
Abstract
Background
Medical care facilities in both developed and developing countries around the world continue to invest in hospital information technologies (HITs). Nevertheless, it has been discovered that user acceptance of these technologies is one of the imperative issues during their implementation and management in developing countries such as Ghana.
Purpose
Notably, the technology acceptance assessment of nurses is a timely one since they play a very important role in the medical sector. Based on the model of “Unified Theory of Acceptance and Use of Technology,” this study explored the factors that affect Ghanaian nurses’ acceptance of HIT.
Conclusions
Precisely, HIT systems are essential in the quality and the enhancement of nursing services provision and in the effectiveness of the performance of nursing staff. This study, therefore, offers a piece of empirical evidence for hospital administrators in developing countries especially Ghana, to assess the success probability of new HITs before and after their implementation.
Keywords
Implementation and expansion of “Hospital Information Technologies (HITs)” are some of the core global determinations to improve patient care protection and medical quality (Buabbas et al., 2019; Wu et al., 2011). Medical care facilities in both developed and developing countries around the world continue to invest in hospital information technologies (HITs). Nevertheless, it has been discovered that user acceptance of these technologies is one of the imperative issues during their implementation and management in developing countries such as Ghana.
Nurses form a larger portion of the health-care staff and therefore, their behavior toward HITs use could likely have a greater effect on the acceptance and implementation process of “electronic health records” (Giuse & Kuhn, 2003; Huryk, 2010). Health-care organizations continuous investment in HIT have brought about the recognition of user acceptance and implementation as important issues in the management of HITs worldwide (Hu et al., 1999). Consequently, more than 40% of the changes in information technology (IT) in different areas of medical care systems have resulted in disappointment/rejection (Aarts & Gorman, 2007). Inadequate consideration of the technical aspects, particularly of how organizations and individuals accept IT is one of the reasons that culminated in such failures (Aarts & Gorman, 2007; Bawack & Kala Kamdjoug, 2018; Giuse & Kuhn, 2003). Besides, nurses are afraid that the use of HIT may desensitize patient care (Huryk, 2010). Actually, users’ adoption and individuals’ utilization of the IT collectively form the most valuable factors contributing to successful acceptance and implementation of HIT (Selder, 2005). The adoptions of such HIT systems in some developing and developed countries have now become a certainty. Nevertheless, nurses as a group of caregivers have been discovered to counterattack automation. They usually recognize computerized systems in hospitals as uncaring and desensitizing (Alquraini et al., 2007). A developing trend indicates an increasing number of HITs as more hospitals become interested in creating and maintaining electronic health records systems (Kuo et al., 2013). However, such technological systems are not always completely utilized by the core staff members such as nurses (Secginli et al., 2014). The development of HIT systems, its acceptance and usage are quite challenging (Ahlan & Ahmad, 2014; Ologeanu-Taddei et al., 2016), while IT use has produced countless studies that have investigated factors affecting its acceptance and implementation. In fact, understanding the reasons for HIT use, in addition to assessing the factors that influence the acceptance of HITs, may help to confirm whether their use is successful. Pertinently, nurses should be the major users of HITs since they play a central role in medical care settings. Certainly, their adoption and usage of HIT applications are regarded as crucial signs of a positive implementation of HIT system (Alquraini et al., 2007).
There are several technology acceptance theories and models that have been in operation in the medical care field (Aggelidis & Chatzoglou, 2009; Holden & Karsh, 2010). The concept of Unified Theory of Acceptance and Use of Technology (UTAUT) was developed via review, integration, and mapping of eight dominant theories and models. Previously, these models and theories have been successfully utilized in other studies (Ahlan & Ahmad, 2014; Ketikidis et al., 2012; Melas et al., 2011; Wu et al., 2011) on technology or adoption of innovation as well as circulation within both the information systems (IS) area and different fields of study. The UTAUT model integrates all the features in the earlier theories and is proficient in offering results that are acceptable in genuine systems and samples (Venkatesh et al., 2003). The UTAUT model explains 69% of the variance of the intentions of individuals’ acceptance to use any form of IT. However, the earlier theories only explained 40% of intentions of individuals acceptance of ITs (Bawack & Kala Kamdjoug, 2018; Kijsanayotin et al., 2009).
The Study Aims and Hypotheses
The purpose of this study was to discover factors affecting the acceptance rate of nurses use of HITs in three teaching and two regional hospitals in Ghana through the UTAUT model (Venkatesh et al., 2003). The proposed UTAUT model was validated appropriately to provide a combined theoretical groundwork wherein the research on IS or adoption of IT and dissemination could be promoted. Four core parameters that were suggested by the UTAUT model and applied to directly determine health IS or health IT use behavior and behavior intentions (BIs) were performance expectancy (PE), effort expectancy (EE), social influence (SI), and facilitating conditions (FC) (Venkatesh et al., 2003). In addition, through the model, it was assumed that factors such as age, gender, experience, and voluntariness to use greatly moderate the effect of key parameters (Venkatesh et al., 2003).
In this context, it was therefore logical to map out and bring the various concept together and create a merged theoretical basis (Venkatesh et al., 2003). The research hypotheses of this study were the following: H1: PE is a predicting factor of nurses’ adoption of HIT system; H2: EE is a predicting factor of the nurses BI to use HIT system; H3: nurses “attitude towards use of technology (ATUT)” is a predicting factor of nurses’ adoption of HIT system; H4: SI is a predicting factor of the nurses’ BI to use HIT system; H5: FC is a predicting factor of the nurses’ BI to use HIT systems. The research model (depicted in Figure 1) was adopted from the original UTAUT model.

The Research Model.
Method
Research Study Design, Settings, and Participants
A descriptive cross-sectional research assessment was conducted in selected hospitals in Ghana during the 3-month period from January to March 2019 (Bani-Issa et al., 2016; Zhou et al., 2019). This study focused on primary data derived from nurses from five major public hospitals in Ghana where HITs were being applied for patient care. All the nurses who attended to patients care at the aforementioned hospital qualified to participate in this study. These hospitals were selected because their facilities provide HIT systems, giving nurses the opportunity to use IS in their daily work. A purposive sampling approach was used to select five public facilities comprising of three teaching and two regional hospitals that use HITs in Ghana. Six hundred and sixty nurses out of a targeted nursing population of 52,136 were randomly selected from the 5 public hospitals in Ghana (Esmaeilzadeh et al., 2015).
Material and Procedure
Data were collected from January to March 2019 via an organized questionnaire composing of items based on constructs validated in the original English version of the UTAUT model as described elsewhere (Venkatesh et al., 2003). An electronic data were obtained (via smart mobile phones and tablets) with structured questionnaire coded in Open Data Kit (ODK) application (Wright et al., 2015). The questionnaire was pretested severally before being sent out for the data collection. The feedback of the pretesting prompted the authors to make minor modifications to suit the study settings. The modified survey questions were tested for validity, reliability, and accuracy. Almost all the selected nurses were approached during their working shifts and were contacted either through a mobile phone or verbally to take part in this study. The electronic questionnaires (made with ODK mobile application) were distributed to the nurses personally by the authors and other supporting data collectors. Completed questionnaires were automatically sent to our ODK Google aggregate server-based website for download in excel format. All the questions were written in understandable English language and each questionnaire took about 4 to 10 minutes to complete. The questionnaire composed of 42 questions including demographics. Consistent with a previous study (Maillet et al., 2015; Ologeanu-Taddei et al., 2016; Venkatesh & Morris, 2000), structural measurements were performed using the 7-point Likert-type scale, with 1 expressing strong disagreement and 7 expressing strong agreement. All the questions were closed and designed according to the 7-point Likert-type scale to suit the answers. Researchers personally sent questionnaires to recruited nurses working in the five hospitals using HIT systems.
Model Instruments and Measurements
The reliability of the data collected was evaluated by detecting Cronbach’s alpha (CA) coefficient. The “SmartPLS-SEM application software” (v. 3.2.8) was used for the estimation of the path analyses and the model hypotheses testing (Hoque & Sorwar, 2017; Mateos-Aparacio, 2011). Parameters were measured directly through indicators designed to elicit responses associated with a variable (Gefen et al., 2000). Most researchers use structural equation modeling (SEM) as a measurement statistical tool for analyzing data. In SEM evaluation, a causality network is estimated by researchers with respect to a theoretical model. The main UTAUT study reported using the “partial least square” path modeling approach (Venkatesh et al., 2003) as having negligible demands on sampling size, residual or underlying data distributions, and measurement scales. Reliability is associated with the measurement within parameters that is independent of the state within other variables, while construct validity is associated with the measurement within parameters (Gefen & Straub, 2005; Straub et al., 2004). The assessment of the “internal consistency reliability” of parameters such as CA was applied to examine the one-dimensionality of a group of the survey questionnaire measurements. Moreover, additional analysis such as “average variance extracted” and “Composite reliability” for the individual construct provides coefficients that confirmed the reliability of the survey (Abdalla Mohammed & Muhammed Pandhiani, 2017). In this regard, 0.70, 0.70, and 0.50 were estimated as the respective recommended values. The linear correlation coefficient (R2) of each dependent construct in the model was generated in order to assess whether the model fits well with the hypothesized relationship (Mateos-Aparacio, 2011). Notably, R2 is interpreted as the proportion of explained variance similar to regression analysis and therefore denotes the percentage of variance in the dependent constructs that are explained with the independent ones.
Reliability and Validity of Measurement
The CA for testing the overall reliability for the measurement items was 0.949, while the Kaiser–Meyer–Olkin Measure of sampling adequacy was 0.928.
Results
Demographic Characteristics of the Respondents
Notably, majority of nurses in Ghanaian hospitals are females. Hence, it was not surprising that 404 (61.2%) of the respondents were females. The respondents’ demographic data have been summarized and depicted in Table 1. Staff nurses were the most usual nursing category title among the respondents (58.4%). Most respondents (52.4%) were between the ages of 20 and 30 years with all the respondents having at least diploma degrees. A portion of (48.03%) of the respondents had over 1 to 5 years of professional experience, while almost all the nurses have had at least 1 year of HITs experience.
Demographic Characteristics of Respondents.
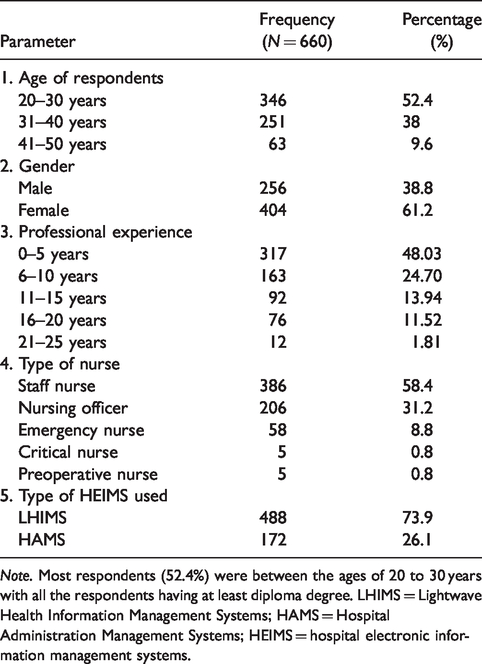
Note. Most respondents (52.4%) were between the ages of 20 to 30 years with all the respondents having at least diploma degree. LHIMS = Lightwave Health Information Management Systems; HAMS = Hospital Administration Management Systems; HEIMS = hospital electronic information management systems.
Table 2 shows the reliability and validity results for each construct. The CA value greater than or equal to 0.70 is considered to be the criterion to prove the internal consistency of the scales (Tavares & Oliveira, 2017; Vannesteet al., 2013). The internal consistencies of the measurement variables were considered satisfactory since the CA recorded for each of them were more than 0.72, representing satisfactory reliability as shown in Table 2.
Reliability and Validity Testing Results for Each Construct.

Note. AVE = average variance extracted; CR = composite reliability; CA = Cronbach’s alpha; KMO = Kaiser–Meyer–Olkin; SI = social influence; FC = facilitating conditions; BI = behavioral intention.
The Measurement Models
The model is composed of 9 observed variables, namely, PE, EE, ATUT, SI, self-efficacy, FC, computer anxiety, BIs, and use behavior with 34 total items. In this report, the measurement was primarily based on five of the constructs. The overall goodness of fit was assessed via some model fit measures. The results of the goodness-of-fit statistics are depicted in Table 3. As shown earlier, the required criteria for the majority of the fit indices were met. This result represents a reasonable fit between the obtained data and the suggested model measurement. In view of this, the instrument’s psychometric properties were evaluated regarding the “discriminant validity,” “convergent validity,” and reliability. The findings of the items’ loadings, means and the CA for all the measurement items (when an item is deleted) statistics are depicted in Table 3. The standardized loads of most of the measurement items were greater than 0.7, which shows good convergence validity (Handayani et al., 2017; Kim et al., 2015).
The Actual and Recommended Values of Fit Indices.

Note. χ2/df is the ratio between Chi-square and degrees of freedom. GFI = goodness-of-fit index; AGFI = adjusted goodness-of-fit index; CFI = comparative fit index; NFI = normed fit index; RMSEA = root mean square error of approximation.
The Structural Model
The structural model was examined via SEM technique with the effects of five latent variables tested. The findings showed that the nurses’ intention to use HITs systems in terms of their behavior was predicted by SI (t = 3.656, p < .001), FC (t = 2.616, p < .001), and ATUT (t = 5.861, p < .001; Table 4). In terms of usage intention of HITs by the respondents, SI, FC, and ATUT explained a total variance of 60.7% (R2=0.607) as indicated in Figure 2. Furthermore, SI, FC, and ATUT substantially impacted the BIs to use HITs (p < .001), which respectively supported H2, H3, and H4 (Table 4). The majority of the hypotheses were strongly supported with a significance level of at least 99%. The standardized SEM results from the structural model analyzed with SmartPLS are depicted in Figure 2 (the standardized path coefficients which signify the substantial structural association within the tested parameters).
Hypotheses Testing Results.

Note. The results of the application of Structural Equation Modeling technique to estimate the path coefficients and test of the model hypotheses. ATUT was the strongest predictive factor that plays a key part in the nurses’ intention to use HIT systems. PE = performance expectancy; BI = behavioral intention; EE = effort expectancy; ATUT = attitude toward the use of technology; SI = social influence; FC = facilitating conditions.
***Significant level is at p < .001.

The Structural Model of the Constructs.
Discussion
Nurses’ resistance to health technology use is high (Alquraini et al., 2007); however, their intention to use HIT systems were observed to be encouraging and had a significant contribution. The findings show that the nurses’ intention to use HITs systems in terms of their behavior was predicted by SI (t = 3.656, p < .001), FC (t = 2.616, p < .001), and ATUT (t = 5.861, p < .001). The effects of the aforementioned constructs explained 60.7% (R2= 0.607) of the variance in the nurses’ intentions to use HIT systems. As represented in Table 4, three out of five of the research main constructs hypotheses were confirmed to be supportive which was consistent with the results of Aggelidis & Chatzoglou (2009). The outcomes in the study are supported by the suitability of the key constructs denoted in the UTAUT model. Indeed, two main constructs (PE and EE) were confirmed in this report to be not supportive of the hypotheses. This demonstrates that the performance and effort expectancies are not key factors contributing to the nurses’ acceptance and adoption of HIT systems in Ghanaian hospitals. This outcome is in contrast with a similar study conducted in Iran by Sharifian et al. (2014). Probably, this discrepancy could be ascribed to the lack of nursing informatics in the training program of nurses in developing countries such as Ghana. According to the UTAUT model, SI is defined as “the peoples’ perception about how important they are to the society based on what they do or behave towards achieving their goals in their immediate working environment or surroundings” (Venkatesh & Zhang, 2010, p. 11). The key concepts of SI were image, social factors, and subjective norms. The way people act or behave in their immediate environment is basically based on the aforementioned concepts which have a substantial influence on what they do or will not do. Most of the nurses’ acceptance and adoption of HIT systems were based on these concepts. The BI was significantly influenced by SI to use and adopt HITs in Ghanaian hospitals (Kijsanayotin et al., 2009). The UTAUT model describes FC as “the necessary IT resources needed to use a system, and the technical infrastructure that exists to support this usage.” Moreover, it further defines FC as the degree to which an individual believes that an organization can provide the necessary knowledge and training for using HIT. Relevantly, since medical care providers such as nurses are likely to resist technology (Alquraini et al., 2007), there is the need to adequately equip them with technological equipment and good training to use HITs, else the adoption could be rejected.
The UTAUT also defines ATUT as whether users think the system is good or bad and in addition if the system makes work more interesting or not. Three main constructs (SI, FC, and ATUT), therefore, strongly contributed to the nurses’ BIs in relation to the HIT use. The nurses’ BIs to use HIT systems is a result of the discernment that they think; 1. “that the system makes work interesting and also using the system is good (ATUT),” 2. “that they feel motivated to use the system when been admired by family and friends (SI),” and 3. “that their health facilities provide the necessary technical and system support for the usage of the HIT system (FC).” The projecting influence of the three measurements was significant and contributed to the positive intentions of the nurses to use HIT systems. More importantly, the outcome of this study showed that of the three significant contributing factors, ATUT was the stoutest predictive factor that plays a key part in the nurses’ intentions to use HIT systems. These findings are consistent with studies that showed ATUT to be more effective in users’ intention to accept and use HIT system (Chow et al., 2012; De Veer & Francke, 2010; Vanneste et al., 2013).
Limitations of the Study
The limitations of this study were that HITs are relatively new areas in the training of nurses in Ghana and consequently the small number of health-care facilities have access to it. The selection of respondents was limited to only public major teaching and regional hospitals.
Conclusion
Hospitals’ nursing staffs are the core component of the respective hospitals around the world, especially in developing countries. Thus, if their intention toward using new HITs is negative, the daily routine of patient care may potentially be compromised in terms of patient safety and care. The contributing factors supporting nurses’ adoption of HIT systems are assumed to be beneficial to their health-care facilities. This study offers empirical evidence for administrators of hospitals in developing countries and in Ghana especially, to assess the success probability of new HITs and the factors to consider during the implementation process. This may also help the nurses to understand the importance of adoption of new HITs.
Footnotes
Acknowledgments
The authors would like to thank all the Nurses who avail themselves for the success of this study. The authors would like to also thank the National Natural Science Foundation of China.
Author Contributions
All authors contributed equally to the writing of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
This study was approved by the Ghana Health Service Research Ethical Committee (no. GHS-ERC:05-12-18). The Health facility Directors/Managers also gave approval before data were collected. Participants were guaranteed of response anonymity. The consent of the respondents was sought though participation was voluntary. Respondents also signed consent forms before answering the electronic questionnaire.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Natural Science Foundation of China (grants nos. 71974079 and 71904066).