
Abstract
Introduction
Young, minority women are less likely to follow recommendations to prevent infant sleep-related deaths putting their children at risk. This study extended the past pre/post study designs to an RCT design and included both parent report and objective observation of the sleep environment.
Objective
This study focused on this population in a quantitative, randomized controlled trial using a low-cost, brief educational intervention, a Safety Baby Shower (SBS).
Methods
Pregnant teens aged 13–19 (N = 147) were recruited as a dyad with a senior female caregiver and randomized to intervention or control groups.
Results
Comparing self-report, safe sleep knowledge, attitudes, beliefs, and intent (KABI) to act scores across the two groups found intervention dyads to have more positive views on all four constructs than controls. Specifically, intervention dyad young mothers were significantly more likely to have positive beliefs about safe sleep and were more likely to report intent to practice infant safe sleep than control young mothers. Intervention dyad young mothers also had higher self-efficacy related to infant safety and more positive attitudes about safe sleep practices than control young mothers. Observations at a home visit conducted after delivery found no differences in the safe sleep practices by intervention status. Participant report of behaviors at the home visit also showed no differences in the use of safe position between the intervention and control groups.
Conclusion
It appears that even when young mothers gain knowledge and self-efficacy, they have difficulty implementing this knowledge. In practice, this suggests that exploring barriers prenatally with this population and offering suggestions to overcome them may be indicated.
Introduction/Background
Sudden Infant Death Syndrome (SIDS) and suffocation account for more than 65% of all Sudden Unexpected Infant Deaths (SUID) and represent the third leading cause of post neonatal infant death (death in an infant aged 28 days to 1 year) in the United States (Carlin & Moon, 2017). The pathophysiology of SIDS is not fully understood. The Triple Risk model represents SIDS as the result of an intersection between a period of critical newborn development during the first months of life, underlying and often invisible vulnerability in the infant, and external stressors and triggers including sleep position and environment (Filiano & Kinney, 1994). Infants who succumb to SUID are thought to be unable to respond and protect themselves to challenges in the environment, including known risk factors such as nonsupine sleep position and an unfavorable sleep environment (Bombard et al., 2018). Proposed underlying mechanisms for infant vulnerability to SUID include genetically determined developmental issues, delays in maturity of arousal mechanisms, or abnormalities in autonomic, neurologic, or cardiac function (Moon et al., 2011). Interventions to prevent SUID have focused on reducing risk factors in the sleep environment, with recommendations ranging from supine sleep position, avoidance of co-sleeping, and modifications to the sleep environment including a firm sleep surface and avoidance of soft objects in the crib (Hwang, 2021; Hwang et al., 2018; Maged & Rizzolo, 2018).
Review of Literature
Substantial disparities in the incidence of SUID exist, with higher rates noted among the infants of adolescent and minority-race mothers. Some of these disparities may be related to differences in sleep-related practices of these young mothers. For example, the National Infant Sleep Position Study and other studies show that teen mothers are less likely to adhere to safe sleep recommendations (Ostfeld et al., 2017; Willinger et al., 2003). Specifically, teens place their infants in the prone position rather than back more often than mothers over 19 years (Colson et al., 2009). Teen mothers are also less likely to bed their infants on an appropriate sleep surface (e.g., crib, portable crib, or play yard) than older mothers (Caraballo et al., 2016; Hirai et al., 2019). African-American women in general are less likely to use key safe sleep practices such as back sleep position, room sharing, and safe sleep surfaces (Hirai et al., 2019). A 2018 study by the Centers for Disease Control and Prevention (CDC) of safe sleep trends by characteristics of the mother indicated the priority groups for culturally appropriate interventions were younger, less educated, and racial minorities (Bombard et al., 2018).
Interventions have been effective in reducing SIDS in general and in some high-risk groups such as teen minority women. For example, an educational intervention delivered to small groups of Black parents was associated with self-reported safe sleep practices that were sustained through 6 months of life (Moon et al., 2004). Other studies in childcare settings and in intensive home visitation programs have been found effective in addressing some associated risk factors for SIDS (Moon et al., 2004; Moon et al., 2008). While these programs are effective, their intensive nature means that they are also very costly. A recent systematic review of the literature emphasized the heterogeneity of the existing evidence, need for theoretically grounded models, and called for additional research (Ellis et al., 2021).
This study examined the usefulness of a brief 2-hour educational intervention. The intervention, Safety Baby Shower (SBS), uses engaging activities to educate participants on infant safety topics, and is based on a Consumer Product Safety Commission program developed to promote home safety products. SBS has been shown to improve parent knowledge of some home hazards and improve use of safety products (Ahlers-Schmidt et al., 2020; Sanguino et al., 2010). For this intervention, the SBS was tailored to focus on the most common preventable causes of death in the first year of life, including safe sleep, motor vehicle safety, and prevention of abusive head trauma. The event simulates a typical baby shower with themed decorations, games to reinforce educational messages, and refreshments providing a relaxed atmosphere for both didactic and experiential teaching methods. Materials include visual aids, printed materials, and use illustrations and pictures at upper elementary reading levels. Participants receive safety products such as child safety seats, sleep sacks, pack-and-plays, and smoke alarms as their “shower gifts” with education on appropriate use of the products (Aitken et al., 2020).
Grounded in the Theory of Reasoned Action, SBS incorporates recognition that health decision making is based on a complex interplay of knowledge, attitudes, and beliefs, both personal and normative, related to intent to change behavior and the action itself (Ajzen & Fishbein, 1980). This theoretical approach has been used to support interventions for numerous health behaviors, including injury prevention (e.g., seat belt use), physical activity, substance use, and sexual health, and provides insight into what we believe are key mediators of teen mothers’ decisions about safe sleep (Cha et al., 2007; Hunt & Gross, 2009; Kakefuda et al., 2008; Martin & Newman, 1990; Morrison et al., 1998; Morrison et al., 2002; Morrison et al., 2010; Savage & Clarke, 1996; Thuen & Rise, 1994; Trost et al., 2002).
The transition from teen to adult is characterized by more active involvement by the teen in decision making (Steinberg, 1990). Attitudes about sleep position are more strongly associated with appropriate behaviors than knowledge (Chung-Park, 2012). For example, a mother's beliefs about choking risks have been found to be significant determinants of supine sleep positions.
The goal of this study was to examine the usefulness of the SBS intervention. The objective was to assess the change in attitudes and behavior post intervention for key safe sleep constructs: attitudes, beliefs, self-efficacy, and intentions. Further, differences in attitudes and behaviors were examined between treatment groups.
Methods
Research Questions
Did attitudes, beliefs, self-efficacy, and intentions and behaviors become more appropriate for safe sleep post intervention?
Did teen mothers that received the intervention demonstrate more appropriate safe sleep attitudes, beliefs, self-efficacy, and intentions and behaviors than mothers that did not receive intervention.
Design, Sample, and Inclusion Criteria
The study was a randomized controlled trial assessing the impact of an SBS intervention on self-reported beliefs about infant sleep and observation of behavior in the home. Inclusion criteria were pregnant teens aged 13–19, in the second or third trimester (13–28 weeks) of pregnancy, and residing within three target counties in central Arkansas (Figure 1; Table 1). Further, teens (TM) were required to be in their first pregnancy, and to identify a significant female caregiver at least 30 years of age. Finally, recruitment must have been timed to allow the teen and her senior caregiver to attend the educational intervention before the birth of her child. All data collection and intervention occurred between January 2016 and March 2019.
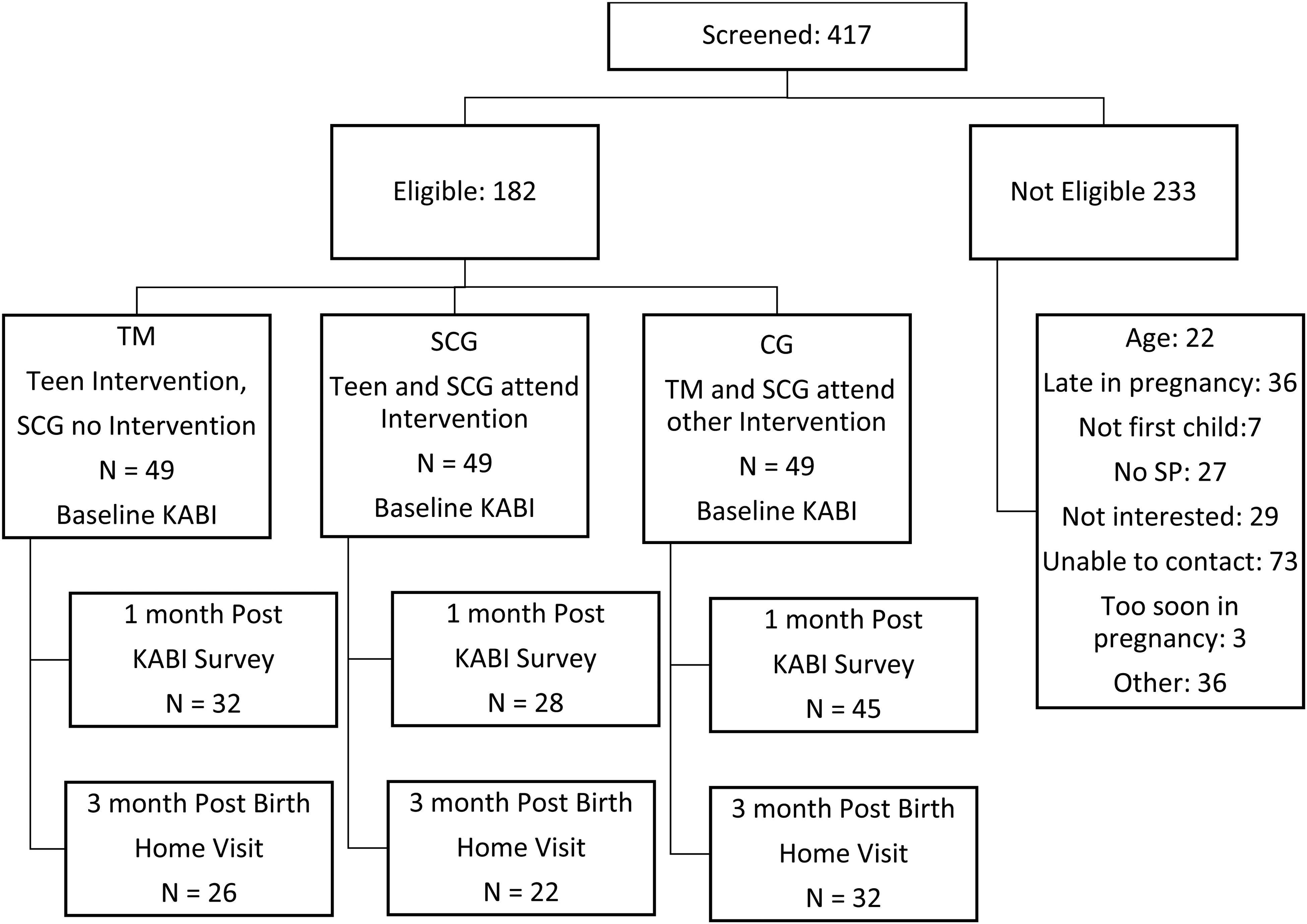
Study flowchart.
Demographics of the Participants at Baseline by Study Group.
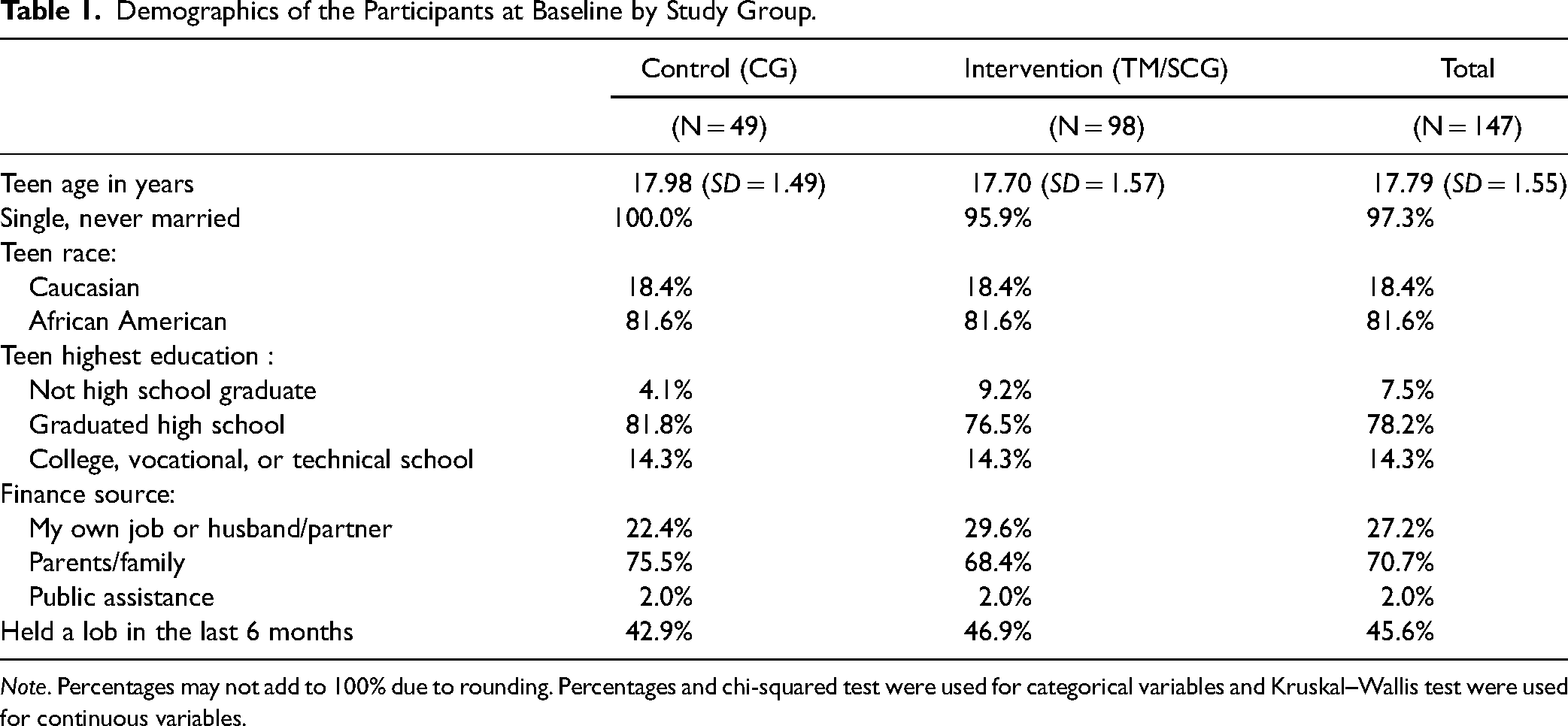
Note. Percentages may not add to 100% due to rounding. Percentages and chi-squared test were used for categorical variables and Kruskal–Wallis test were used for continuous variables.
Procedures and Institutional Review Board Approval
After approval from the local university institutional review board, recruitment began with outreach to community partners and through social media. The full study protocol is described elsewhere (Aitken et al., 2020). Recruitment sites included obstetrical practices, local health departments, home visiting programs, and health educators in hospitals, clinics, and community providers serving young at-risk families. The community partners provided potential participants with information about the study and directed them to study staff (in person or by phone) who administered screening questions to determine the eligibility of both members of the dyad. Dyads that screened as eligible and interested were invited to a brief interest session. The in-person interest sessions were scheduled near the time the teen entered her third trimester of pregnancy. At the interest session, full study details were provided, and dyads electing to participate underwent informed consent.
After enrollment, all participants completed a baseline assessment using REDCap (Harris et al., 2019; Harris et al., 2009). Following completion of the baseline measurements, participants were randomized using a permuted block scheme in a 1:1:1 allocation using the REDCap randomization module (Harris et al., 2019; Harris et al., 2009). All groups consisted of dyads and were randomized into one of the three study groups: Teen Mother only (TM), Teen Mother accompanied by Senior Caregiver (SCG), and Control Group (CG). The TM and SCG groups attended SBS sessions focused on safe sleep. Control dyads were provided with written safe sleep and other infant safety information (standard of care). All three groups attended a follow-up session focused on motor vehicle safety and car seat installation during which a follow-up knowledge, attitudes, beliefs, and intents (KABI) REDCap surveys of safe sleep were administered. In addition, a home visit was conducted approximately 3 months after birth of the target child, during which safe sleep practices were reported by the teen and observed by research staff who was blind to randomization scheme.
Measures
Baseline surveys included sociodemographic information, and an assessment of child development, and safety KABI took about an hour to complete. The KABI assessment was repeated 1 month after the educational intervention at an in-person car seat assessment. The KABI assessment included attitudes (three items, e.g., “Sleeping in the same bed with my baby lets me bond with my baby”), beliefs (four items, e.g., “Putting my baby to sleep on his/her back will make me feel good about his/her safety”), self-efficacy (three items, e.g., “I can’t stop others from smoking in my home”), and intent to act (four items, e.g., “I plan to tell everyone who takes care of my baby about the safest way for my baby to sleep”). Response options were Strongly Disagree (1) to Strongly Agree (5) and summary scores were computed as the mean of the items with higher scores indicating more positive views.
Standardized observations were obtained during a 2-hour home visit and included a parent survey of self-report safe sleep practices and observation of the infant's sleep safety environment. A valid survey assessed key American Academy of Pediatrics (AAP) recommendations but this study focused on (a) supine sleep position, (b) firm sleep surface, (c) separate sleep location and room sharing, and (d) bedding safety—soft or loose bedding (Whiteside-Mansell et al., 2017). A standardized introduction asked the parent to consider how she and others put the baby to sleep. For this study, we report on the 14 survey questions (Table 2) that assess four of the AAP recommendations related to sleep practices. Most questions had a response option on a 4-point Likert scale of “Every Time”, “Most of the Time”, “Some of the Time”, or “Never” (e.g., How often do you put your baby down to sleep in an adult bed?). Respondents also were asked to select from a list of options (e.g., select the sleep location used most often). Finally, one question allowed a yes/no/don’t know response (e.g., Do you think the mattress in the crib is firm?).
Safety Knowledge, Attitudes, Beliefs, and Intents (KABI): ANOVA Comparison of TM/SCG and CG Groups with Mean (SD).

Note. aMeans range from 1 to 5, all analyses are controlled for teen mother's race. CG = Control Group; SCG = Senior Care Giver; TM = Teen Mother Only.
**p < .001.
The observational assessment was developed to match the target of the AAP recommendations. Research staff was trained to assure adherence to the protocol. The assessment included a standardized script and request to be shown the baby's sleep area. In the sleep area, the parent could choose to demonstrate baby's normal sleep location either with their own child or a doll that resembled their baby. The observer completed a detailed examination of the sleep location (e.g., crib). Examining the contents of the indicated sleep area (e.g., blanket, bumper pad, and pillow), items near the sleep environment (e.g., cords and heaters), and the type of sleep area (e.g., adult bed, couch, floor, and crib). The sleep surface (e.g., firm and sheet tight) was noted and a safety assessment was conducted for cribs, pack-n-plays, and bassinets (e.g., broken/missing parts, production date, and crib slat width).
Statistical Analysis
We conducted nonparametric tests to examine pre–post assessments and bivariate comparisons. Surveys included safe sleep constructs: attitudes (three items), beliefs (four items), self-efficacy (three items), and intentions (four items). Data management were performed using the statistical software package R and SPSS (IBM Corp, 2019; R Core Team, 2013).
Results
Sample Characteristics
We recruited and enrolled 147 pregnant teens (13–19 years old) and their significant female caregivers. As shown in Figure 1, 105 teens completed the follow-up KABI survey assessment and 80 teens completed the final home visit. Given the small sample sizes for the intervention groups, TM and SCG were combined as shown in Table 1 (i.e., CG vs. TM/SCG). Preliminary analyses examined randomization assumptions. Demographic characteristics were similar across the TM/SCG and CG at baseline. Teens were 18 years (+/−1.5 years) and most were black (White, 18%, Black 79%, and other 4%). The senior caregiver was most often the teen's mother (70%) or grandmother (11%) and had a similar racial distribution and with median age of 45 years +/− 10 years. Variation in loss to follow-up was also reviewed. Cases with missing KABI data were similar to complete cases on all demographics (i.e., teen age, education level, family structure, finance sources, and job status) except race. Complete cases were more likely to be White (Fisher's exact test [two-sided = .03, one-sided = .03]). Cases with missing home visit data were similar to complete cases on all demographics.
Research Question Results
In the comparison of KABI scores for TM/SCG and CG, the TM/SCG was found to have increased scores on all four constructs and held more positive views than controls (p < .001). As shown in Table 2 and Figure 2, TM/SCG participants demonstrated higher scores on all scales. Specifically, TM/SCG participants were significantly more likely to have more positive beliefs about safe sleep (F(2,98) = 18.4, p < .001), were more likely to report intent to practice safe sleep for their infants (F(2,98) = 10.9, p < .001), had higher self-efficacy related to infant safety (F(2,98) = 9.40, p < .001), and had more positive attitudes about safe sleep practices (F(2,98) = 17.69, p < .001).

Mean comparison of safety knowledge, attitudes, beliefs, and intents (KABI).
For the observations in the home visit, as shown in Table 3, there were no differences in the safe sleep practices by intervention status. Overall, 84% of participants completed the observational task of placing the baby to sleep on their back. An examination of the participant report of behaviors at the home visit showed no differences were reported in the use of safe position; however a trend supporting the intervention was seen with more intervention infants most often being positioned on their back (69% of CG compared to 85% of TM/SCG, p = .082). No differences were seen across intervention and comparison groups for safe positions the night before (78% reported back to sleep), use of back position “every night” or “at least half the time”.
Comparison of Safe Sleep Behaviors (SSB) by Treatment Status and Mode of Assessment.

Note., aPosition last night, back every time; bEver in life use unsafe, Last time surface, Safe Surface Every time; cNever same bed, never with others; dNever with unsafe. AAP = American Academy of Pediatrics: SCG = Senior Care Giver; TM = Teen Mother Only.
**p < .001, + p < .10, N = 74–80.
Most participants (78%) were observed using safe sleep surface and most (71%) “most often” used a safe sleep surface; but no intervention differences were observed. There was no intervention advantage for use of safe sleep surfaces the “last time” the child was put to sleep, use of safe surfaces “at least half of the time”, nor “ever in life used an unsafe” surface. However, participants that reported use of a safe surface “every time” was more likely if the participant was in the intervention group (19% of CG compared to 47% of TM/SCG, p = .001).
Most participants (78%) were observed using a safe sleep location and reported using a shared room most nights (86%) but no intervention differences were observed. There was no intervention advantage for use of safe sleep location such as “never the same bed” (62%); however, the difference trended in favor of the intervention group (50% of CG compared to 70% of TM/SCG, p = .069). The intervention and comparison groups were similar in the self-report of allowing the child to sleep with others (87%).
Less than half of the participants (45%) removed all safety hazards in the sleep space and the rates were not statistically different across groups. A trend was seen in favor of the intervention for participant report of ever in the infant's life allowing unsafe objects in the sleep area (50% of CG compared to 70% of TM/SCG, p = .067).
Discussion
While significant gains have been made in the reduction of deaths from SUID, the decrease has stalled. Despite longstanding campaigns promoting back to sleep, the need to identify novel opportunities to engage parents to address sleep safety is indicated by ongoing high rates of sleep-related death. This is particularly the case for minority women, young adults, and those living in poverty as was targeted in this study. SBS offers an additional opportunity to engage expectant mothers, particularly those in high-risk populations, in a positive manner and with relatively low costs.
The tailored SBS was successful in increasing the basic KABI of participants compared to a randomized comparison group. While the effect sizes were small (∼.2, Table 2), these findings are consistent with the results of more costly interventions. However, in similar implementations of SBS (Sanguino et al., 2010), the increased knowledge did not clearly translate into parenting behaviors that were at the level of current recommendations. That is, there was limited evidence of behavior change in the home after the child was born. Whether observed in the home visit or reported by the parent, there were no statistically significant differences in the safe sleep practices by intervention status. Given the small sample, however, we noted treatment differences at the trend level (p < .1). There were several, all in favor of safe sleep among the intervention families and based on parent report.
Infants were most at risk from objects in the bed, with 55% of infants exposed to unsafe objects. Risks related to sleep surface and sleep location were similar with 22% of infants exposed to risks. As in other studies, the most successful action implemented by new mothers is “back to sleep” with only 16% of infants at risk. Rates for parent report appeared similar and within about 10% with one exception. We observed nearly twice as many infants with unsafe objects (50%) than mothers reported (27%). Mothers underreported on their use of safe sleep surfaces (85% observed compared to 74% reported) but overreported on the use of safe sleep locations (79% observed compared to 89% reported). While this was not a focus of our analyses, this information may be helpful in the revision of the SBS intervention and in the development of future interventions that can increase focus on these areas. One obvious reason for differences between parent report and observation is that observation is based on the one snap shot of the environment; whereas parent report is based on a wide range of time. On the other hand, parent report of behavior may be influenced by social desirability.
Strengths and Limitations
Our study was limited by several factors, most notably challenges in recruitment and retention of expectant teens resulting in reduced home observation data that did not have the power to detect a true change, despite trends toward intervention effectiveness. In addition, the sample in the study is largely African American and may therefore not be fully representative of teen mothers nationally. The study was conducted in English, limiting the participation of potential participants who speak other languages. Additional study of the intervention, tailored to cultural and language differences, are indicated. Finally, our definition of safe did not discriminate between the potential of unaccustomed supine sleep which may have underrepresented the danger to infants (e.g., “all of the time” vs. “most of the time”). Infants are thought to be in more danger when placed in a usual position (Colvin et al., 2014).
Implications for Practice
First-time pregnant teens who attended a SBS intervention focused on safe sleep and on other injury risks that are common during the first year of life demonstrated higher levels of self-efficacy and intent to adhere to safe sleep practices than a control group of pregnant teens who had standard of care educational materials. Direct observation of safe sleep practices in the home failed to detect a significant difference in practices, but was limited by challenges in subject retention and ability to conduct the home visits in other cases. However, even with limited power, we found data trended toward a larger proportion of intervention mothers demonstrating safe sleep practices than the control group.
Conclusions
The “Back to Sleep” campaign demonstrated a link between knowledge and improved sleep for infants overall; however, was least successful with minorities (Pollack & Frohna, 2002). However, in other areas of sleep safety, the link between new knowledge and safe sleep is less clear. It appears that even when young mothers gain knowledge and increased intent to act, they have difficulty implementing this information. In practice, this suggests that exploring the barriers prenatally with this population and offering suggestions to overcome the barriers is indicated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This research was supported by the National Center for Advancing Translational Research under award U54TR001629 (UAMS Translational Research Institute pilot grant program) and by the Eunice Kennedy Shriver National Institute of Child Health and Human Development under grant award R01HD076702. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Institutes of Health.