
Abstract
Introduction
Secondary traumatic stress is highly prevalent among nurses, especially among nurses working within the emergency department (ED). Reducing healthcare worker secondary traumatic stress is important for ensuring the delivery of high quality, safe patient care. This paper reports on the development and implementation of a secondary traumatic stress reduction program.
Methods
We used an adaption of a 5-week intervention based on the Accelerated Recovery Program to test whether there would be a reduction in secondary traumatic stress in a pilot sample of nine ED nurses. Outcomes were assessed using the Secondary Traumatic Stress Scale (STSS), Somatic Symptoms Scale (SSS), and Compassion Satisfaction subscale (CSS) measures.
Results
Eight of nine nurses were able to complete at least three of the five sessions. Results indicate significant change in STSS (F[5,23] = 4.22, p = .007) and SSS (F[3,15] = 4.42, p = .02) scores, but not CSS (F[5,23] = 0.83, p = .54) scores. Pairwise comparisons revealed that the beneficial effects of the program happened early. For both STSS and SSS, scores at sessions 1 and 2 were generally higher than subsequent sessions. We also found a trend for continued effects on STSS at a four-month follow-up (t23 = 1.95, p = .064).
Conclusion
Overall, results indicate the 5-week program was associated with a significant reduction in secondary traumatic stress and related somatic symptoms in healthcare workers.
Introduction
Secondary traumatic stress and post-traumatic stress disorder are interrelated but distinct concepts. Secondary traumatic stress (STS) occurs as a result of direct practice or exposure to victims of trauma and is manifested behaviorially with symptoms that mirror post-traumatic stress disorder (PTSD) (Figley, 1995). The diagnostic criteria for PTSD include re-experiencing the traumatic event, avoiding reminders, and ongoing hyperarousal. Though the symptoms can be similar, a key difference is characteristics of the instigating event. The DSM-5 critera for PTSD requires “exposure to actual or threatened death, serious injury, or sexual violence.” This was expanded to include “repeated or extreme exposure to aversive details” of an event which in effect broadened the criteria to include that beyond direct experience (American Psychiatric Association, 2013). In contrast, STS can develop from exposure to events that may be neither repeated nor extreme in that they arise vicariously through others and as a result does not necessarily meet criteria for PTSD (Sprang et al., 2019).
STS is common in healthcare settings and has been observed in 18–33% of nurses (Beck, 2011; Dominguez-Gomez & Rutledge, 2009; Mealer et al., 2007; Mealer et al., 2009; Oginśka-Bulik et al. 2021). STS is associated with increased job turnover (Bride & Kintzle, 2011; Burlison et al., 2016), absenteeism (Burlison et al., 2016), reduced confidence, and secondary medical errors (Kruper et al., 2021). A related concept is compassion fatigue first coined to describe burnout phenomena in high acuity nursing contexts (Joinson, 1992). It was later adapted as a synonym for STS that was less stigmatizing to healthcare workers (Figley, 1995). The term has evolved since to connote difficulty with empathic engagement with patients as a result of work-related stress.
In addition, STS can result from the distress arising from medical errors and adverse patient events (Kruper et al., 2021). These effects may not be uniformly distributed across the workforce. Some studies suggest that nurses are at higher risk for STS than other medical professionals (Haik et al., 2017). Risk factors that aggravate or magnify the effect of STS include younger age, newness to the field, pre-existing anxiety and mood disorders, prior traumatic experiences, and non-ideal coping strategies such as distancing or detaching (Newell & MacNeil, 2010). In nurses, social and behavioral risk factors also include lack of social support systems, substance use, and absence of hobbies (Von Rueden et al., 2010). At the organizational level, the absence of adequate clinical supervision, supportive colleagues, and acknowledgment by the organization of the existence of STS are all contributing factors to the development of STS (Newell & MacNeil, 2010). Conversely, studies have documented a number of protective factors against the development of STS, including male sex, being older, increased work experience, training in the treatment of psychological trauma, positive coping styles, and more autonomy in work environments (Sprang et al., 2007).
There is limited data regarding how to specifically address the specific concept of STS in healthcare workers (Bercier & Maynard, 2015). As a result, potentially effective approaches to preventing, managing, and treating STS rely on data from the treatment of acute stress disorder (ASD) and PTSD as the behavioral manifestations are essentially identical. ASD differs from PTSD in that symptoms have been present for less than one month. Literature has reported that comprehensive organizational support systems are recommended to manage secondary victimization (Dekker, 2013). Attempts have been made to develop short-term intervention strategies following acute trauma to reduce the incidence and severity of traumatic stress symptoms. Single incident debriefing is one such example; however, its effectiveness at reducing STS is unclear, as meta-analytic studies have found no reduction or even deleterious effects of single incident debriefing sessions (Van Emmerik et al., 2002). Why this intervention has been not found to be helpful or may even be harmful is not clear.
In contrast, Cognitive Behavioral Therapy (CBT) is one of the more effective treatments for ASD, with both acute and long-term beneficial effects (Bryant et al., 1999; Bryant et al., 2003; Tol et al., 2013). CBT has not been associated with short- or long-term worsening of prognosis, and the effects of CBT appear to be larger than other interventions, such as supportive counseling (Bryant et al., 1999; Bryant et al., 2003). Results from empirical work in ASD indicate that psychological ventilation with a supportive listener is not sufficient to reduce trauma-related symptoms, suggesting the additional need to skillfully address dysregulated feelings and thoughts associated with trauma (Bryant et al., 1999; Bryant et al., 2003).
These findings in ASD are mirrored in the treatment of PTSD. Two forms of CBT, prolonged exposure (PE) and cognitive processing therapy (CPT), have confirmed, albeit imperfect, efficacy in reducing PTSD symptomatology based on a meta-analysis of randomized controlled trials (Steenkamp et al., 2015) (Kline et al., 2018). Exposure to the traumatic event in a therapeutic, skills-based framework such as CBT has thus emerged as a common component of effective approaches to PTSD.
When considering the problem of STS among workers in medical settings, current approaches to PTSD have three notable limitations. First, healthcare workers who meet criteria for diagnosis of PTSD may have difficulty accessing evidence-based treatment, due to system problems like work demands, availability of services, and stigma against seeking help; thus, making such treatments available to all health care workers difficult. Second, less than 10% of trauma victims develop ASD and/or PTSD (Breslau, 2009); thus, not all traumatized individuals may require a full treatment course. Third, given the ubiquity and chronicity of exposure to STS in healthcare workers, the need for preventative approaches is heightened.
One promising program to reduce compassion fatigue among workers in high-stress careers is the Accelerated Recovery Program (ARP), developed and refined to assist professionals suffering from STS as a result of the Oklahoma City Bombings (Gentry et al., 2004). ARP consists of a series of 4–5, 90-min training sessions that provide: 1) psychoeducation about CF; 2) experiential exercises conducted in pairs to address difficult memories; and 3) cognitive exercises to confront trauma-based feelings and thought patterns that are interfering in daily life (Gentry & Baranowsky, 1999). There have been two prospective studies of the ARP using a non-randomized, pre-post design, showing reductions in STS and burnout 6–12 months after training in both oncology nurses (Potter et al., 2013) and ICU and emergency room nurses (Rajeswari et al., 2020). Interestingly, an adaption of the ARP that condensed training into a single, four-hour session also found that it significantly decreased burnout and secondary traumatic stress (Flarity et al., 2013).
We sought to develop a quality improvement program to reduce STS and somatic symptoms in nursing staff who were impacted by changes in patient volume and acuity following the reopening of The University of Chicago Medical Center Level-1 trauma center. Emergency department nurses are known to be at risk for STS (Dominguez-Gomez & Rutledge, 2009; Duffy et al., 2015; Ratrout & Hamdan-Mansour, 2020). The purpose of this paper is to describe a local adaptation of the ARP that was developed for this population and to report the results of the intervention among a pilot sample of emergency room nurses who participated in the program in the first year following the reopening of the Level 1 Trauma Center.
Methods
The intervention protocol and plan for anonymized data collection were submitted to the Chief Quality & Innovation Officer in the Center for Health Discovery Science and Innovation at The University of Chicago Medicine who determined that the project met the definition of Quality Improvement and did not require additional review by the IRB, given that no identifying information was collected and no experimental procedures were implemented. Nine emergency department (ED) nurses volunteered to participate in a 5-week intervention during the spring of 2019. Participants were recruited by the nursing manager based on willingness to participate and work in high acuity shifts characterized by frequent exposure to trauma activations. Contextually, the need for this program was recognized by by the ursing manager, the nursing staff, and the project team, based on qualitative reports and observations from the nursing manager. All participants provided informed consent to participate in the five week program and data collection. Four sessions occured at one-week intervals, with a 5th session held three weeks after the 4th session. Each session was 120–150 min starting at 7:30 am. Coffee and a light breakfast were provided. These sessions occurred at the beginning or end of participants’ 12-h shifts. All sessions were led by a psychiatrist and a psychiatric resident.
Intervention
Session 1: Introduction and Assessment
This session began with an introduction to the program, including a description of the purpose of the program and a notice of confidentiality. Group discussion centered on what has and has not worked for managing participant stress. Participants broke out into pairs to discuss why they became an ER nurse and what kept them coming back into work every day. Participants then voluntarily shared their experiences with the group if they felt comfortable doing so.
Next was a psychoeducation presentation on the topic of trauma, different symptom presentations, and treatment options, including the gold standard of exposure therapy. We described the concepts of Secondary Traumatic Stress/Compassion Fatigue and Compassion Satisfaction. We then reviewed physiological response to stress, including effects on the sympathetic and parasympathetic nervous system and how humans are evolutionarily primed to respond quickly to threatening circumstances. We described two gross responses to stressful situations: hyperarousal (agitated, vigilant state) and hypoarousal (numb/detached/depersonalized state). We discussed one theory of pathological responses to trauma as being caused by an inability to integrate a stressful event properly into a timeline – essentially, that either an agitated or a detached state can arise even when not temporally adjacent to the stressful event.
Finally, we introduced the concept of mindfulness as a mitigating factor that could aid in integrating these experiences. We introduced a single item scale termed “Window of Tolerance” which qualitatively assessed arousal so that during all sessions, and particularly during mindfulness, participants could monitor their physiological and emotional responses (Siegel, 2009). See Supplemental Figure 1 for subjective scale. We stressed that mindfulness, while potentially helpful, may not be appropriate for everyone, particularly during sessions where the exercise precipitated warning signs (hyper- or hypoarousal) that participants were outside of their comfort zone. Throughout all sessions and mindfulness exercises, we encouraged participants to monitor physical symptoms and/or responses as a trauma-informed way of ensuring participants would not become overwhelmed by particular components of the sessions or mindfulness exercises.
We also explained that mindfulness sessions would expand in length and complexity over the course of the program. We told participants that if they began to feel uncomfortable or were experiencing either hyper- or hypo-arousal symptoms, they could break from the exercise. The first mindfulness session involved a one-minute guided meditation focused on bringing the individual into the present moment by making them more aware of their breathing with their attention focused on the length and quality of their inhales and exhales. See Supplemental Figure 2 for an example script.
Session 2: Personal & Professional Timeline
The group was divided into pairs to develop a professional timeline of their career with a focus on major milestones, transitions, and setbacks. We instructed participants to identify three core values that propelled them forward in their professional journey.
We then provided brief psychoeducation about traumatic memory reviewing topics covered in the previous session with a focus on how habituation to traumatic experiences is difficult when one engages in avoidance. We informed the group that although traumatic memories are never fully forgotten, habituation helps neutralize maladaptive responses.
Participants reconvened with their partner to share an experience that happened at work that began to erode the core values they had identified earlier. This was referred to as a “stuck point” that could occur when participants directly experienced a traumatic event or witnessed it happening to someone else. We directed the listening partner to not interrupt the person describing the event, although they could use praise and encouragement if sharing the memory was too difficult. We encouraged the listening partner to further share thoughts about the event especially if the narrative described the speaking partner as being at fault. We expressed how sometimes fear can cause individuals to have overly simplistic or self-chastising thoughts about the event. Participants were encouraged to insert this moment into their timeline and we reconvened for group discussion and for participants to share their experiences if they felt comfortable.
We closed with a mindfulness exercise that expanded upon the first session, being more descriptive and of longer duration (5 min). See Supplemental Figure 2 for an example script. As homework, the group was instructed to start thinking about the development of a narrative for their particular “stuck point” trauma.
Session 3: Re-Framing and Reprocessing, Part 1
This session started with a brief review of the prior session, participant feedback, and a review of the homework. We provided brief psychoeducation on the role of cognition and emotion after unexpected events. We detailed initial reactions such as fear, anger, and sadness and secondary ones which have to do with interpretation of the events. We described how secondary emotions like guilt, regret, and shame are influenced by our personal narrative and core beliefs and that these can persist for long after the event.
The mindfulness exercise in this session was a walking meditation, where participants focused on taking steps to foster attention and awareness to the present moment. See Supplemental Figure 2 for an example script.
Session 4: Re-Framing and Reprocessing, Part 2
This session focused on developing and reviewing narratives of “stuck point” traumas identified in the previous session. Participants who felt comfortable shared their narratives. Primary and secondary emotional responses were identified through open-ended questions. Opportunity was given for participants to examine their narratives and hear supportive feedback from their peers.
The session closed with a mindfulness exercise that integrated breath with a full body scan which helps to induce a sense of progressive relaxation. See Supplemental Figure 2 for example script.
Session 5: Self-Supervision, Closure and Aftercare
In the final session we instructed participants to write a letter from a hypothetical supervisor representing what they would hope to hear from a compassionate manager. We asked participants to pair up and share what they had written with a partner. Each participant sealed and addressed their letter which was mailed to them 6 months later. We then emphasized essential components of self-care and discussed what participants currently did to maintain their own self-care.
We closed with a mindfulness session that involved building a sense of progressive, non-judgemental connection with one’s physical surroundings. See Supplemental Figure 2 for an example script.
Measures
A self-report questionnaire assessing outcomes was administered to participants at each session. Participants were asked to create a unique ID that could be used to link their survey responses over time. To protect the privacy of the participants, the survey questionnaire did not collect identifying information, such as gender, age, or race. For the 1st and 2nd sessions, the questionnaire was administered at the end of the session. For the 3rd through 5th sessions, the questionnaire was given at the beginning of the session. It was decided to change the administration of the questionnaire to after the session in order to include the potential therapeutic effects of that question. The questionnaire was readministered approximately four months after the final session to assess potential long-term effects of the intervention.
The questionnaire included items measuring secondary traumatic stress, somatic symptoms, and compassion satisfaction as primary outcomes. All items were derived from standardized assessment tools widely used in research with healthcare professionals. Secondary traumatic stress was measured using the 17-item Secondary Traumatic Stress Scale (STSS), a measure developed to assess symptoms of intrusion, avoidance, and arousal associated with indirect exposure to traumatic events via one's professional relationships with traumatized clients (Bride et al., 2004). The STSS shows excellent reliability and convergent and discriminatory validity among healthcare professionals (Kellogg et al., 2018). We assessed physical indicators of stress using the 8-item Somatic Symptoms Scale (SSS) (Gierk et al., 2014). The SSS has excellent psychometric properties and has been robustly linked to depression, anxiety, and quality of life in healthcare professionals (Gierk et al., 2015; Touissaint et al., 2017). Finally, we used six questions from the 10-item Compassion Satisfaction subscale (CSS) from the Professional Quality of Life Measure (Hundall-Stamm, 2009) to assess pleasure derived from doing one's job well. The CSS subscale has adequate psychometric properties (Hemsworth et al., 2018) and has been inversely associated with burnout and secondary traumatic stress (Hinderer et al., 2014).
The response scale for all items was: Never (0), Rarely (1), Occasionally (2), Often (3), Very often (4). Items for the STSS were recoded 1 to 5 for comparison with published scale. One respondent was missing data on a single item on one assessment of the STSS, and a different respondent was missing data on a single item on one assessment of the CSS. Data from these two subjects were imputed using the average of each respondent's non-missing items. All items were then summed within scales to create single composite scores for the STSS, SSS, and CSS at each time point. Due to a procedural error, the SSS was not administered during session three or at follow-up.
Data Analysis
Data analysis was conducted with SAS software, version 9.3 for Windows. Copyright © 2002–2010, SAS Institute Inc. SAS and all other SAS Institute Inc. product or service names are registered trademarks or trademarks of SAS Institute Inc., Cary, NC, USA. PROC MIXED was used to conduct repeated measures analyses for each of the three outcome measures with time as the repeated factor. The mixed effects model allowed for inclusion of all non-missing data and to specify the covariance structure between time points. Model fit comparisons revealed that the compound symmetry covariance provided the lowest AICC and BIC values for CSS and SSS and were only slightly higher in comparison to autoregressive covariance for STSS; thus, all models assumed equal covariance across time points. Pairwise contrasts between time points were estimated using least-squares means tests.
Results
Quantitative Change in Outcomes
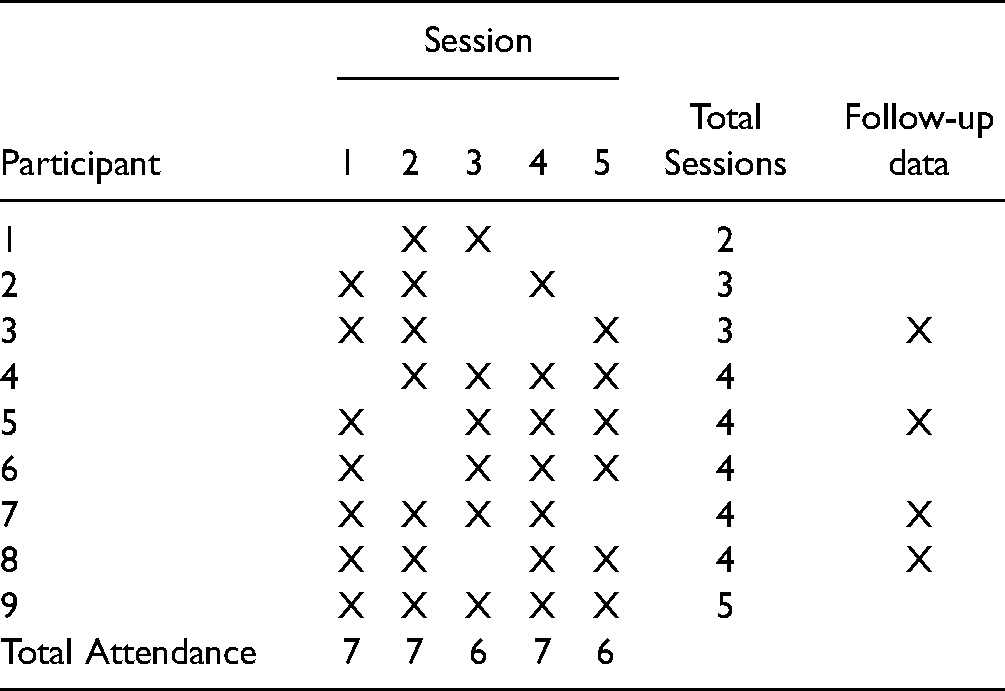
Table 1 shows the attendance patterns of the nine participants. One participant attended all five sessions, one participant attended only two sessions, and the remaining participants attended three or four sessions. All four participants with follow-up data four months after the intervention attended at least three sessions. Using data from the first session attended for each participant, the mean STSS, CSS, and SSS scores were 47.00 (SD = 5.88), 16.20 (SD = 3.63), and 10.22 (SD = 3.15), respectively. Using data from all sessions, including follow-up data, STSS was significantly correlated with SSS (r = .62, p < .001), but CSS was not correlated with either STSS (r = -0.16, p = .36) or SSS (r = -0.05, p = .81).
Summary of Participation.
Figures 1–3 show the estimated least squares means across time points for STSS, CSS, and SSS, respectively. For STSS, the effect of time was statistically significant (F[5,23] = 4.22, p = .007). Pairwise contrasts revealed that STSS scores at session 1 were significantly higher than STSS scores at sessions 3 (t23 = 2.93, p = .008), 4 (t23 = 4.34, p < .001), and 5 (t23 = 3.06, p = .006), with similar trends for comparisons with session 2 (t23 = 1.95, p = .064) and at the 4-month follow-up (t23 = 1.95, p = .064). Scores at session 2 were also significantly higher than scores at session 4 (t23 = 2.33, p = .03). None of the other comparisons across time points were significant. There was no significant effect of time for CSS (F[5,23] = 0.83, p = .54) and none of the pairwise comparisons were significantly different at p < .05. SSS was compared across sessions 1, 2, 4, and 5, given missing data at session 3 and follow-up. The overall effect of time was significant (F[3,15] = 4.42, p = .02). Pairwise comparisons revealed no significant change between sessions 1 and 2 (t15 = 0.73, p = .48). However, SSS scores at session 1 were significantly higher than at session 4 (t15 = 3.16, p = .007) or 5 (t15 = 2.56, p = .02), with similar patterns for comparisons between session 2 and 4 (t15 = 2.36, p = .03) and session 2 and 5 (t15 = 1.81, p = .09).

Mean secondary traumatic stress scale (STSS) scores across sessions and at follow-up. Note. Bars represent standard errors. *p < .05; #p < .10.

Mean compassion satisfaction scale (CSS) scores across sessions and at follow-up. Note. Bars represent standard errors. *p < .05; #p < .10.

Mean somatic symptom scale (SSS) scores across sessions and at follow-up. Note. Bars represent standard errors. Due to a procedural error, the SSS was not administered at Session 3 or at the 4-month follow-up. *p < .05; #p < .10.
Analyses were also re-run using dose (i.e., counting the number of sessions attended by each participant) rather than a week as the measure of time. For STSS, results were virtually identical, with a significant effect of time (F[5,23] 3.91, p = .01) and significant (p < .05) comparisons between STSS scores at the 1st dose compared to scores obtained at the 2nd, 3rd, and 4th doses. The comparison between the 1st dose and follow-up was also significant (p = .05). None of the other comparisons were significant. Patterns for SSS were similar, although the overall effect of dose was significant only at p = .08 (F[4,14] = 2.66), and the only significant comparison was between the 1st and 4th doses (p = .03). Dose was not associated with CSS scores (F[5,23] = 1.23, p = .28).
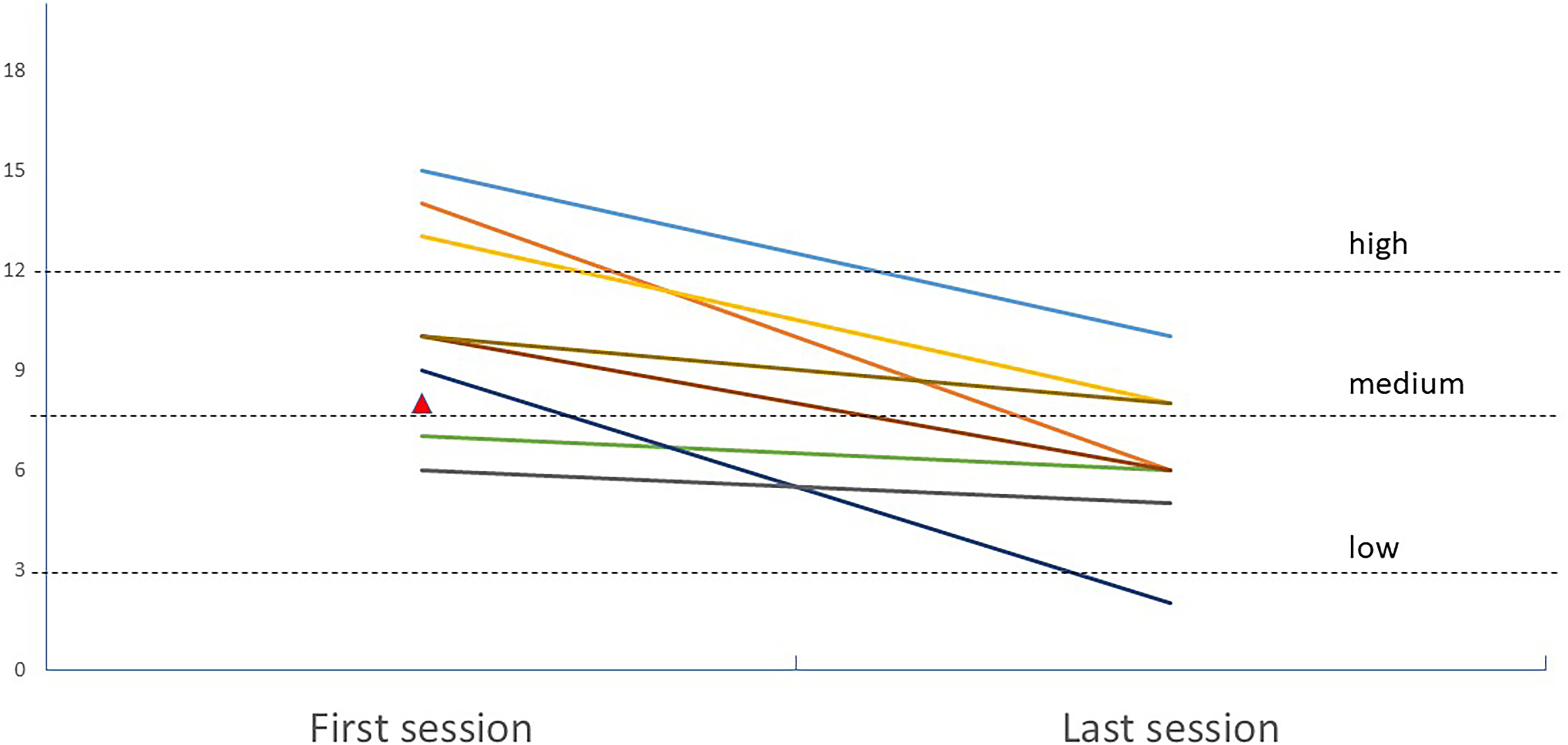
Figures 4 and 5 plot the total STSS and SSS scores for each of the 9 participants at their first and last sessions. For 2 of the 9 participants, their first attendance was at the 2nd session, while the remaining 7 participants attended the 1st session. The last session attended was the 5th session for 6 of 9 participants, the 4th session for 2 participants, and the 3rd session for 1 participant. This last participant did not have data for SSS. At the first session attended, the average STSS score was 47.00 (SD = 5.79), which dropped to M = 37.78 (SD = 4.43) at the last session attended. Seven of the 9 participants scored above the 90th percentile on STSS during the first session attended (based on norms published on Bride et al. 2004). At the last session attended, only 2 participants were still above the 90th percentile. At the first session attended, the average SSS score was 10.22 (SD = 3.15) which dropped to M = 6.38 (SD = 2.39) at the last session attended. Based on published national data from Germany (Gierk et al., 2014), only 2 of the 8 participants had SSS scores below medium at the first session attended; this number increased to 5 of 8 at the last session attended.

Individual scores for the secondary traumatic stress scale (STSS) at each participant's first and last sessions.
Individual scores for the somatic symptom scale (SSS) at each participant's first and last sessions. Note. On participant dropped out after two sessions and did not have SSS scores from the 2nd session.
Adverse Events
We had one adverse event where a participant refused to engage in mindfulness exercises due to high arousal and anxiety when initiating them. This participant chose not to continue in the program, which was voluntary.
Discussion
This study presented detailed information on an adapted 5-session ARP in a cohort of nine emergency room nurses and provided promising initial data to support the program's effectiveness. We saw significant decreases in both STS and somatic symptoms, which were largely retained four months after the intervention. Compassion satisfaction scores remained relatively consistent and did not differ significantly as the program proceeded.
This study adds to a growing body of evidence suggesting that trauma-based CBT programs can be effective at reducing stress levels in frontline medical workers dealing directly with trauma patients (Flarity et al., 2013; Gentry et al., 2004; Potter et al., 2013). Interestingly, the greatest reduction in STS scores occurred between the 1st and 2nd sessions, and there was no relationship between dose and STS. Likewise, the largest reduction in somatic symptoms occurred between the 2nd and 4th sessions, with no apparent impact of dose. This suggests that the 5-week program could potentially be shortened. Although there was no evidence that additional sessions further decreased STS and somatic symptoms, it is possible that additional sessions might be necessary to provide a “booster” effect to maintain lower levels of stress. Future studies with larger samples and to test whether the length of the program significantly impacts the effectiveness of the intervention.
Notably, our program did not seem to impact compassion satisfaction scores. We note that we used an abbreviated version of the CSS to reduce question burden on participants. It is possible that the use of six items rather than the full 10-item scale may have impacted our results. With this caveat, one explanation for the lack of a significant effect of the intervention on compassion satisfaction is that there could be a ceiling effect. Participants in our program already had high levels of compassion satisfaction when they began the program, which may have reduced our ability to detect a significant change in score. As participation was voluntary, selection bias may have contributed to the high levels of observed compassion satisfaction. Thus, caution is warranted in assuming that this finding is generalizable to the larger population from which this group was sampled. Nevertheless, the fact that participant compassion satisfaction scores did not change over the course of the program does suggest that the observed decreases in STS and somatic symptoms are not due to participant desire to report symptom improvement to please the program designers, as one would suspect that compassion satisfaction scores would also be inflated over time if this were the case. Hence, although our sample size was small, we are fairly confident that our results are not biased due to social desirability.
In this study we also found that compassion satisfaction was not correlated with either secondary traumatic stress or somatic symptoms. There is some evidence that the factors that influence compassion satisfaction may differ from those impacting secondary traumatic stress and related constructs, such as burnout and compassion fatigue. For example, in a study using the ProQOL in a sample of ER trauma nurses, burnout and compassion fatigue, but not compassion satisfaction, were associated with hours worked (Hinderer et al., 2014). Conversely, age and education level were associated with compassion satisfaction, but not burnout or compassion fatigue (Hinderer et al., 2014). In a similar study using a national sample of ER nurses, education level, age, years of experience, and hours worked were associated with compassion satisfaction and burnout, but not compassion fatigue (Hunsaker et al., 2015). Burnout and secondary traumatic stress, but not compassion satisfaction, were associated with self-reported stress and anxiety in a sample of Australian nurses in an acute care hospital (Hegney et al., 2014). Thus, it is possible that interventions to reduce stress may have less impact on overall job satisfaction, although additional studies with larger samples are needed to test this hypothesis directly.
Quality improvement is focused on both people and systems, as emphasized by SQUIRE 2.0 guidelines (Ogrinc et al., 2015). With regards to system-level conclusions, the most important one is that implementation of the ARP training program was highly feasible and did not interfere with clinical operations. It did require effort on the part of the nursing manager and the project team to coordinate the training activities. Because we refrained from collecting participant-level data, we did not examine potential system-level effects such as retention and patient outcomes. However, this could be an important target for future work. In addition to the finding of person-level improvement in STS, qualitative feedback was positive. An important system-level observation was that the program participants, members of a high acuity work unit, became more interested in wellbeing projects that they would like to implement. Future studies should also measure such “carryover” effects on system culture and operations that have been relatively negelected by empirical work.
Limitations
The study should be evaluated in the context of several limitations, the most noticeable being the small sample size. The small sample size and quality improvement framework prohibited us from obtaining any detailed data on demographic characteristics or work environment that may have influenced results. In addition, we cannot determine whether improvement in STS and somatic symptoms was due specifically to the effects of the intervention. As participation in the training occurred while at work, it is possible that structured time together may have been beneficial to participants. Due to the nature of their work, which involves fluid, shift-based schedules, most participants missed at least one session. It is possible that we may have found stronger effects if all participants had attended each session and if all measurements had been taken at the beginning of each session. Lastly, although our intervention reduced STS and somatic symptoms in ER nurses in a large urban trauma center, it is unclear if the results would generalize to physicians, technical staff, and workers in other departments or at other institutions.
Implications for Practice
A salient feature of this program is that it was conducted within a quality improvement and safety framework. Administrative support was substantial. Participants did the program as part of their usual work shift and therefore did not have to use vacation or non-work time to participate. This was intentional, given that time away from work is a priority for healthcare worker wellness. Although not measured directly, the trainers themselves found the work meaningful and gratifying. We highlight these features of the program because they are foundational to creating a sustained program in environments characterized by high workloads for both the trainers and trainees.
Conclusion
We developed a 5-session intervention program and observed a significant reduction in secondary traumatic stress scores in a cohort of emergency room nurses who were selected by their managers because of perceived increased stress during their work. We also saw significant reductions in somatic symptom scores. Compassion satisfaction remained relatively high throughout the program though this finding was not significant. The implementation of this program may have affected these different domains. Future areas of research include expanding the model to other departments and including other types of healthcare professionals.
Supplemental Material
sj-docx-1-son-10.1177_23779608221094530 - Supplemental material for A Secondary Traumatic Stress Reduction Program in Emergency Room Nurses
Supplemental material, sj-docx-1-son-10.1177_23779608221094530 for A Secondary Traumatic Stress Reduction Program in Emergency Room Nurses by Lauren K. Robinson, Laura Sterling, Joel Jackson, Eric Gentry, Fabiana Araujo, Cynthia LaFond, Kristen C. Jacobson and Royce Lee in SAGE Open Nursing
Footnotes
Acknowledgments
We would like to thank Kimisha Cassidy and Craig Umscheid, MD, for their administrative support of the project.
Funding
This work was supported by a University of Chicago Medicine Innovations Grant, “Reducing Compassion fatigue in UCMC Health Care Workers,” from The University of Chicago Center for Healthcare Delivery Science and Innovation (HDSI) to author RL.
Declaration of Conflicting Interests
Eric Gentry, PhD is affiliated with the Forward-Facing Institute in Phoenix, AZ which provides an array of services for compassion fatigue resolution and professional resilience including the Accelerated Recovery Program for Compassion Fatigue and the Forward-Facing(R) Professional Resilience workshops. ![]() .
.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.