 95%CI = 0.03–1.32. p = .033), being trained on COVID-19 (AOR = 0.04, 95%CI = 0.01–0.14, p = .000 and having adequate knowledge on COVID-19 (AOR = 0.20, 95%CI = 0.03–1.32, p = .032) were determinants of midwives’ preparedness on provision of maternal care.
Conclusion
Knowledge and preparedness in the provision of maternity care during the COVID-19 pandemic were low. Emphasis should be put on training midwives on IPC when providing maternity care. This may help in preventing the spread of infectious diseases including COVID-19 as we observed in the present study.
Introduction
The COVID-19 pandemic is caused by a severe acute respiratory syndrome coronavirus (SARS-CoV-2), which was first reported in Wuhan, China, in December 2019 (Liu et al., 2020). Recently, the virus has rapidly spread throughout the world. Evidence has shown that the coronavirus disease outbreak is a respiratory tract infection caused by SARS-CoV-2 (Hossain et al., 2020; Li et al., 2020). COVID-19 pandemic disease is transmitted in two main ways: direct transmission through close contact with a person infected and indirect transmission which is through contact with contaminated surfaces (Grimaud et al., 2020).
Midwives play a significant role in ensuring safe childbirth and quality care provision for women, girls, and families (Pallangyo et al., 2020). Because of the increased risk of SARS-CoV-2 infection in pregnant women, maternal care is of paramount importance. Midwives’ knowledge and preparedness in providing maternal care have been reported elsewhere to be higher. For example, in studies done in Ethiopia and Pakistan, the level of knowledge among midwives was 88% and 85%, respectively (Shi et al., 2020b; Wuneh et al., 2021). Despite the high level of knowledge of health care providers reported in the literature, there is limited local data on midwives’ knowledge as well as preparedness for the provision of maternal care during the COVID-19 pandemic.
One study by Breslin et al. showed that pregnant mothers are more vulnerable to SARS-CoV-2 than nonpregnant women (Breslin et al., 2020). Similarly, other studies have reported that pregnant women are at increased risk and severity of COVID-19 as well as complications compared to nonpregnant women (CDC, 2021; DeBolt et al., 2021; Metz et al., 2021; Villar et al., 2021). This has been explained due to reason that pregnant women have an increased risk of acquiring the infection due to physiological immune suppression which occurs during pregnancy (Qeadan et al., 2021; Rebutini et al., 2021).
After the outbreak of COVID-19 in different parts of Tanzania in which the Dodoma region is included, the provision of maternal services was negatively affected. Midwives had no prior training regarding the pandemic. Additionally, they were not prepared for providing optimal maternal care due to fear of contracting the infection and transmitting the infection to family members and others. Nurse–midwives were worried about contracting the infection like any other person as well. On the other hand, pregnant women also had worries about contracting COVID-19. As a result, they decided to have home delivery. Therefore, all these shortcomings compromised greatly the provision of maternal care in the region (Personal communication).
Therefore, the current study aims to assess the midwives’ knowledge and preparedness in providing maternity care during COVID-19 pandemic in Dodoma Region, Tanzania. In addition, we determined the predictors of both knowledge and preparedness for the provision of maternal care during the COVID-19 pandemic.
Methods and Materials
Study Area and Design
This is a multicenter, cross-sectional study that involved five health facilities in Dodoma region, Tanzania between February and March 2021. Despite there are many health facilities that provide maternal and child health in Tanzania, we selected the five health facilities conveniently. The selected health facilities included three district hospitals, one regional referral hospital, and one health center. Dodoma is one of the 30 regions in Tanzania and is located in the center of the country. The Tanzania Population and Housing Census of August 2012 reported that the region had a total population of 2,328,949 people of whom 1,134,496 were males and 1,194,453 were females. The census also reported that women of reproductive age were 526,542 (URT, 2013). The fertility rate in Dodoma region was 4.9 persons per woman in 2013 (National Bureau of Statistics, 2016). Dodoma region was selected for this study because it has been experiencing a rapid increase in population. However, there was a challenge in the documentation of the incidence of COVID-19 among pregnant women in the region and country as large.
The Study Population
The study involved midwives practicing in labor wards from the selected health facilities. The inclusion criteria included all midwives who agreed to participate in the study and were ready to sign a written informed consent. We excluded all midwives who refused to provide consent.
Sample Size Determination
We calculated the sample size using the Kish Leslie formula for quantitative studies as it was used in our previous study (Alphonce Joho, 2021). n = Z² p(1-p)/ e², where n = minimum required sample size, z = confidence level at 95% (standard value of 1.96), and p = proportion of the estimated level of knowledge, and marginal error of 0.05. We assumed the proportion to be 7.6% as was reported in the previous study which was done in Nepal regarding the perceived level of knowledge on COVID-19 among frontline healthcare workers (Tamang et al., 2020). We obtained a sample size of 104. Additionally, to accommodate nonresponses, we considered an attrition rate of 20% to obtain the required sample size was 125.
Sampling Method
Conveniently, we selected five health facilities which included three district hospitals, one regional referral hospital, and one health center. These health facilities were selected because of the high number of deliveries. Census sampling was used to obtain the eligible midwives to be included in the present study. This method was used because the population was deemed to be small. All midwives working in labor wards in the selected health facilities were screened for eligibility and consecutively included in the study until the required sample size was obtained.
Data Collection Tool
Data collection was done by the principal investigator and the coinvestigator. The process of data collection involved a face-to-face approach. Data were collected from the labor ward of the respective health facility, in which a screen was used for privacy purposes. Approximately, it took 25–30 min for each participant to complete filling out the questionnaire. A self-administered questionnaire that we used had two components: knowledge and preparedness.
The 27 items for assessing knowledge were adopted and modified from a previous study by Id et al. (2020). On the other hand, 13 items for assessing preparedness were designed by the investigators and pretested for validity by analyzing their internal consistency using Cronbach's alpha coefficient (Taber, 2018). We performed pretesting of the questionnaire among 30 nurse–midwives students from a site other than the selected health facilities. Acceptance for validation was based on Cronbach's alpha value of ≥0.7 (Taber, 2018). In this study, we found Cronbach's alpha of 0.714 and 0.672 in measuring the internal consistency reliability for knowledge and preparedness, respectively.
The questionnaire contained closed-ended questions, which were divided into three parts: Demographic characteristics, knowledge of COVID-19, and midwives’ preparedness. The sociodemographic characteristics included sex, age, education level, qualification, years of work experience, and marital status. The questionnaire had 26 questions regarding midwives’ knowledge of COVID-19; six questions related to the model of transmission, eight questions on safety precautions, six questions on signs and symptoms, and six questions related to complications.
We used questionnaire that contained 13 questions for collecting data regarding midwives preparedness for providing maternal care during the period of COVID-19. The questionnaire contained information regarding training on COVID-19, availability of separate labor room for women who were suspected to have COVID-19, availability of guidelines, availability of personal protective equipment (PPE) and oxygen, adequacy of PPE, room for changing clothes before and after provision of care, the process of referral, supervision, and ANC services during COVID-19.
Measurement of Knowledge and Preparedness
Midwives’ knowledge was measured using 27 questions and each response was scored “1” (correct) and “0” (wrong), with total scores ranging from 1 to 27. A cutoff level of <80% was considered to be inadequate knowledge about COVID-19, whereas ≥80% was considered adequate knowledge about COVID-19 as was reported in the previous studies (Asemahagn, 2020; Ellen et al., 2021; Olum et al., 2020). Component principle analysis (PCA) was performed to reduce weak items for knowledge and preparedness questions. The Kaiser–Meyer–Olkin (KMO) measure of sampling Adequacy of 0.705, p-value .000, Bartlett's test of sphericity 1120.547, and total variance explained by the model was factor number 9 with cumulative initial Eigenvalue of 65.535. Initial Eigenvalue involved 27 items, of which none of them weighted <0.3. Therefore, all of the 27 were retained for further analysis.
Midwives’ preparedness was measured using 13 questions. Each question was given a score of 1 for adequately prepared and 0 for inadequate preparedness. Participants with a total percentage score of at least 77 and above were considered to be adequately prepared for COVID-19. For preparedness, the KMO measure of sampling adequacy of 0.642, p-value .000, Bartlett's test of sphericity 263.976, and total variance explained by the model was factor number 4 with a cumulative initial Eigenvalue of 58.774. Initial Eigenvalue involved 13 items, of which none of them weighted <0.3. Therefore, all of them were retained for further analysis.
Data Analysis
Data analysis was performed using the STATA version 15.0. The predictors of knowledge and preparedness for the provision of maternal care during the first surge of COVID-19 were determined by using binary logistic regression. A two-sided p-value <.05 was considered to be statistically significant.
Results
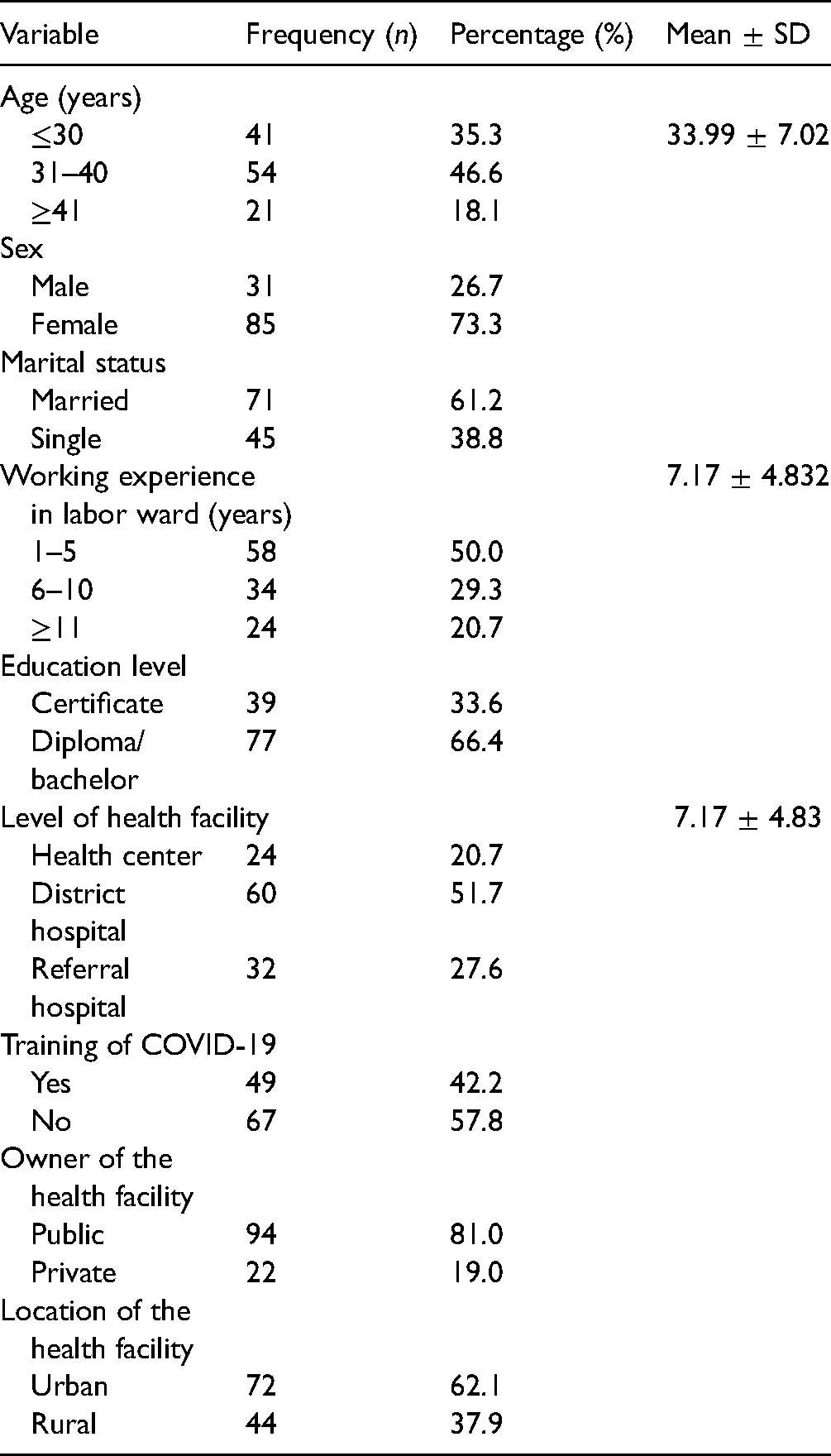
In this study, a total of 125 midwives were approached of whom 116 agreed to participate in the study with a response rate of 93%. Most 54 (46.6%) of the midwives were aged between 30 and 40 years with a mean age of 33.99 ± 7.02 years. The majority 85 (73.3%) of participants were females. Over half 68 (58.6%) of the participants had attained a diploma level of education. Concerning working experience in the obstetric ward, 58 (50%) had 1–5 years. Regarding training on COVID-19, the majority 67 (57.8%) did not attend any training (Table 1).
Sociodemographic Characteristics of the Study Participants (N = 116).
Knowledge of the Midwives on COVID-19
Overall, the mean knowledge score was 12.53 ± 2.66. Over half (54.3%) of midwives had an adequate general knowledge of COVID-19. Also, 49 (42.2%) of them responded correctly that, COVID-19 may be transmitted through droplets when an infected person coughs, sneezes, or speaks. Regarding signs and symptoms of COVID-19, slightly over half of 59 (50.9%) of the participants responded correctly that, difficulty in breathing is a common sign of COVID-19. Surprisingly, only 22 (19.0%) of the participants responded correctly that body weakness is a common symptom of COVID-19. Furthermore, the majority of 98 (84.5%) of the midwives responded correctly that, physical social distancing among workers is a preventive measure of COVID-19. However, only 30 (25.9%) of them were knowledgeable that, self-isolation (extended leave) for sick staff is a preventive measure for COVID-19. Regarding complications of COVID-19, only 26 (22.4%) of the participants responded correctly that, acute respiratory distress is a complication of COVID-19 (Table 2).
Summary of the Frequency of the Midwives Who Responded Correctly to the Items Used to Measure Knowledge During the First Surge of COVID-19.

SPO2 = Oxygen saturation.
Midwives’ Preparedness in the Provision of Maternal Care During the First Surge of COVID-19 Pandemic
Only 30 (25.9%) midwives had adequate preparedness with a mean score of 6.03 ± 1.28. Over one-third 49 (42.2%) midwives received training on caring for patients with COVID-19. Out of them, only 24 (20.7%) had received training on caring for pregnant women suspected to have COVID-19. The majority of 82 (70.7%) of the midwives had the standard operating procedures (SOPs) for managing pregnant women with respiratory distress. Only 16 (13.8%) midwives had enough personnel preventive gears for protection against COVID-19. All midwives (100%) who were included in the current study responded that they did not have a separate room for caring for pregnant mothers who were suspected or confirmed with COVID-19 in their health facilities (Table 3).
Summary of Positive Indicators Regarding Midwives’ Preparedness on the Provision of Maternal Care During the First Surge of COVID-19.
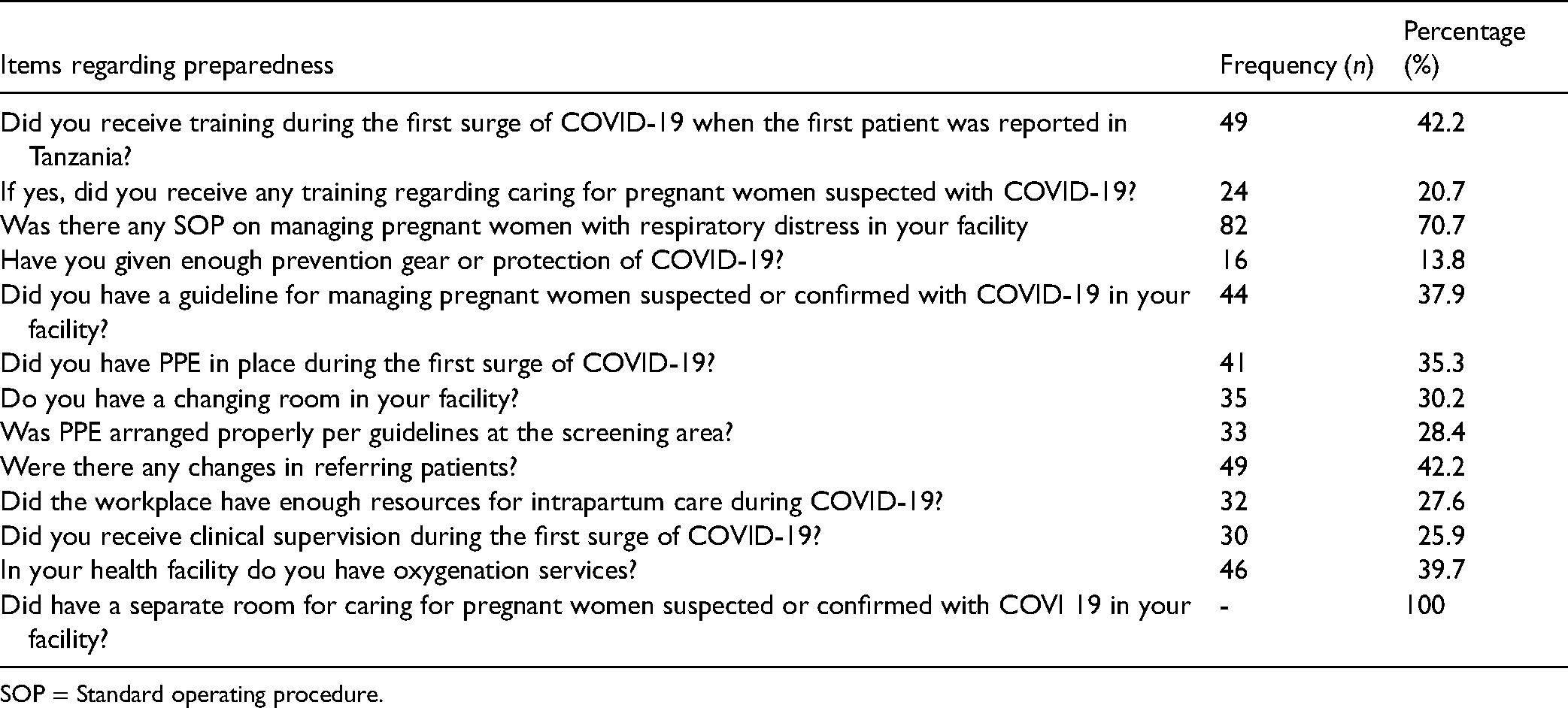
SOP = Standard operating procedure.
Factors Associated with Knowledge of COVID-19 Among Midwives
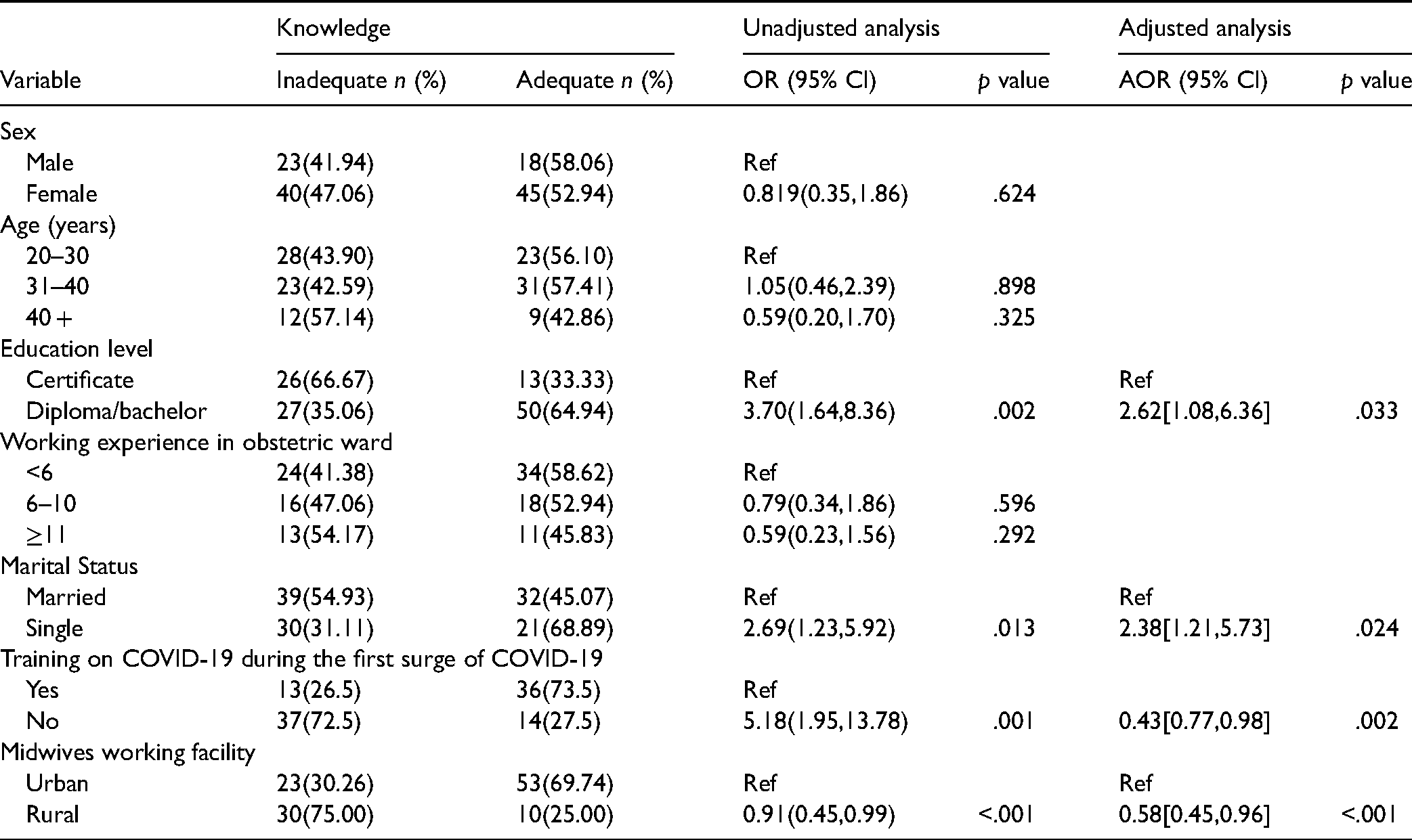
Midwives with a diploma and/or bachelor's education level were almost 3 times more likely to have adequate knowledge of COVID-19 compared to midwives with a certificate level of education (OR = 2.6, 95%CI = 1.08–6.36, p = .033). Midwives who did not attend training during COVID-19 had 57% less chance of having adequate knowledge compared to midwives who attended training (AOR = 0.43, 95%CI = 0.77–0.98, p = .002). Midwives who work at rural health facilities, had 42% less chance of having adequate knowledge (AOR = 0.58, 95%CI = 0.45–0.96, p = .001) (Table 4).
Factors Associated with Knowledge of COVID-19 Among Midwives.
Factors Associated with Midwives’ Preparedness for Provision of Maternal Care During the First Surge of COVID-19
Midwives who were working at health centers had 81% less chance of having adequate preparedness for the provision of maternal care during the first surge of COVID-19 compared to the midwives who were working at referral hospitals (AOR = 0.19, 95% CI = 0.03–1.32, p = .033). Also, midwives who were working at district hospitals had 64% less chance of having adequate preparedness for the provision of maternal care compared to midwives who were working at referral hospitals however the difference was not significant (AOR = 0.36, 95% CI = 0.09–1.52, p = .099). Regarding training of the midwives on COVID-19 during the first surge, we observed that midwives who were not trained had 96% less chance of being likely to have adequate preparedness (AOR = 0.04, 95% CI = 0.01–0.14, p = .000). Midwives who had inadequate knowledge had 80% less chance of having adequate preparedness (AOR = 0.20, 95%CI = 0.03–1.32, p = .032). Other details can be found in Table 5.
Factors Associated with Midwives’ Preparedness on Provision of Maternal Care During First Surge of COVID-19 (N = 116).

Discussion
The current study presents midwives’ knowledge and preparedness in the provision of maternal care during the COVID-19 pandemic in Dodoma region, Tanzania. COVID-19 pandemic has caused a significant change in the provision of care for pregnant women at the time of childbirth locally and globally (Davis-Floyd et al., 2020; Jardine et al., 2021; Silverio et al., 2021).
In this study, 54.4% of the midwives had adequate knowledge during the first surge of COVID-19. Surprisingly, this level of knowledge in the present study was significantly lower than 89.5%, 88%, 85, and 70% of the level of knowledge among health care providers including midwives that were reported (Kasahun et al., 2020) in China, Northern Ethiopia, Pakistan, and the Amhara region in Ethiopia, respectively (Asemahagn, 2020; Izhar et al., 2021; Shi et al., 2020a; Wuneh et al., 2021).
There are several reasons for this difference in the level of knowledge across studies. A small percentage (42.2%) of our participants had received training during the first surge of COVID-19, compared to more than half of participants in Ethiopia who received relevant training on IPC (Asemahagn, 2020). Being trained for IPC might have given more exposure, knowledge, and experience to health care providers in Ethiopia. In countries where there was a lack of political will to address issues related to COVID-19 in public, this had a great impact on knowledge, attitude, and even practice (Hatcher, 2020). In addition, it has been shown that high incidences of confirmed cases of COVID-19 have a positive impact on increasing the level of knowledge and awareness (Lin et al., 2020).
Regarding factors associated with knowledge of COVID-19 among midwives on the provision of maternal care in this study, not attending any training on COVID-19 during the first surge had 57% less chance of having adequate knowledge. Similarly, a finding was reported by Asemahagn in the study conducted in the Amhara region, Ethiopia in which it was found that health workers who attended training on IPC were 2.4 more likely to have adequate knowledge of COVID-19 (Asemahagn, 2020). These findings noticeably indicate the significance of improving health care provider COVID-19 knowledge via health education, which may also result in enhancements in their attitudes and practices toward COVID-19. This has been demonstrated in many other studies among health workers (Shi et al., 2020a).
Emphasis has been reported on the importance of training for frontline health workers and the community at large in the prevention of communicable diseases (Miguel-Puga et al., 2021; Otu et al., 2021). It is crucial to empower healthcare workers with the required knowledge and skills for understanding and practicing evidence-based medicine. Provision of training on COVID-19 is important in raising awareness and level of knowledge in particular for developing countries in which Tanzania is included, in which acceptance and uptake rate of available vaccines is substantially at a low rate (MacPherson, 2020). Parallel to training, the health systems should play an important role in providing enough PPE and IPC resources to frontline midwives so that they can provide quality care to patients without worries of contracting the disease.
Having a diploma or bachelor's degree in our study had a positive association with having adequate knowledge related to COVID-19. A similar finding was reported in the study of Bhagavathula et al., who reported that the level of professionalism was associated with an adequate level of knowledge of COVID-19 (Bhagavathula et al., 2020). Furthermore, Gambhir et al. reported that there was an association between level of education and knowledge of COVID-19 among health care providers, p = .018 (MacPherson, 2020).
Midwives’ preparedness for the provision of maternal care during the first surge of COVID-19 in this study was very low. Only 25.9% of midwives were found to be adequately prepared for the provision of maternal care during the first surge of COVID-19. The level of preparedness in the current study was significantly lower compared to 41.4%, and 57.5% of the level of preparedness reported by Chanie and Nkansah in Northwest Ethiopia and Ghana, respectively (Chanie et al., 2021). The reason for low level of preparedness among midwives in this study may be contributed to inadequate training on how to respond to infectious diseases including COVID-19.
Factors that determined the level of knowledge seem to be similar to that determined preparedness among health workers. Political will has been reported to have an impact on both knowledge, practice, awareness, and preparedness, and even the community when it comes to COVID-19 globally. For example, in the countries that have positive political will toward COVID-19 pandemic, studies have shown that both levels of knowledge and preparedness are higher than in areas where there is negative political will (Guest et al., 2020).
Midwives are the frontline health care providers in dealing with the lives of women during pregnancy, at the time of delivery, and after delivery. They are vulnerable to contracting SARS-CoV-2 when providing care and fighting against infectious diseases. Previous studies have reported that health care workers including midwives are at high risk and vulnerable to acquiring COVID-19 (Heinzerling et al., 2020; Khunti et al., 2021; Smith, 2020), and need preparedness is paramount important (Vos et al., 2017).
In this study, we observed that not attending any training during the first surge of COVID-19 had a 96% less chance of having adequate preparedness. This observation was strongly supported by the similar observation in other studies done everywhere (Elhadi et al., 2020; Grabowski & Joynt Maddox, 2020; Kasahun et al., 2020). For example, a study conducted in Libya reported that 54.7% of nurses who received training on the effective use of PPE had adequate preparation (Elhadi et al., 2020). The difference observed in the percentage of nurses and/or midwives preparedness may be contributed by lower public announcement of the incidence of COVID-19. In Tanzania, during the first surge, there was a challenge in the public announcement of incidences of COVID-19. Various studies have emphasized the importance of training for emergency preparedness (D et al., 2021; Grabowski & Joynt Maddox, 2020).
In the current study midwives’ knowledge of COVID-19 was significantly associated with preparedness. Midwives who did not have adequate knowledge of COVID-19 had 80% less chance of having adequate preparedness. A similar finding was reported by Suleiman et al. in the study conducted in Jordan that knowledge of COVID-19 was correlated with preparedness (Suleiman et al., 2020). Another study conducted in Libya reported that inadequate knowledge is a risk factor for transmitting the infection and poor preparation (Elhadi et al., 2020).
Regarding guidelines for the management of pregnant women in labor during the period of COVID-19, in the current study most of the participants 62.1% had no guidelines. Working without guidelines or having guidelines from multiple organizations may bring challenges in the provision of care to midwives and it may cause increase the risk of acquiring and transmitting COVID-19 in the health setting and also increase the risk of maternal morbidity and mortality. This has been supported by Pavlidis et al. in a study conducted in Australia, who reported that different clinical guidelines created by different organizations create challenges for clinicians who provide maternal care during labor and deliveries (Pavlidis et al., 2020). Having different guidelines may create confusion because of differences in direction in provision of care. Fore stance some guidelines directed that when a woman had a spontaneous vaginal delivery and in short of breath, suggested to shorten the time of second stage of labor by performing instrumental delivery (Favre et al., 2020; Vrachnis et al., 2019). Meanwhile, others suggested the model of delivery be a cesarean section (Api et al., 2020). Regarding delayed cord clamping, various guidelines have no consensus on whether delayed cord clamping is best for neonates in women with COVID-19. Such as studies done by Api et al. and Favre et al. (Api et al., 2020; Favre et al., 2020) suggested that delayed cord clamping should be avoided in newborns to mothers with COVID-19, the reason that the SARS-CoV-2 has been identified in the placenta and membranes (Api et al., 2020). But other guidelines suggested that delayed cord clamping should be continued for the safety of the newborn (Baud et al., 2020; He et al., 2022). All these discrepancies in recommendations of maternal care during COVID-19 and others bring confusion to health care providers. However, clinical guidelines save lives (Pavlidis et al., 2020). Having clinical guidelines or protocols is mandatory for the safety of the women and their newborns and that of health care providers themselves. On the other hand, when women come to the health facility on time and midwives don’t provide the required care because of a lack of guidelines, then this is the cause of a third delay in the provision of care (Knight et al., 2013).
In the current study, we found that only 30.17% of health care facilities had space for staff to put on and remove minimum PPE before entering and exiting the labor room. This is likely due to limitations of space, gaps in knowledge, and the absence of guidelines and training. Our findings are mirrored by research in India where staff shortages and limited spacing required a need to optimize resources and establish local protocols for the prevention of the spread of COVID-19 (Sharma et al., 2020). For use of PPE, recent research focuses on the proper use of PPE, donning and doffing PPE, and performing hand washing or hygiene after removal of PPE (Agarwal et al., 2021; Bampoe et al., 2020).
In the current study, we investigated the presence of a separate labor room for COVID-19-infected mothers. Our finding showed that there is no health facility with a separate labor room for mothers with suspected or confirmed COVID-19 infections. To prevent the spread of COVID-19 infection among pregnant women with suspected or confirmed COVID-19, facilities should have separate rooms for their labor, delivery, and postpartum care to prevent the spread of COVID-19. A similar study done by Davis-Floyd et al. (2020) supported noninfected pregnant women to give birth in a separate labor ward and should give birth in the selected rooms for safety, efficacy, and reducing the chance of contracting the disease.
Strength of the Study
To the best of our knowledge, this is the first study in Tanzania in examining midwives’ knowledge and preparedness in providing maternity care during COVID-19 pandemic. Our findings add to the available evidence from other studies regarding midwives’ knowledge and preparedness in the provision of care to mothers with labor pain during the COVID-19 pandemic.
Limitations of the Study/Potential Sources of Bias
Self-reporting of midwives’ preparedness might have introduced recall bias by either over-reporting or underreporting depending on the person's behavior in the recent past information which might have caused information bias. Convenience sampling for selecting health facilities might have caused selection bias. The current study had a small sample size which may affect the power of the study.
Conclusion
Knowledge and preparedness in the provision of maternity care during the COVID-19 pandemic were low. Emphasis should be put on training midwives on IPC when providing maternity care. This may help in preventing the spread of infectious diseases including COVID-19 as we observed in the present study.
Recommendations
Protecting health workers and clients should be of paramount importance to our health system. This can be accomplished through regular in-service training focused on caring for patients with COVID-19, provision of and correct use of PPE, and ensuring proper running water and alcohol-based hand gel for proper hand hygiene. Guidelines on caring for pregnant women with COVID-19 during antenatal, delivery, and postnatal should be provided and implemented to ensure quality care and to prevent the spread of infection to others. Health facilities administrators should ensure that PPE supplies are readily available for frontline health workers, including midwives. With support from facility leadership, health workers should implement the use of minimum PPE and create a place for donning and doffing additional PPE when attending birth to prevent contacting and spreading of infection. All pregnant women presenting for care should be screened for symptoms of COVID-19 and have timely access to effective testing and treatment for COVID-19. Pregnant people who confirmed COVID-19 positive should wear masks effectively to prevent the spread of the infection to others, including health care workers.
Footnotes
Authors’ Note
Ethical clearance was obtained from the Institutional Research Review Committee (IRRC) of Dodoma University (UDOM/MA.84/261/01/85). All mothers gave both oral and written informed consent after discussing the purpose of the study and issues of confidentiality. Strict ethical standards and procedures were adhered to, and the anonymity of the participants was observed. Written informed consent was obtained and a copy of the consent form was given to each participant. Participants were free to withdraw from the research at any stage without incurring any cost.
Acknowledgments
The authors are grateful for the support which was provided by the Department of Clinical Nursing, School of Nursing and Public Health, University of Dodoma, and also the study participants.
Authors’ Contribution
SA: conceptualization, designing, data collection, data analysis, and writing the first draft, AAJ: methodology, supervision, writing the first draft of the manuscript, and in-depth literature search. All authors reviewed the final version of the manuscript and they agree to be accountable for the intellectual contents of the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.