
Abstract
Introduction
Ostomy 1 stigma negatively impacts the health of people with an ostomy and contributes to a lower quality of life and health outcomes.
Objective
To assess whether participants experience perceived stigmatizing sentiments (SS) from medical clinicians at the time of their ostomy procedure.
Methods
Using a nonprobability sample of 312 persons with an ostomy, we conducted a retrospective descriptive study. We measured SS as patients’ self-reports of verbal and non-verbal communication from clinicians that were perceived to be negative and may contribute to ostomy stigma. We used thematic analyses to analyze open-ended written comments.
Results
Findings indicate that ostomy patients experience stigmatizing sentiments from their medical clinician before and after surgery. Sixteen percent of patients reported a SS, such as clinicians stating feelings of disgust, showing visible signs of disgust, or treating patients negatively regarding the ostomy.
Conclusion
The perceived treatment that this patient cohort experienced in healthcare likely contributes to ostomy stigmatization and may impact ostomy patients’ psychosocial adjustment. Future research should examine the specific consequences of perceived stigmatizing sentiments from medical clinicians.
Introduction
Stigma is a pressing social issue that contributes to disparate medical treatment of marginalized groups (Major et al., 2018). The disparate treatment, in turn, may contribute to disparate outcomes and health disparities. In this paper, we examine the extent to which persons with an ostomy experienced perceived stigma from medical clinicians.
Scholars have theorized about stigma and stigma-related mechanisms for decades (Goffman, 1963; Kleinman & Hall-Clifford, 2009; Major et al., 2018). Modern scholarly stigma research owes a great deal to Erving Goffman (1922–1982) who proposed two types of stigma: (a) a discredited stigma, where the stigma is known to others or assumed as known to others, such as race or a visible disability, and (b) a discreditable stigma, where the stigma is unknown or concealable to others (i.e., passing as normal (Briggs et al., 1977)), such as HIV status or mental illness (Goffman, 1963), or an ostomy appliance, which is generally attached to the abdomen (i.e., there are internal ostomy devices without a bag attached to the abdomen) and hidden under clothing; thus, ostomy stigma may (or may not) be concealable in everyday life. Concealability is the extent to which a stigma can be seen by others (Jones et al., 1984). As concealability pertains to an ostomy, it can be concealable until the pouch becomes full of gas or bodily fluids and then it may become exposed or balloon up so that clothing moves away from the body, or it may be heard passing gas, or it may leak bodily fluids on the front of clothing. However, concealability would be impossible with medical clinicians when the patient is at the hospital for ostomy surgery. Therefore, ostomy patients would not be able to conceal their stigmatized status in this scenario.
While both types of stigma may result in negative psychological affects (Chaudoir et al., 2013), there is an important difference between the two forms: persons with a discredited stigma (known to others) are perceived as “tainted” and may be more likely to experience a stigmatizing sentiment due to the inability to hide their stigma (Chaudoir et al., 2013). A stigmatizing sentiment refers to negative communication—both verbal and nonverbal—about a label, group, or condition that is devalued by society (Aakre et al., 2015; Kroska & Harkness, 2006). Stigmatization can vary in degree and the way(s) it affects individuals, and result in patients being secret about their stigmatized status or withdrawing from the social world, for example (Link et al., 1997). In the current article, we examine ostomy patients’ perceived experience of stigmatizing sentiments from medical clinicians. Addressing this issue will allow us to further examine ostomy patients’ responses to perceived stigma, such as social withdrawal and isolation.
Review of Literature
A large body of literature has examined stigma-related processes, such as race as a stigmatized status (Cohen, 1999; Sacks, 2019), obesity stigma (Fruh et al., 2016), mental illness stigma (Kroska & Harkness, 2006; Link et al., 2001), cancer stigma (Chapple et al., 2004; Phelan et al., 2013; Shen et al., 2016), substance use stigma (Chang et al., 2016), inflammatory bowel disease stigma (Taft et al., 2012), HIV stigma (Li et al., 2007), sexual orientation stigma (Williams & Mann, 2017), transgender stigma (Kosenko et al., 2013; Poteat et al., 2013), and to a smaller degree, ostomy stigma (Qin et al., 2020; Smith et al., 2007). Furthermore, several studies have examined ostomy patients’ experiences in everyday life (Claessens et al., 2015; Danielsen, Burcharth, et al., 2013; Diebold, 2016), and health outcomes, such as how living with an ostomy negatively affects quality of life (Erwin-Toth, 1999; Grant et al., 2011; Popek et al., 2010), alters a patient's body image (Black, 2004), and results in feelings of anxiety (Richbourg et al., 2007) and shame (Colman, 2014; Diebold, 2016). Quantitative studies have examined ostomy patients’ quality of life in relation to working with an ostomy care nurse (Aronovitch et al., 2010), and analyzed perceptions of quality of care (Persson et al., 2005). Overall, research on ostomy patients’ healthcare experiences tends to focus on patients’ knowledge or adjustment relating to the type of ostomy instruction on how to clean and care for their ostomy they received at the hospital, such as educational materials, video tutorial, verbal instruction, or a combination (Colwell & Gray, 2007; Crawford et al., 2012; Haugen et al., 2006; WOCN, 2018). By contrast, very few studies have examined ostomy patients’ outcomes based on interactions with medical clinicians at the time of ostomy surgery.
The current article focuses on an unanswered question in the ostomy stigma literature regarding whether people with an ostomy perceive experiencing stigmatizing sentiments from medical clinicians. Living with an ostomy may be stigmatizing and can result in feelings of shame, anxiety, and fear (Diebold, 2016; Richbourg et al., 2007). Understanding the sources of that stigma—specifically, whether medical clinicians contribute to that stigma—is an important step for addressing the shame, depression, and social isolation that results from a stigmatized identity.
The Stigmatization Process
People learn about stigmatized identities, such as what it means to be mentally ill, or to have a disability, through the process of socialization where individuals develop beliefs about being devalued and discriminated against because of their condition (Link et al., 1997). Based on these cultural beliefs, individuals internalize what it means to be attached to a stigmatizing label. As this process pertains to ostomy stigma, culturally induced conceptions of an ostomy appliance include a social taboo regarding the excretion of bodily fluids (Black, 2004; Briggs et al., 1977; Chelvanayagam, 2014). By definition, a social taboo is a prohibited practice in society (Brown, 2020). Stigmatized topics make them a taboo topic of conversation (Hudson & Okhuysen, 2014).
Feelings of disgust play a central role in the taboo topic of bodily excretion. Secretions from the body often evoke the emotion of disgust (Curtis & Biran, 2001). In Haslams (2012) book, Psychology in the Bathroom, he describes the tendency for people to keep the act of excretion hidden because it is a personal and a private practice, even though these practices are universal to living (p. 3). Haslam postulates that humans hold feelings of disgust and fear of fecal contamination and a dread of parasite-borne diseases; as a response, humans try to put great distance between “ourselves and our waste” due to this disgust (Haslam, 2012, p. 2). Anthropologists have studied disgust and proposed that there is an area in the brain where disgust may reside, and that disgust emotion is an adaptive response to the threat of disease (Curtis & Biran, 2001, p. 17). Disgust research stems from investigating hygiene behavior and the law of “contagion,” which holds that once you are in contact with a contagion then you are always in contact with the contagion (Rozin et al., 1986). Manifestations of disgust include a number of outward behaviors, such as facial expressions, explicit statements like “ew” “ick,” and even neurological signs, such as low blood pressure (Curtis & Biran, 2001).
Previous research shows a relationship between ostomy stigma and level of ostomy adjustment (Qin et al., 2020; Xu et al., 2019), perceptions of attractiveness (MacDonald & Anderson, 1984), and disgust sensitivity with respect to the idea of being in close proximity to someone with an ostomy (Smith et al., 2007). This study addresses gaps in the ostomy stigma literature by examining a potential source or origin of stigma. More specifically, we investigate whether ostomy patients experience perceived stigmatizing sentiments from medical clinicians after ostomy surgery.
Methods
Research Question and Design
To address the research question of whether ostomy patients perceive experiencing stigmatizing sentiments from medical clinicians, we use data from a cross-sectional study of 312 persons who self-reported to have an ostomy. Patients could have had an ostomy for any reason (e.g., cancer, inflammatory bowel disease, trauma, etc.). We collected data between April and December of 2019, recruiting from 166 support groups affiliated with the United Ostomy Associations of America (UOAA), posted the questionnaire link on UOAA's discussion board, and we recruited through Facebook ostomy support groups, Twitter, and MeetAnOstomate's website discussion board. We secured a small grant from the University of Oklahoma in Norman, Oklahoma to incentivize participation by entering respondents into a drawing for the chance to win $25.00 Amazon gift cards. Overall, we received responses from a total of 353 respondents. The current study uses responses from 312 participants. Forty-one observations are excluded from the analyses because they have missing data on variables of interest in the current study. The omitted observations did not differ substantially from the observations included in the analyses.
Institutional Review Board Approval
The study and methods were approved by the IRB at the University of Oklahoma in 2019.
Inclusion and Exclusion Criteria
Eligibility to participate included self-identifying as having an ostomy, being aged 18 or older, and the ability to read and write English well enough to complete the questionnaire. Prior to accessing the questionnaire, respondents signed an electronic informed consent form, and the questionnaires were self-administered and comprised of closed-ended and open-ended questions.
Variables
To answer the research question of whether ostomy patients experienced perceived stigmatizing sentiments from medical clinicians at the time of ostomy surgery, we analyzed the following open-ended question, “Was there a particular medical provider who made you feel bad about your ostomy? If yes, what did the medical provider do to make you feel bad about your ostomy? Please describe in the box below.” We asked this general question rather than specific components of stigma in order for respondents to be able to respond with any verbal or nonverbal form of communication from clinicians that the patient perceived as a negative sentiment. We used thematic analyses to examine written comments. A stigmatizing sentiment refers to negative communication—both verbal and nonverbal—about a label, group, or condition that is devalued by society (Aakre et al., 2015; Kroska & Harkness, 2006). Thematic analysis involves focusing on the narratives of the individuals in the data, repeated words or phrases (Grbich, 2013), and is a flexible approach to identifying patterns within data and a way to understand broader cultural meanings (Braun & Clarke, 2006).
We also report basic demographic characteristics of the study sample. All demographic characteristics are self-reported by the respondents. Gender was collected dichotomously with the categories male and female. The variable race/ethnicity included the following categories: Hispanic White, Hispanic Black, American Indian or Alaska Native, Black/African American, Asian, Asian American, White/Caucasian/non-Hispanic, Native Hawaiian or Other Pacific Islander, and Other (please specify). Because there were so few respondents in categories other than White/non-Hispanic, we collapsed the categories into the categories White and non-White. Education was measured by the following categories: less than high school degree, high school degree, some college, completed an associate degree, completed a bachelor's degree, completed a postgraduate degree. The education variable was collapsed into four categories: high school or less, some college, bachelor's degree, postgraduate degree. Age was measured in years. Time since the respondent had the ostomy surgery was measured in years. We recorded the geographical location of the ostomy surgery. Respondents included information about the hospital as well as the city and/or state where the surgery occurred. In the results below, we indicate whether the surgery occurred in the U.S. or outside the U.S.
Analyses
We present patient demographic characteristics of the study sample and subthemes found upon analyzing the open-ended comments. To analyze the open-ended written comments, we used thematic analyses using QSR NVIVO qualitative data analysis software (QSR, 2021). Once the initial thematic analysis was complete in NVIVO in identifying stigma sentiments, we examined the stigma sentiments for subthemes, and we present these subthemes.
Results
Sample Characteristics
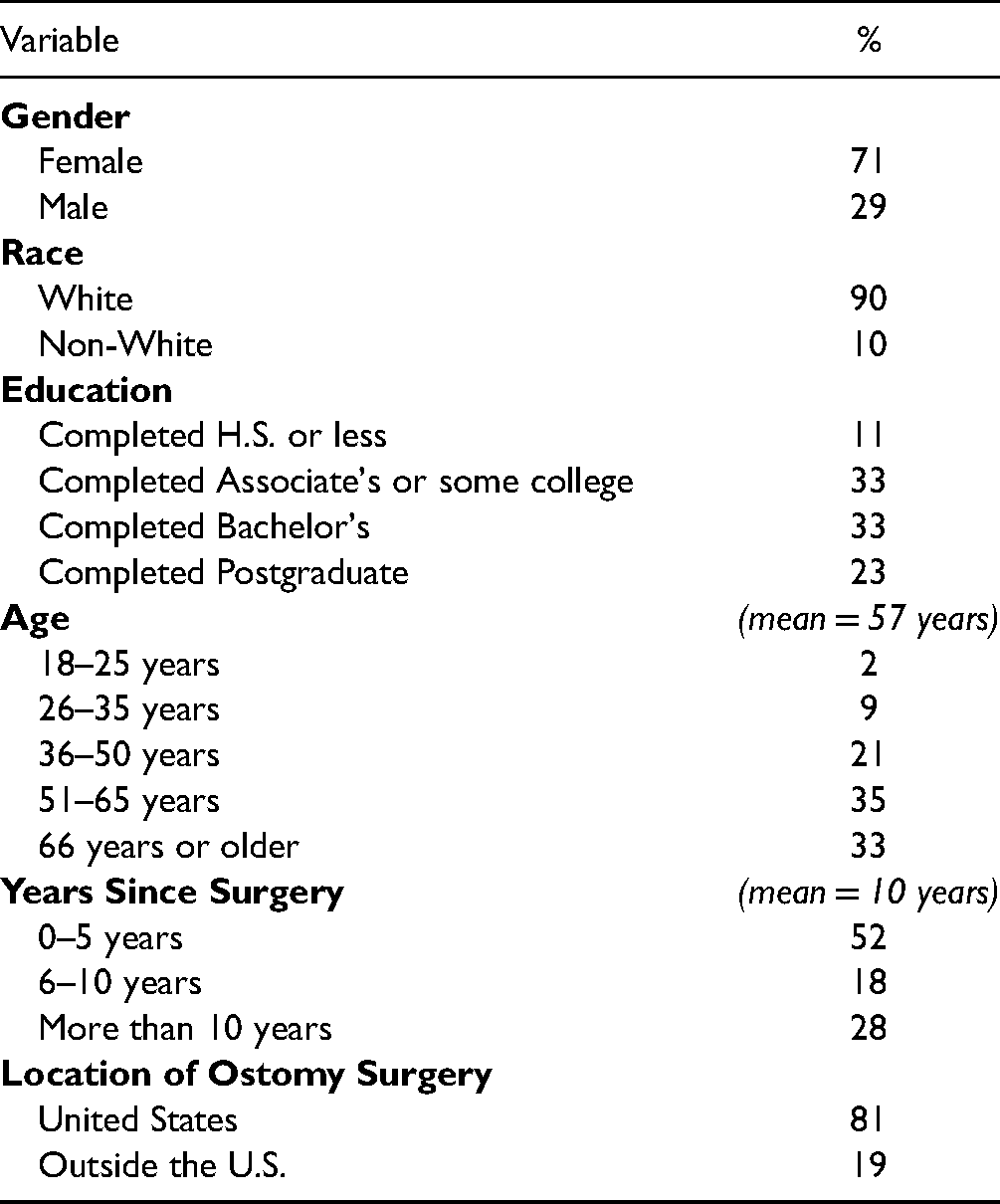
Table 1 shows frequencies and percentages of the variables describing the sample. The sample is majority White and female, with education levels higher than the U.S. average (U.S. Census Bureau, 2019), and age higher than the U.S. average (U.S. Census Bureau, 2019). There are 312 participants with an ostomy included in the current study. Almost three-quarters (71%, n = 221) of the sample are women, and an even higher percentage are white (90%, n = 280), slightly more than half of the sample (56%, n = 174) have a bachelor's degree or higher. The mean age for participants is 57 years old. The mean years since ostomy surgery is 10 years. Finally, nineteen percent (n = 59) of the participants had their ostomy surgery outside of the United States; the non-U.S. sample had surgery in Canada or the United Kingdom (the specific countries are not shown in Table 1).
Characteristics of the Study Sample (n = 312).
Research Question Results
While the majority (n = 254, 81%) of participants reported that they did not experience a verbal or non-verbal interaction that was perceived as stigmatizing, we found that 16% (n = 49) of the sample reported experiencing a verbal or non-verbal interaction that was perceived as stigmatizing, with a small percentage (n = 9, 3%) that did not know.
The thematic analyses of the respondent's written comments identify perceived stigmatizing sentiments from medical clinicians, and we identified eight subthemes reflecting cultural values and norms about ostomies. The following subthemes were identified as they relate to medical clinicians’ sentiments: (a) age-related, (b) patient at-fault, (c) body-specific or sexuality, (d) disgust, (e) medical gaze, (f) negative experience, (g) treated as less than human, and (h) uncaring or rude (see Table 2 for the descriptions and frequencies). We present respondents’ quotes for each of these themes. Note that many statements and descriptions from the participants can fall under multiple themes.
Description and Frequencies of Subthemes of Stigmatizing Sentiments.

Discussion
The current study investigates perceived stigmatizing interactions with medical clinicians for ostomy patients. We asked patients whether they experienced communication from medical clinicians that made them feel bad about their ostomy. We operationalized ‘feeling badly’ as patients experiencing a verbal or non-verbal interaction in the medical encounter that was perceived as stigmatizing. The stigmatization process includes discrimination, which is when a person intentionally and overtly treats another person in a negative manner; the effects of stigma on individuals may result in feelings of shame, self-doubt, anxiety, among other harmful effects (Major et al., 2018). We found that ostomy patients reported experiencing a verbal or non-verbal interaction that they perceived as stigmatizing
Results from the analyses of the respondents’ written comments elucidate this process of stigmatization for those ostomy patients who perceived stigmatizing sentiments from the clinician. There were several notable subthemes identified in perceived stigmatizing sentiments that medical clinicians made to ostomy patients, such as visible signs of disgust or explicitly stating their feelings of disgust when providing medical care to ostomy patients; the patient was treated as if the medical situation was their fault; statements about the patient's age and having an ostomy or how the ostomy will negatively impact their quality of life as they grow older; patients were treated as less than human because of their ostomy or treated as just a number; finally, patients described a negative encounter with their clinician or had an uncaring or rude medical clinician. Similar results have been found in clinician-patient research for patients with substance use issues (Chang et al., 2016), patients with lung cancer (Chapple et al., 2004), and patients perceived as obese by clinicians (Fruh et al., 2016).
Strengths and Limitations
While the findings help to understand ostomy patients’ experiences with medical clinicians after ostomy surgery, there are several limitations of the study to consider. The primary limitation is related to the selection of study participants. The data were collected using nonprobability selection methods. This, in turn, can result in selection bias or differences between participants in the study and those not in the study. While there are multiple sources of selection bias, the most common are self-selection and selection from specific areas (Berger & Christophi, 2003). Self-selection occurs when individuals can decide whether to participate in the research or not, in which case, the selected sample may not accurately reflect the entire population. In the current study, the participants are disproportionately white and female. The types and frequency of stigmatizing sentiments may be different for white females than for other groups. In addition, the disproportionate number of white and female participants prevented us from making comparisons across race and gender. The other likely source of selection bias present in the current study is related to participants coming from a specific area. This often refers to geographical areas. In our case, however, it refers to selecting participants from ostomy support groups. It is possible that persons living with an ostomy who are not part of a support group are different than those who do participate in a support group. It is possible these two sources of selection bias are related. That is, it may be the case that ostomy patients who are non-white and male may not participate in ostomy support groups at the same levels as white females. While not the focus of this research, this relationship should be investigated.
Another important limitation of the study is the retrospective measurement of key variables. Participants reported and described events that occurred in the past. The average time from the data collection to the ostomy surgery was eight years. The retrospective study design has the potential to introduce recall bias, which is remembering an experience as “better or worse than it actually was” (Blome & Augustin, 2015, p. 112). While recall bias is a potential limitation in the current study, research suggests that events that hold an emotional significance are more likely to be recalled with more accuracy than more mundane events, especially those affectively-relevant aspects of an experience (Kensinger, 2011). That is, an event that triggers a strong emotional response is likely to result in a lasting and accurate memory (Murphy & Isaacowitz, 2008).
Conclusion
This study demonstrates that ostomy patients perceive experiencing stigmatizing sentiments and negative treatment in the medical encounter because of their ostomy. Stigmatizing sentiments from medical clinicians likely contribute to feelings of anxiety, fear, and shame for patients.
Implications for Practice
The findings suggest several important implications and directions for clinical practice and for future research. The first implication is related to improving clinical care for ostomy patients, such as more education for medical providers on best-in-practice approaches to ostomy care, as well as more resources for ostomy patients after discharge. The findings suggest that there is significant room for improved clinical care. Previous research has demonstrated that ostomy patients live with feelings of stigma. Sentiments from clinicians are likely contributing to that stigma. Previous research also shows ostomy care in the United States is lacking (Gleba & Mantell, 2020; Miller & Peck, 2019). As such, the United Ostomy Associations of America (UOAA) has developed recommended standards of care in their ostomy Patient Bill of Rights (UOAA, 2019), which is a tool that assists ostomy providers when caring for ostomy patients, and it is a self-advocacy tool for patients.
In addition, the findings suggest important directions for future research. Most notably, future research should investigate ostomy stigma further by quantitatively examining whether there is a statistically significant relationship between medical clinician communication and subsequent feelings of stigma from patients. The current study has demonstrated that patients perceive stigmatizing sentiments from clinicians. It is an open question whether the communication contributes to long-term or sustained ostomy stigma. Another important issue relates to the sources that contribute most to stigma for persons living with an ostomy. At least two lines of research are warranted. One line of research involves the relative impact of the medical encounter as a source of stigma compared to more general social sources. The relative importance of these two sources is not well understood. The other issue worth exploring is the relative importance of specific medical providers. The current study is not able to distinguish between physicians, nurses, and other providers. If interactions with medical clinicians do contribute to stigma, future research should evaluate the relative importance of physicians and other providers within the medical sector.
Footnotes
Acknowledgments
The authors would like to thank the United Ostomy Associations of America for their ostomy patient support, and advocacy. In addition, they would like to thank the hundreds of people living with an ostomy who provided data for this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received a Graduate College Foundation Fellowship from the University of Oklahoma to support parts of the research presented in this article.