
Abstract
Background
Drug abuse is an issue that affects all people regardless of gender, race, ethnicity, age, or socioeconomic status. It is associated with a range of physical, social, and economic consequences at both individual and community levels. Community involvement is necessary for effective drug abuse prevention. Communities need to be ready for such involvement.
Methods
We applied the Community Readiness Model and its assessment tool to determine the level of readiness for prevention of drug abuse in Obukpa and Ubollo communities of Nsukka and Udenu Local Government Areas of Enugu North Senatorial zone, Nigeria. Community Readiness Model and the Tool are very useful in identifying gaps in community readiness and capacity as well as guiding strategies for community initiatives. Twelve key informant interviews were conducted and analyzed according to procedures outlined in the Community Readiness handbook.
Results
The results of the study showed that members of Obukpa and Ubollo communities were at the vague awareness stage. SWOT analysis of the qualitative data revealed the strengths, weaknesses, opportunities and threats within the communities for an intended intervention to increase level of readiness. One such strength is the church, which was identified as a viable means of disseminating information on drug abuse prevention in both communities.
Conclusion
Rural communities are vulnerable to drug-related problems as a result of low levels of awareness of the dangers of drug abuse. The findings of this study provided strategies and directions for future intervention programmes in the study area. Nurses and other health personnel involved in Community Health Education should take cognizance of the strengths, weaknesses and opportunities within the communities in designing drug abuse prevention intervention programmes.
Drug use has become a great health challenge in many countries in sub-Saharan Africa (Olawole et al., 2018). Use and abuse of drugs is gradually becoming a norm particularly among youths in many rural communities in Nigeria (Ibrahim et al., 2016). The taking of cannabis, though considered illegal in Nigeria is becoming very rampant. Abuse of alcohol particularly hard liquor is also on the increase (Eze et al., 2017). In 2018, about 15% of the adult population in Nigeria used a considerable level of psychoactive drug (tobacco and alcohol not included). The highest levels of drug use in Nigeria was recorded among people aged 25 to 39, with cannabis being the most widely used drug. The use of sedatives, heroin, cocaine and the non-medical use of prescription opioids were also noted (United Nations Office on Drugs and Crime [UNODC], 2018). The abuse of prescription drugs, such as Tramadol, and household products, such as paints and superglue, are becoming rampant in some rural communities in Nigeria (Dibia et al., 2020).
Alcohol abuse is highly problematic in many communities in Nigeria. Lasebikan and Ola (2016) observed that alcohol consumption is prevalent in semirural communities in Nigeria with the majority of drinkers at moderate or high health risk. The prevalence of alcohol use is rising even among teenagers. It has been reported that more than 50% of male secondary school students in Nigeria moderately consumed beer and local cocktails (Eze et al., 2017). The crude prevalence of harmful use of alcohol in Nigeria as reported by Adeloye et al. (2019) was 34.3% (95% CI: 28.6–40.1). Harmful alcohol use was higher in rural settings (40.1%, 24.2–56.1) compared to urban settings (31.2%, 22.9–39.6).
Drug abuse has been shown to have many negative consequences on the wellbeing of its users. Several studies conducted in Nigeria have shown that drug abuse among Nigerian youth is associated with: poor academic performance of students in Nigeria (Akanbi et al., 2015), low self-esteem (Okafor, 2019), crimes (Ayodele et al., 2018), chronic health conditions (UNODC, 2018), loss of potential manpower, low productivity, and creation of an unfavorable environment for investors which of course will affect Gross National income as well as internally generated revenue (Kawugana & Faruna, 2018).
To combat the growing incidence of drug abuse in many communities, an integrated community prevention intervention is needed. Such intervention must integrate the key elements of community mobilization, environmental intervention in retail shops, home, and school, as well as classroom education (Johnson et al., 2007). One of the major problems observed in the prevention or control of drug abuse is the exclusion of the community in designing and implementation of drug abuse prevention strategies or programmes (Chavan et al., 2017). The community is an important force in halting some unwanted behaviours that threaten the welfare of the community. Every community has its own culturally accepted ways of maintaining peace and preserving values and norms which the community cherishes.
Prevention of drug abuse should start from home, and extend to the community. Involving communities in the prevention of drug abuse can help in reducing the rate of drug abuse through a more youth-friendly and culturally acceptable approach (Johnson et al., 2007). The community should not only participate in prevention of drug abuse but should be actively involved at all levels of prevention for an effective drug prevention strategy.
Indigenes of Enugu state belong to the Igbo tribe. Like other Igbo communities, the people traditionally practice communal life. This is highly evident in rural communities in this area where members of the communities come together to confront problem situations when they arise. In these communities, every member is bound to get involved in such efforts to solve an emerging problem. Sanctions are invoked against any community member that defaults (Ekeopara, 2012). The situation however seems to differ in the urban areas occupied mainly by non-indigenes. Taking advantage of the communities’ communal life by involving them actively in drug abuse prevention will help in reducing the incidence of drug abuse in rural communities in Nigeria.
The relative success or failure of prevention programmes is not just a matter of the quality of planning, but also the issue of the interventions being appropriately matched to the community’s level of readiness (Paltzer et al., 2013). Community readiness is defined as the level at which individuals and groups are willing to accept and support the implementation of new programmes or activities in the community (Donnermeyer et al., 1997). Evidence-based interventions may fail if a community is not interested or has not invested in supporting such programmes (Paltzer et al., 2013).
Community Readiness Model
The Community Readiness Model (CRM) was developed by researchers at the Tri-Ethnic Center for Prevention Research (Oetting et al., 1995) to help communities be more successful in their efforts to address a variety of issues, such as drug and alcohol use and HIV/AIDs prevention (Oetting et al., 2014). The CRM expanded the personal stages of change model and the community development principles to include new dimensions which were unique to communities and programme development. It equally introduced stages within each dimension to track the progress of a community from a state of no awareness, to the community taking full ownership of an issue. The CRM was refined through expert consultation and the application of psychometric principles. The CRM with the Community Readiness Tool (CRT) provides a multifaceted tool to identify gaps in community readiness and capacity while guiding strategies for interventions (Frerichs et al., 2012).
The CRM has five dimensions of community readiness which are scored through the CRT. These dimensions are: Community Knowledge of Existing Efforts, Leadership, Community Climate, Community Knowledge about the Issue, and Resources (Oetting et al., 2014). Results from assessment of these dimensions are used as an indicator of whether a community needs change around an issue. Each dimension is measured through leadership support, community climate, and knowledge. The CRM uses semi-structured qualitative interviews of key informants to assess readiness. Data from the interviews are scored by using anchored rating scales for each dimension and then averaged for an overall quantitative readiness score that corresponds to one of nine stages (see Table 1). Since the 1990s, core researchers at the Tri-Ethnic Center for Prevention Research have promoted the Community Readiness Model. The accompanying CRT has also been shown to be reliable; reported scorer ratings agree 92% of the time (Plested et al., 2005).
Community Readiness Model Stages.

Adapted from Edwards et al., 2000.
The CRM has been used as an intervention tool in many public health issues among diverse populations. In recent studies, the CRM has supported communities in identifying strategies to effect widespread behaviour change. For example, researchers in the Nebraska community used the CRM to guide their work in developing a youth advocacy programme to address childhood obesity within an underserved Latino community (Frerichs et al., 2012). Other studies (Buckner-Brown et al., 2014; Paltzer et al., 2013) used the model to improve the built and social environment and to reduce alcohol consumption. By capitalizing on multisectoral partnerships and implementation of evidence-based strategies, the communities used the CRM to effect substantial environmental changes, such as improved air quality, pedestrian-friendly streets, and walking groups. Overall, the literature suggests that community readiness may be beneficial not only in identifying community readiness, but also in engaging multiple community sectors to support efforts that facilitate positive behaviour change. Since community needs vary, one size cannot fit all in community-level health promotion and disease prevention strategies (Bloch et al., 2014). In this study, CRM served as a theoretical framework and method for measuring the communities’ readiness to prevent drug abuse.
Community involvement is necessary for effective community health programme (Conklin et al., 2015). Community programmes are beneficial in substance abuse prevention. Such programmes are useful in addressing risk factors for substance abuse, such as early aggression, poor social skills and academic difficulty among young people (Chakravarthy et al., 2013). Frerichs et al. (2012) observed that efforts that do not consider readiness for change and tailor strategies to stage of readiness will likely neglect communities with lower readiness but higher need.
This study is therefore set out to identify community readiness for prevention of drug abuse in rural communities in Enugu North senatorial zone, Enugu state Nigeria. The second objective is to identify the strengths, weaknesses, opportunities, and threats in the internal and external environment of the communities for preventing drug abuse. This is hoped to enable an intervention that will increase the communities’ capacity to generate both the demand for and the supply of community-relevant, preventive interventions
Methods
We adopted the qualitative approach to assess the level of drug abuse and readiness of community members to undertake community drug abuse prevention programmes in Enugu North Senatorial zone. Enugu North senatorial zone is made up of Igbo-Etiti, Igbo-Eze North, Igbo-Eze South, Nsukka, Udenu, and Uzo-Uwani Local Government Areas.
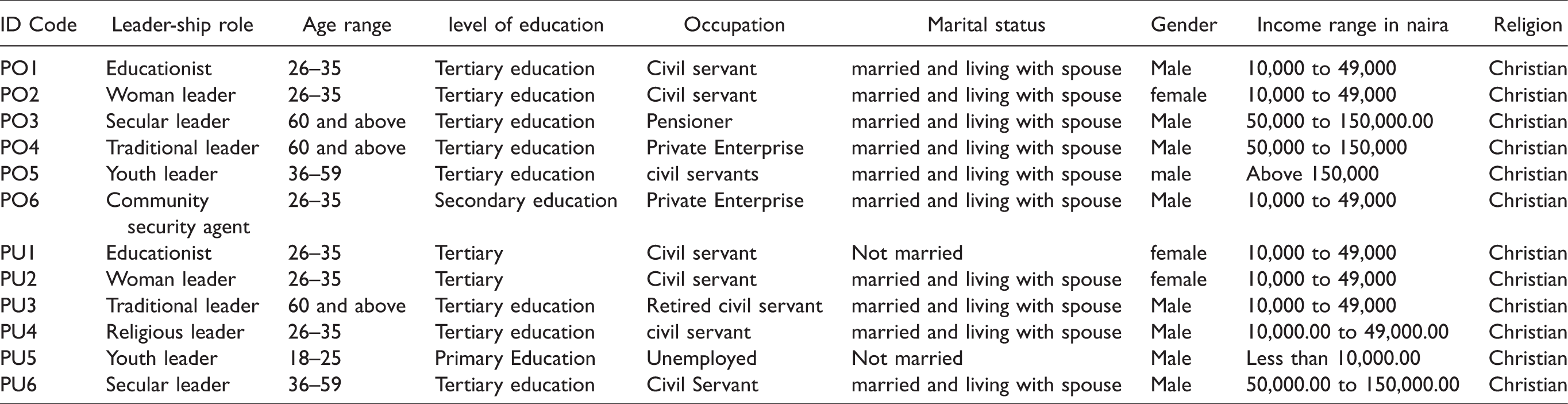
The population for the study comprised all adults and adolescents in the communities. Simple random sampling technique (balloting without replacement) was used to select two Local Government Areas (LGAs) from the zone (Nsukka and Igboeze North LGA). From the sampled LGAs, two communities (Obukpa and Ubollo communities) were randomly selected. We used the snow-ball sampling to select twelve participants. Those selected from the communities were; traditional rulers, community security leaders, youth leaders, women leaders, educationists, and religious leaders. The demographic characteristics of the participants are presented in Table 2.
Demographic Characteristics of Respondents (n = 12).
The community readiness tool (CRT) was used for this study. This tool was developed by Edwards et al. at Colorado State University as a tool to engage the key community members and assess the community’s readiness for change (Donnermeyer et al., 1997; Edwards et al., 2000). The CRT is based on the community readiness model (CRM), which was initially underpinned by the personal stages of change model also called the Transtheoretical model of Behaviour Change (Prochaska & DiClemente, 1992) and community development principles (Rogers, 1983). The CRT consisted of 40 questions. We used the CRT to identify the communities’ stage of readiness for drug abuse prevention. Prior to our using it, we trial tested the CRT questions to ensure that they are comprehensive and systematically structured such that no ambiguities will arise during use of the instrument. Following the CRT protocol we identified 6 leaders as key informants for interviews from each community. By the time we had interviewed the six community leaders in each community, we had reached data saturation and additional interviews yielded no new themes, and that informed our stopping at 12 interviews. These people were adjudged to be connected to the issue of drug abuse prevention in the communities either by occupation or by general health interest or by position. Inclusion criteria was that participant for the CRM interview were living in the communities and were not involved in substance abuse or doing business with substances of abuse. Only those willing to voluntarily participate were interviewed. All the participants were required to give both oral and written informed consent. The interviewer provided a brief introduction to the project and asked the standard CRM interview questions (Oetting et al., 2014). Interviews ranged from 40 to 60 minutes. All interviews were completed in person and audio-recorded.
We transcribed the audio recordings verbatim. Three researchers scored the interview transcriptions independently. The anchored scales range in whole numbers from 1 to 9 for each dimension; 9 represents the most favorable score. Each dimension was rated using the scale (see Table 1 for a description of community readiness stages). The researchers compared scores and, in the case of disagreement, established reliability by reaching a consensus. To compute the total CRM score for each respondent, the ratings of the five dimensions were averaged. The stage of readiness was determined for each community by rounding down the scores (Oetting et al., 2014). The qualitative analysis involved reading and highlighting key comments from each participant’s interview transcript. The highlighted comments were read again to identify those relevant for each dimension. From the highlighted comments, major themes for each dimension were identified. Furthermore we conducted a SWOT analysis to identify the communities’ strengths, weaknesses, obstacles and opportunities (Oetting et al., 2014) to drug abuse prevention action. The study was approved by the research ethics committee of the Faculty of Education, University of Nigeria, Nsukka (REC/FE/2018/000008).
Results
We found that the two communities we studied were at a low stage of readiness to prevent drug abuse in their communities (Table 3). Obukpa community had an overall mean score of 3.39 (SD = 0.36) while Ubollo community had an overall mean score of 3.48 (SD = 0.37) with an overall mean score of 3.44 (SD = .20) for both communities on the 9-point scale (Table 3). Both communities were therefore at stage 3, “vague awareness,” indicating they felt drug abuse was a local issue, and there was no significant effort, to take action, within the communities to prevent drug abuse. The dimension scores did not differ so much in each community except for knowledge of issue where Obukpa scored 2.9 and Ubollo scored 4.02.
Level of Readiness.

Scores were rounded down to determine readiness level.
*At individual community level the level of readiness for this dimension varied.
Knowledge of Efforts
In the two communities, a few community members have heard about local efforts at preventing drug abuse, but know little about them.
Strength
The church was noted as a viable means of disseminating information on drug abuse prevention in both communities. In both communities, nobody is planning to get something started to address drug abuse. However, admonitions on preventing drug abuse generally occur in these communities through church programmes, radio programmes, and talks by elders during gatherings.
Weakness
No specific effort to address substance abuse in the communities. General efforts are seen in the form of crime control by community leaders and preaching by religious leaders.
Opportunities
The church presents a social structure for creating awareness on the need for preventing drug abuse in the communities.
Threats
Poor media coverage and network services will hinder effective dissemination of information on drug abuse prevention through the media.
In Obukpa, although all the participants indicated that there were community-efforts aimed to prevent drug abuse in the community. When asked to describe the efforts, it was revealed that there were no specific efforts targeting prevention of drug abuse in the community. Rather the community makes efforts from time to time by using community security agents and the police to arrest those who abuse marijuana. Those arrested pay fine before they are released. These efforts have been misconceived by some community members as a means by which the community leaders bring vengeance on their enemies in the community and also make money for themselves. The effort is also seen as having a weakness in that the wrong individuals might be arrested by the security agency. This effort also has obstacles … at times those people that smoke Indian hemp, they use to attack these boys (referring to community security agents) that are arresting … maybe they (still referring to community security agents) may arrest the wrong person. Maybe they have a problem with somebody and they arrest the person. (PO2)
Four participants from Obukpa explicitly stated that there were no specific efforts in the community aimed to prevent drug abuse in the community. Participants also revealed that the major means of communicating efforts to community members was through announcements in churches.
In Ubollo, two participants stated that there were no specific efforts by the community aimed at preventing drug abuse in the community except occasional efforts being made by priests to preach against drug abuse. “Apart from sermon from the church I do not see any other avenue where such a thing takes place. The church is the only veritable means of telling people the bad effect of drugs” (PU6).
Leadership
Leaders and community members believe that preventing drug abuse may be a concern in the community.
Strength
The existence of elders and traditional rulers who serve as community leaders. Community leaders exist in the form of traditional rulers and elders locally called Onyishi. They make efforts to ensure peace and progress in the community.
Opportunities
Existence of vibrant community leaders who are interested in making their marks in the communities.
Weakness
The existence of community leaders who benefit from drug business, including those involved in the alcohol business. Also, there was no formal structure of leadership in Ubollo.
In Obukpa community, the traditional leader had an organized group whose job was to arrest individuals who engage in activities that disrupt the peace of the community. However there was no specific effort directed at preventing drug abuse in the community by the leaders.
In Ubollo there was no organized leadership structure at the time of this study. “…the separate units do not even have collective ties. There is no cordial relationship with community leader in the community PU6” However this community had religious leaders who from time to time speak against drug abuse.
Community Climate
Community members have been making little efforts at preventing drug abuse.
Strength
There were locally agreed forms of punishment for the drug abusers although this was not strictly enforced.
Weakness
Drug abusers and those doing drug business oppose community efforts to prevent drug abuse.
Opportunities
The communities are close to a tertiary institution within the zone. Human and material resources from the institution can be made use of to help the community prevent drug abuse.
Threats
Some community members who were involved in drug business or who have other conflict of interest try to subvert efforts at preventing abuse of substances.
In Obukpa, participants noted that while many members of the community will passively support prevention of drug abuse, those who benefit from drug abuse and those who abuse drugs will oppose drug abuse prevention efforts. A participant from Obukpa stated that fines are sometimes given to those involved in drug abuse.
Also in Ubollo a participant stated that sometimes the community members give punishments to those who engage in drug abuse. “…if you are caught smoking ‘Igbo’ (marijuana) especially a young person, the elders will organize and have you flogged very well. PU4).”
Knowledge of Issue
Community members have little knowledge about drug abuse prevention
Strength
The communities acknowledge that drug abuse is harmful to health and leads to social disruption, so there is a need to prevent it.
Weakness
Very few sources of information on the issue of preventing drug abuse in the communities.
Opportunities
Presence of secondary schools and churches in the two communities, these present good structures for drug abuse prevention efforts.
Threats
Poor electricity and internet facility to facilitate wider coverage in drug abuse prevention to increase awareness of dangers of drug abuse particularly among youths in the community.
Resources
There are limited resources that could be used for further efforts to address the issue.
Strength
Availability of physical resources for preventing drug abuse. Each community had one public secondary school with many private schools. The schools within the community provide very good channels for drug abuse prevention efforts.
Weakness
Very limited financial and human resources for preventing drug abuse.
Opportunities
Experts from the nearby higher institution can be engaged to assist in drug education programmes within the communities.
Threats
Inadequate professional and energetic workforces.
Participants from both communities indicated lack of financial resources for support of drug abuse prevention programmes. Many participants however reported availability of space and volunteers but there was total lack of grant funding, experts and very few financial donations for drug abuse prevention. Many young professionals from the communities reside in the cities in search of greener pasture, leaving mainly the retired and unskilled members of the communities living in the villages.
Discussion
Main Findings of the Study
The two communities were found to be at stage three on the CRM anchored scales, which is described as vague awareness stage. Therefore the communities were aware that drug abuse exist in their communities but they had no specific plans for preventing drug abuse and were not making any such plan. They did not see it as something worthy, to have efforts targeted specifically at preventing drug abuse in the community. Plested et al. (1999) in a study found that most rural communities are at relatively low stages of readiness. The result also revealed the communities’ stage of readiness across all the dimensions. Although the communities’ overall mean scores indicated that the two communities fall within the same level of vague awareness, it is important to note that at individual community level, the readiness level of the two communities varied for knowledge of issue dimensions (Table 3). In a similar study, Ehlers et al. (2020) found that a high proportion of adult (93%) and youth (96%) respondents were aware of one or more of the drug abuse prevention intervention activities in rural California. This shows that rural communities can differ in their level of readiness for drug abuse prevention and their awareness of drug abuse prevention efforts. Such differences may stem from differences in resources available to each community and means of disseminating information to community members. The two communities’ low level of readiness reinforces the need for an intervention that should be tailored to their level of readiness.
We used SWOT analysis to analyse the external factors (strengths and weaknesses) and internal factors (opportunities and threats) that are closely related to the various dimensions of community readiness for drug abuse prevention. On knowledge of effort, we identified the church as a means of preventing drug abuse in the two rural communities. This finding is consistent with previous studies which showed that rural churches and faith-based organizations can play important roles in promoting substance abuse prevention (Gale et al., 2012; Nieuwsma et al., 2014). Studies have equally shown that rural adolescents are more inclined to participate in organized church-related events and could benefit from activities focused on substance abuse prevention (Gale et al., 2012). The main threat to knowledge of effort identified by participants was poor media coverage and network service for effective dissemination of information. The overwhelming advantages of media such as mobile phones to disseminate health information to rural communities are well documented (Sokey et al., 2018). Addressing this threat will go a long way to enhance dissemination of information related to drug abuse prevention in rural communities.
On leadership, the main strength for both communities is the leadership role of the elders in the communities. This is consistent with the culture and tradition of many communities in Northern Igbo lands which give special recognition and respect to the elders (Nwagu et al., 2017). These elders can be very useful in correcting the ills in the communities and can serve as count measures targeting the identified weaknesses of no formal structure of leadership in Ubollo community.
Regarding community climate, the strength of the two communities’ was in the existence of agreed form of punishment for drug abusers. Although Punishment alone has been identified as a futile and ineffective response to drug abuse (Chandler et al., 2009), it is an evidence that the communities recognize the need to stop drug abuse in their communities. One weakness inherent in both communities is that drug abusers and those doing drug business oppose community efforts to prevent drug abuse. This apparently is as a result of the economic benefit they are making from drug business. Local security agency and national security agents should work hand in hand with community leaders and health personal to curb the excesses of this group of people in rural communities.
Community members had little knowledge of drug abuse prevention. The communities however acknowledged that drug abuse is harmful to health and can lead to disruption of social life and so there is need to prevent it. This can serve as a good starting point for increasing the communities’ knowledge of drug abuse prevention practices. The presence of churches and schools within the two communities presents good opportunities for reaching out to members of the community with intervention programmes for drug abuse prevention. Literature has shown that youths who participate in faith-based activities are less likely to use alcohol or begin using illicit drugs (Gale et al., 2012).
The communities had limited resources for drug abuse prevention. Each community however has a physical space where community members can gather. Such spaces are necessary for holding community or town hall meetings to raise awareness of the issue of preventing drug abuse (Rural Health Information Hub, 2018). Resources are vital to any health intervention programme’s success and they serve as potential indicator of future sustainability of the effort. There is need for state and local government intervention in order to get efforts in form of grants to help implement drug abuse prevention interventions in rural communities. Rural communities would benefit from enhanced media network, collaboration with experts from educational institution, national drug law enforcement agency, and national security agency to move them to a higher stage of readiness to address issues of drug abuse prevention in their communities.
In our study, the CRM interviews has helped project partners learn about the community and established relationships that will guide and facilitate an intervention that will increase the community’s capacity to generate both the demand for and a supply of community-relevant, preventive interventions. Participants were selected from various sectors of the community to ensure that the interest and needs of the various sectors of the community will be catered for in the intended intervention programme.
The qualitative feedback from the CRM interviews will help community health nurses and other drug education experts tailor interventions to increasing knowledge among the community members of specific tailored efforts that can help prevent drug abuse in the community.
Implications for Nursing Practice
The two rural communities we studied were at a low stage of readiness to prevent drug abuse in their communities. Nurses and other health personnel involved in Community Health education should therefore identify strategies to create awareness of the dangers of drug abuse in rural communities and raise communities’ members’ readiness level to prevent drug abuse in their communities. In working to raise readiness levels, community health nurses should identify creative ways to package their messages taking advantage of the opportunities within the communities and the strengths of the community, while working to deal with the weaknesses of the communities and with situations that threaten their readiness.
Oetting et al. (2014) observed that one-on-one meetings work well when readiness levels are low. The nurse should therefore make good use of opportunities that present themselves during patients’ visit to the rural health posts and nurses’ home visits to engage community members on discussions on preventing drug abuse one-on-one, bearing in mind, each client’s peculiar need. Apart from one-on-one interventions, community health nurses should also make use of traditional media that are readily available and accessible to community members in their drug abuse preventive efforts. Such media may include posters, billboards, TV and radio. Social media, such as Facebook and Twitter will equally be used, but the nurse should not rely solely on these social media as they may exclude the less privileged and the older members of the community.
The two rural communities in our study had locally agreed form of punishment for drug abusers. The community health nurse should therefore identify interventions which are socially, culturally, religiously, politically, and economically appropriate. Such interventions are more likely to be accepted by community members (Armenakis, 2007).
The church was identified as a viable means of disseminating information on drug abuse prevention in communities. Community health outreach to different groups in the church will assist the nurse in providing targeted health education to youths and women on the dangers of drug abuse. Involving Religious leaders in such health programmes can yield valuable health dividend
Apart from the religious leaders, the community health nurse should endeavour to seek out other opinion leaders and engage them as volunteers in drug abuse prevention effort since these individuals may have more influence on people's opinions, actions, and behaviors than the media. Opinion leaders can be beneficial in getting the attention of the audience. In addition, they continue to influence community members long after a specific programme is dismantled (Valente & Pumpuang, 2007).
Our findings showed that the two communities had inadequate professional and energetic workforces. The community health nurse should identify and collaborate with other health care professionals within and outside the community to ensure that all the necessary health care services are delivered to the communities. Those individuals and organizations that will participate directly in making decisions about drug abuse prevention projects and have roles to play in the interventions should be co-opted by the nurse. Such key individuals may include the staff of the Departments of Health and Education, members of the police force, community leaders, youth leaders, teachers, school counselors, parents, political figures, NGOs, etc.
Limitations
The study was limited to two rural communities in Enugu state Nigeria. The socioeconomic status of members of these communities may differ from that of other parts of Nigeria and hence generalization of the findings of this study should be done with caution. Also the small number of participants in this study limits the generalizability of the findings; nonetheless, the findings provide direction for future projects.
Conclusion
Rural communities are vulnerable to drug related problems as a result of low level of awareness of the dangers of drug abuse. This study therefore verifies the importance of the CRM which was developed to help in measuring a community’s readiness levels on several dimensions that will help diagnose where efforts are needed. We have also been able to identify the communities’ weaknesses and strengths, as well as the obstacles and threats we are likely to meet as we move forward intervening in the two communities. The findings of this study will therefore be very useful in developing an intervention programme of drug abuse prevention in the area of study.
Footnotes
Acknowledgments
The authors would like to acknowledge the community leaders who provided enabling environments for the study. We equally appreciate all the participants who gave up their valuable time to take part in the qualitative interviews.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Tertiary Education Trust Fund (TETFund) Institution Based Research (IBR) grant (TETFUND/DESS/UNN/NSUKKA/RP/VOL.X).