
Abstract
Inadequacy in discharge planning, preparation of readiness, and unplanned readmissions are closely linked and could cause misutilization of hospital services, creating higher costs to the health-care system. The information given before discharge is vital and of great importance for the well-being of the patient. The study’s objective was to describe the patient’s experience of their discharge process. A descriptive study was designed. Fifteen (n = 15) interviews with patients at one University Swedish hospital were held, and a qualitative content analysis was made from the collected data. The results show that accessibility, information, communication, confidence, and participation are pivotal in future development in the discharge process. The findings of this study indicate that in affirmation with the patient’s experiences and desires, there is a great urgency for improvement in the discharge process. There is a need to focus on information and communication at discharge by initiating interaction from the nurses together with the doctors at a specific time in the discharge process. The discharge process needs to be more individualized and person-centered which could lead to better patient governance. Both accessibility and continuity need to be improved. The information given needs to be met with the patient’s level of understanding.
Introduction
This study examines the discharge process of a Swedish health-care system at a university hospital in the south of Sweden. It is imperative to improve this process because if it is not improved it can lead to further utilization of hospital services, giving rise to higher costs within the health-care system (Hesselink, Schoonhoven, Plas, Wollersheim, & Vernooij-Dassen, 2013; Jones et al., 2016; Karlsson Krohwinkel & Winberg, 2012; Stockwell-Smith et al., 2018). Jencks, Williams, and Coleman (2009) reported that unplanned readmissions and lack of readiness of patients at discharge are closely linked. In some cases, when the patient’s needs are not met at time of discharge, it can lead to an early increased number of untimely readmissions after discharge (Flink, 2014; Jencks et al., 2009; Karlsson Krohwinkel & Winberg, 2012; Leppin, Gionfriddo, & Kessler, 2014; Ragavan, Svec, & Shieh, 2017). Twenty percent of patients are readmitted within 3 weeks of discharge; suffering either from adverse drug events or other effects of their illness which lead to severe comorbidities (Forster, Murff, Peterson, Gandhi, & Bates, 2003; Hesselink et al., 2013). To work proactively with the patient and to optimize the discharge process, it is important to gain an understanding and knowledge of how the patient experiences the discharge process and their involvement in the process. Patient involvement in health care is highlighted in the recent revision of the Patient Act in Sweden (Swedish Code of Statutes, 2017). The purpose of the law is to create a better balance of patient-empowerment between patients and staff, thereby enhancing patients’ influence over their own health care. Published studies on patient involvement have also shown that patient involvement in their health care is a high priority, and patients’ lack of determination and autonomy lead to major challenges (Elwyn & Miron-Shatz, 2010; Ijäs-Kallio, Ruusuvuori, & Peräkylä, 2010; Siouta, Hellström Muhli, Fossum, & Karlgren, 2017). This study concerning the topic of the discharge process is relevant in today’s fast pace turnover of hospital patients where patient involvement is becoming more and more central to the health policy and practice. The aim of this study is to analyze and describe how patients describe their experiences and participation in the discharge process. These descriptions are understood as a meaning-making activity embodied in the patient’s experience and understanding (including events, actions, roles or identities, knowledge claims, and communication).
Background
Verhaegh et al. (2014) showed that nearly a fifth of the patients discharged in the United States are rehospitalized within 30 days and almost half of these admissions could have been prevented if the discharge process was better developed. The costs of untimely readmissions are high, and readmissions are greatly increased (Friedman & Basu, 2004; Jencks, Williams & Coleman, 2009; Verhaegh et al., 2014). The discharge process is about listening to the patient and taking consideration of the patient’s understanding of the information. Besides, it is the responsibility of the care provider to communicate in ways that are understandable to the patient, thus contributing to their rehabilitation (Fong & Longnecker, 2010; Kriplani &Weiss, 2006). From a holistic point of view, a good patient discharge process ensures that there is a coherent care chain; links between the hospital and the municipality need to be established and maintained. Many of the problems could be prevented by giving a better handover. The quality of handovers is a challenge for everyone involved, including the hospital, the municipality, and primary care; especially in relation to the aging population, for example, multisick and chronically ill patients (Flink, 2014; Hesselink et al., 2013). However, there is a communicative gap between the involved parties, a gap that should be curtailed (Hesselink et al., 2014). In the Swedish context, a medical reconciliation and medication list have been obligatory before discharge since 2012 (Socialstyrelsen [National Board of Health and Welfare], 2015). The medical reconciliation sheet includes the patient’s medical history stating the reasons for admission, preparation, drug dosage, as well as information regarding treatment plans, monitoring methods, and discharge criteria. This implementation of the medical reconciliation sheet was revolutionary to the Swedish health system resulting in an improved structural discharge process, minimized drug-related readmissions, which ultimately increased and improved patient safety both inside the hospital and in primary care. This process was initiated by the Swedish Health department. Improvements were observed relating to the 30-day readmissions which was one of the reasons this process was implemented (due to increasing health-care costs; Socialstyrelsen [National Board of Health and Welfare], 2015). Dialogue as opposed to monologue became very much in focus for all medical personnel, educational opportunities were provided, and projects were imminent and set up inside the hospital settings with established links to the community and primary care. Communicating with the municipality and performing safer handovers for the patient discharge were the essence handovers consisting of patient medical reconciliation summaries and an updated medicine list. The reconciliation process was initiated in an emergency department at a university hospital in the south of Sweden, which was implemented both on patient admission and discharge. The medical reconciliation sheet later became a safety tool, one of many, to improve patient safety which subsequently won a national prize for patient safety in 2011. The reconciliation sheet helped in reducing polypharmacy, drug prescription duplication, as well as confusion and disorientation in the older adults. Confusion and disorientation in the older adults was improved by restricting benzodiazepines, anticholinergics, and opioid products. What has been recently initiated is a pharmacist in the departments securing the medical reconciliation sheets even more. This was a topic of interest in 2011 while forming the safety toolbox to improve patient safety, but the idea did not appeal to the physicians at that time.
Furthermore, organizational factors may also be a contributing factor to an inefficient discharge process, for example, lack of time, an urgent need of other patients to be dealt with, shift work forcing medical staff to discharge patients before doing an accurate assessment of their health problems as well as staff not knowing the patient well enough, and above all, the high percentage of patient turnover in the emergency departments (Hesselink et al., 2013).
From a holistic view, the discharge process determines the future of the patient’s health (Hesselink et al., 2013; Hunter, Nelson, & Birmingham, 2013; Laugaland, Aase, & Waring, 2014). Therefore, it is necessary to assess the discharge process to enable good health and disease prevention (Hesselink et al., 2014; Laugaland et al., 2014). Communication and the information given before discharge are vital and of great importance to the well-being of the patient. Dialogue should be based on open communication where the patient feels respected (Linell, 2014; Tamura-Lis, 2013; Tobiano, Chaboyer, Teasdale, Raleigh, & Manias, 2019). The theoretical basic principles of interactive communication, such as face to face correspondence, enabled a positive interaction and agreement (Linell, 2014). Pawar (2005) maintained that to achieve compliance, it is necessary to create a trusting relationship with the patient. The information should be given both verbally and in writing to the patient before discharge (Böttiger, 2005; Mc Larnon, Walsh, & Ni Shuilleabhain, 2016). In accordance with the Swedish health-care system, health-care providers are obliged by law to ensure that the patient has understood the information given at hospital discharge by having a dialogue with the patient (Swedish Code of Statutes, 2017). However, many studies have shown that there are shortcomings in the discharge process regarding communication with and information provided to patients (Hesselink et al., 2014; Muhli, Trost, & Siouta, 2019; Popejoy, Moylan, & Galambos, 2009; Siouta, Hellström Muhli, Fossum, & Karlgren, 2017).
Methods
A qualitative approach was chosen for this study, and an inductive latent content analysis per Elo and Kyngäs(2008) was used. The data were collected through semistructured interviews, manifesting the patient’s experiences of the discharge process. The interview questions were based on both open and follow-up questions. During the period of March to June 2015, 15 patients were strategically selected by M. K. the first author. A review of all hospitalized patients in a medical emergency department, at a university hospital in the south of Sweden, was carried out with the intention of achieving a variety of data based on gender, age, and education (Polit & Beck, 2017). The criteria for inclusion were respondents from both genders between the ages of 50 to 85 years, including the following diagnoses: pneumonia, atrial fibrillation, central chest pain, and chronic obstructive pulmonary disease (COPD; see Table 1). The patients’ characteristics are described in Table 1. The exclusion criteria included patients who could not speak or understand Swedish had cancer or lacked cognitive ability. Ethical approval was obtained from the Regional Ethics Committee in Stockholm, Sweden (Dnr: 2015/6239).
Demographic data and patient characteristics (n = 15).

Note. CBS = central chest pain; COPD = chronic obstructive pulmonary disease; AF = atrial fibrillation.
Each patient was informed of the study’s purpose both verbally and in writing. The patients were interviewed 24 to 72 hours after discharge. The interviewer (M. K.) explained the study in more detail before the interview and answered questions about the study. All interviews took place at a time and place chosen by the patient either in their home or in the hospital. The interview time ranged from 30 to 45 minutes and was recorded digitally. Fifteen interviews were carried out by the same interviewer, whereby seven of them were conducted in the patient’s home, one by telephone, and the remaining seven in a locality within the hospital. The impact of meeting with the patient face to face gave a better response compared with a telephone interview. The telephone interview limited the interviewer’s scope of impact due to a hearing ailment. The theoretical basic principles of interactive communication, such as face to face, and a two-way information sharing, enabled a positive interaction and agreement with the patient (Linell, 2014; Pawar, 2005; Tobiano et al., 2019).
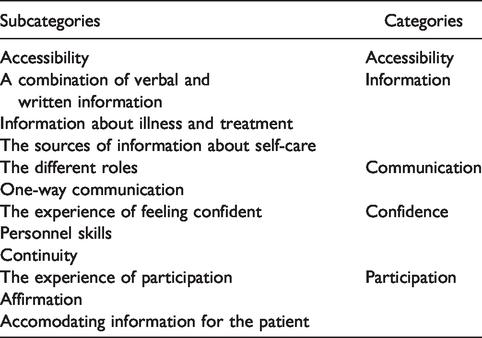
For the interview analysis, all 15 interviews were transcribed verbatim. The transcribed interviews were read straight through and were checked for exactness by the interviewer. Second, the transcripts were read several times, searching for statements describing experiences related to the study’s aim. A total of 147 identified meaning units were found regarding the patients’ experiences of the discharge process. The meaning units were then abstracted into shorter sentences. The sentences from the transcripts that shared the same meaning were condensed and coded. The codes were then transferred to a coding page, where similar codes were grouped together thereby comparing their differences and similarities. From these differences and similarities, the subcategories and main categories were created (Table 2). To increase the credibility of the analysis process (Polit & Beck, 2017), the analysis was discussed between all authors together by comparing content differences and similarities between the codes, subcategories, and main categories.
Findings.
Results
The results of the patients’ experiences of the discharge process are reported in 5 main categories and 12 subcategories. The main results are summarized in Table 2. Relevant excerpts describing patients’ perceptions are presented next to illustrate the categories.
Accessibility
The patients experienced a lack of accessibility in different ways; they expressed concerns about the hospital’s stressful environment especially in relation to the hospital staff; they were “always on the go.” The doctors did not have time to linger on to answer the patient’s questions. If I could only talk as a patient to the doctor and nurse … and not a whole ward full of other patients and people running here and there … You need to understand, one is not given a chance, no chance to ask questions and wait for answers … What will I do … ? I am thinking, I can do absolutely nothing. (P. 5) If you were given a number to an answering machine or something similar, one could call for a specific period after being in hospital … instead of going to the hospital … just to be able to make a telephone call. (P. 3)
Information
The patients’ experiences of information manifested into three subcategories: a combination of verbal and written information, information regarding illness and treatment, and finally, information about self-care.
A combination of verbal and written information
Many of the patients’ experiences of written information were positive; it complemented their verbal discharge information. They mentioned with delight how they had received both verbal and written information. I received both verbal and written information and really appreciated it. (P. 7)
The information about illness and treatment
The patient did not want to be sent home without being given further information about their illness and eventual side effects and also information about future investigations. Furthermore, it was important to have their medication list reviewed as well as receiving a medical reconciliation. The patients experienced a lack of information regarding their illness and treatment given before discharge; for example, regarding an anticoagulant medication. So, if they eliminate my Fragmin injection, then there should be a small lecture or a major lesson as to why. (P. 14).
The sources of information about self-care
It emerged from the interviews that the patients were actively pursuing information due to their interest in their own health. That information included, brochures being available in the waiting rooms and corridors of the hospital relating to health and illness issues. An 80-year-old patient with COPD said that she chatted with other COPD patients online from the Netherlands and Germany and that the exchange of information was both useful and stimulating. The patient also said that it inspired her to motivate herself and set up goals for different activities. Yes! You know, I have oxygen continuously over 24 hours …, and this coming May it will be a total of seven years. So, I have done relatively well, which I can attribute, then again others could say differently because I motivate myself. I think that is important that one should keep active. (P. 5)
Communication
The different roles
It was discovered the nurse did not participate in the discharge process at the emergency department. However, in specialized areas such as cardiology, the patient meets with a nurse as well as the doctor before discharge. However, the role of the doctor and the nurse was perceived differently in both contexts. It emerged from the patient’s interviews that it was the doctor who managed the discharge process. Yes, yes, she (the doctor) spoke a language there one could have a dialogue, huh, and what I asked, I got an answer. So, it was no problem, I thought she was good, now I don’t remember her name, but she was very accurate, as to say. (P. 6) Nurses, yes the nurses distribute our medication, No, they don’t say very much. (P. 8)
A one-way communication
The discharge process was experienced as a one-way conversation, which meant that the patients did not feel like a participant in the discharge process. Several patients experienced a one-way communication, for instance, where the doctor was talking too fast. He talked so fast, he did really. Just as well I asked a lot of questions myself, so it is. (P. 12)
Confidence
It emerged from the interviews that trust and confidence were important for the patients’ feeling of autonomy. Feeling confident was perceived differently and could be associated with the experience of nursing staff’s skills and in the patient’s continuity of care.
The experience of feeling confident
It became apparent from the discharge process that feeling confident and supported by the hospital staff were important for the patients, and that there was an acceptance and knowledge of the patient’s condition and their vulnerabilities. Patients wanted to feel confident, both on admission to the hospital and after their discharge. To feel confident is a prerequisite for good health, as one patient put it. The patient should feel confident when leaving the hospital. There are many questions; it doesn’t take much to feel safe, to be accepted, to be acknowledged. It only takes 5–10 minutes. Not this, with the patient lying down and the doctor standing over you. It requires two grown adults to sit down. (P. 13)
Personnel skills
The personnel’s competency skills played a part in the patient’s feeling of being confident. However, the competency skills were perceived differently depending on whom the patient met. However, it is so very different depending on who, some seem very secure and others seem to be very new, the experience was that many nurses had a variety of skills. (P. 7)
Continuity
It also emerged that there was a desire for continuity of care which was perceived as being cared for. Repeating their entire medical history all the time was tiring for the patients. I sincerely hope that I get a permanent doctor at the Healthcare Clinic. It makes it easier to talk because you don’t have to repeat yourself at every visit. It’s so tedious. (P. 4) It’s not the doctors who have the continuity with the patient before discharge, it’s the nurses. Well, what I mean the doctor comes in … yes, this sounds very mean, but all the doctor does is adds his signature so that I can be released home. What I mean by this is that it is the nurses who play the important part, that’s what I think. (P. 5)
Participation
Participation transpired through the patient’s own experience of being a participant or a nonparticipant by being confirmed or not being acknowledged in dialogue.
The experience of participation
The predominant experience of participation was the lack of it. For instance, the lack of participation was experienced when the doctor talked to the patient’s relative before talking to her regarding her treatment and discharge from the hospital. Furthermore, to call the patient, “the COPD case” was not considered respectful or polite. However, sometimes the patient felt that the doctors did have a good bedside approach. On the other hand, when talking to doctor x “for example, you felt like you wanted to sit and talk.” (P. 10)
Affirmation
To engage the patient in conversation made the patient feel involved and was considered an excellent prerequisite for promoting good health. That someone cared and that one feels important and I have confidence in her are some of the expressions that emerged from the analysis. There I was taken care of, because when I came back there afterward and … the whole ward! Oh, hello! … how I felt so important. (P. 8)
Accommodating information for the patient
The experience of a hospital discharge stressed the importance of the patient being met at their own level of understanding. Occasionally, the patients do receive a satisfactory level of information. I have experienced it a few times now, where they really do care and explain exactly what happened. (P. 14) It is up to the doctor to explain so people can understand … Generally speaking, it is all about how you say it so that the patient understands. (P. 10)
Discussion
The study’s objective was to describe the patient’s experience of the discharge process and by using this background for discussion for future developments in the discharge process in preventing early and untimely readmission. The results revealed that the inclusion of patients in the discharge process is vital but unfortunately, insufficiently met; a result that was even shown in the Hesselink et al.’s (2014) and Eldh’s(2006) studies. In this study, what the patients meant, was that the doctors did not have enough time to spend with the patients because the hospital’s environment was too stressful. This coincides with Hesselink et al.’s (2013) results, claiming that organizational factors may be contributing to an inefficient discharge process. This could be an accurate account in view of the shortcomings in the health-care’s continuity of care, to which the patients refer to. According to Hesselink et al.’s (2014) study, patients, or their caregivers, should participate in the discharge process and be aware of their health status and treatment. Assessment by hospital staff whether the discharge information is accurate and understood by patients and the municipality are important aspects to overcome the identification barrier for an efficient and effective discharge (Hesselink et al., 2014). The discharge process would be much better if the patient met with a doctor, nurse, or care provider who knew the patient and their medical history and background. Patients described misperceptions regarding information and communication before discharge; a monologue from the doctors was considered insensitive and disrespectful at a time when the patients did not feel receptive to information. The patients did not feel confident or “seen and heard.” Thus, the dialogue is not based on an open communication where the patient feels respected and did not give grounds for a positive interaction, trust, and mutual agreement before discharge as Tamura-Lis (2013), Linell (2014), and Tobiano et al. (2019) emphasized. According to Pawar (2005), a lack of trust decreases the possibility to achieve compliance regarding the doctor’s recommendation to treatment.
The patient emphasized that the information given should be accommodated to the patient’s level of understanding. It was also the patient’s desire, that the doctors should be more effective in their listening and that they checked the patient’s understanding of information given. Both Linell (2014) and Tobiano et al. (2019) agree on these points. The patient’s understanding of information is pivotal for the effectiveness of the discharge process. This study shows that verbal information given could be better accommodated to the patient’s ability to understand. This is a very important point as knowledge is power; it gives assurance, strengthens, and empowers the patient in their self-care (Larsson, Rahle Hasselbalch, Palm, & Nylander, 2008). Furthermore, according to Lagerdahl (2008), patients want to be involved in their own self-care, “its my body and I take care of it twenty-four hours, every day. So, I can take control over my health and my life.” (P. 16). In this study, it became evident because patients actively sought information.
However, the role of the doctor and the nurse was perceived differently in both contexts. It emerged from the patients’ interviews that it was the doctor who managed the discharge process and that the doctor’s role was clearly defined. The role of the nurse was perceived as being more ambiguous. This finding contradicts another finding, namely, that the doctors were perceived as the expert and that it was the nurse who had full control of the situation and was competent and confident in his or her role as a nurse. Although the study’s material is limited in scope, it speaks for a clarification in the heath-care staffs’ role to enable the utilization of the various professionals’ skills in a more optimized manner.
Implications for Practice
The pedagogical implications have to do with establishing and implementing nurses’ awareness in enhancing person-centered communication with patients in the discharge process. One aim for future research is to explore how nurses experienced patient involvement in the discharge process as well as how they promoted involvement and communicated with these patients.
Study Limitations
A descriptive qualitative design was used, not a statistically representative sample. Thus, all quantifications of the results were missing in this type of research study. An adequate number of patients were selected to achieve a high value of the findings in terms of qualitative analysis. The usefulness of our qualitative analysis is in what patients said (not how many held a similar view) and how they derived their observations about the discharge process. The use of interviews with a clinical sample (Table 1) and qualitative content analysis reveals new relevant aspects of patient perceptions and experiences in the discharge process. Only 15 patients were interviewed, and all of them were from one hospital. Their biases or world views are likely to be similar. The patients in the sample were strategically selected for strengthening the study and were of both genders, we believe that the value of the information in the findings is high. The transferability of the results might be an emphasis on the concept of patient involvement in the discharge process.
Conclusion
There is obviously a great need to improve the discharge process regarding the patient’s experiences and desires. The discharge process needs to be more individualized and person-centered. Both accessibility and continuity need to be improved. Patients described misperceptions regarding information and communication before discharge. The information given needs to be modified and met with the patient’s level of understanding. According to the patients, the doctor’s role in the discharge process was clearly defined, but the role of the nurse was perceived as being more ambiguous. The doctors were perceived as the expert by the patients and that it was the nurse who had full control of the situation and was competent and confident in his or her role as a nurse. There is a need to focus on information and communication at discharge by initiating interaction from the nurses together with the doctors at a specific time in the discharge process. Furthermore, communicating with the municipality in providing a good and safe handover is pivotal to patient safety, that is, updated medication reconciliation sheet and medication list to prevent untimely readmissions and drug errors. All measures that are applied and taken in the reconciliation are to ensure a better communication and dialogue between the patient and the health-care staff as the information handover between the various health-care providers is to improve the patients’ adherence to their medication and above all prevent errors in their prescribed drug medication.
Contribution of the Paper
What Is Already Known About the Topic?
The costs of untimely readmissions are high and increasing; however, most of the admissions can be prevented if the discharge process is better developed. Drug-related incidents are related to 30-day readmissions. Interactive communication, respectful listening to the patient, and quality of the information given, written and verbal, before discharge are of great importance for a successful discharge process. It is of great importance to ensure that there is a coherent care chain; links between the hospital and the municipality. Many hospital organizational factors may be contributing factors to an inefficient discharge process, for example, lack of time from personnel and an urgent need of other patients.
What This Paper Adds
The patients’ feeling of security is of great importance. Continuity in the discharge process and availability, being able to call the hospital department after discharge, give a feeling of security and safety. The importance of a medical reconciliation sheet and updated medication list. Improvement in communication and interaction.
Footnotes
Acknowledgments
The authors sincerely thank the interviewed patients. The authors are also grateful to Associate Professor Ulf Olsson, Stockholm University, Sweden and David Lynch, London for the help with the reading of the manuscript.
Ethical Approval
Ethical approval was obtained from the Regional Ethics Committee in Stockholm, Sweden (Dnr: 2015/6239).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.