
Abstract
Introduction
Research shows steady growth in clinical leadership (CL); however, CL is still misunderstood in all clinical environments. Few studies have been conducted on the CL needs of nursing staff. No studies have linked CL needs (CLeeNs) in nursing to safety climate (SC) in clinical settings. Therefore, this study analyzed the differences in the perceived nurses’ CL needs and SC between nurses and nurse managers.
Methods
A cross-sectional research design was implemented employing an online survey. A convenience sample of 252 registered nurses (RNs) and 139 nurse managers was employed using the Clinical Leadership Needs Analysis (CLeeNA) instrument and the Safety Climate Survey (SCS).
Results
The chi-square test showed that nurse managers differed from nurses in most of the sample demographics, except in their time commitment, area of work, and the reported decision-making style in their area of work. The mean score of the overall scale of CLeeNs was “very important” (M = 6.05, SE = 0.072). The highest mean of the subscales was for “standards of care.” In contrast, the lowest mean of the subscales was “financial and service management.” The T-test revealed that the total mean score of CLeeNs was higher among nurse managers as compared to that of nurses (6.52 ± 1.01 vs. 5.79 ± 1.55, p = .001), which held the same trend for all subscales and the individual mean scores of CLeeNs for the privilege of nurse managers. The mean score of the perceived SCS of the total sample was 3.41 (SE = 0.032), indicating negative perceptions of the SC. Although there were no statistically significant differences in the total and individual mean scores of SC (p = .252), nurse managers reported slightly higher scores (3.46 ± 0.64) than nurses (3.38 ± 0.62). This result indicates that there were no significant differences found between RNs and nurse managers in SC scores, and a weak negative correlation was observed between CLeeNs and SC.
Conclusions
CL and CLeeNs are essential for a safe climate; however, little is known about how nurses and nurse managers differ in their perceived CL and SC in practice. CL should be sustained in all hospital settings. The low perceived SC is worrying and mandates immediate intervention at all organizational levels. Notably, a negative correlation was observed between CLeeNs and SC, suggesting that stronger perceptions of CL do not necessarily translate into more favorable SC perceptions.
Introduction
Clinical leadership (CL) encompasses clinical excellence by equipping individuals with the necessary skills, support, and guidance while emphasizing collaborative efforts across various disciplines (Mrayyan, 2022a, 2022b; Stanley & Stanley, 2018). Additionally, CL involves having clinical knowledge within a specialized field and ensuring that professionals are actively engaged in clinical care and patient safety (Mrayyan et al., 2023b; Stanley & Stanley, 2018). Therefore, the nursing staff must have the necessary skills to support high-quality and safe patient care; nurses’ and nurse managers’ clinical leadership needs (CleeNs) should be continuously assessed and updated.
One critical area where CL plays a pivotal role is in shaping the safety climate (SC) within healthcare settings. SC refers to the shared perceptions and attitudes of healthcare workers regarding the importance and implementation of safety-related practices, policies, and procedures (Mrayyan, AL-Atiyyat et al., 2023a). A strong SC reflects an organizational culture that prioritizes safety, which in turn influences staff behavior and overall safety performance. Clinical leaders contribute to this climate by modeling safety-oriented behaviors, promoting adherence to safety protocols, and fostering open communication about safety concerns. As (Mrayyan et al., 2023b) emphasized, the presence of effective CL is essential for maintaining a safety-focused environment, underscoring the need to support and develop clinical leaders in all areas of patient care.
Problem, Purpose, and Significance
With ongoing changes in clinical settings, it is essential to emphasize the importance of CL and CLeeNs. Nurse managers are rarely assessed for CL, often based on the assumption—held by organizations or healthcare systems—that their leadership competence surpasses that of nurses, particularly in power and empowerment (Mrayyan, 2022a, 2022b). However, this assumption warrants scrutiny, as power dynamics and empowerment directly influence leadership effectiveness and staff engagement. Therefore, all personnel, including managers, should demonstrate CL skills, ensuring high-quality, safe patient care (Mrayyan, 2022a, 2022b).
Despite CL gaining attention in the nursing literature, its definition remains unclear (Mrayyan et al., 2023b). Few studies examine its role in fostering a safety-focused work culture (Mc Carthy et al., 2019a, 2019b). The specific CLeeNs of nursing staff are underexplored (Mrayyan, 2022a, 2022b), and CL is rarely studied from nurses’ perspectives, especially in comparison to managers. Research integrating both concepts is scarce, making this study the first international investigation of CL and SC in nursing.
Strong CL is vital for shaping healthcare, patient care, safety culture, and team effectiveness. Clinical leaders inspire and transform workplaces into secure, supportive environments (Mrayyan et al., 2023b). This study assesses how nurses’ perceived CL affects SC in hospital settings by examining differences between nurses and nurse managers, presenting a novel research direction.
Theoretical Framework
The Transformational Leadership Theory, brought to life by Bass and Riggio in 2006, serves as the foundation of this study. It offers a solid framework for exploring the diverse CLeeNs and how nurses and nurse managers view the SC. This theory pointed out the significance of motivating team members through the 4Is: “Idealized Influence” (acting as a role model), “Inspirational Motivation” (sharing a compelling vision), “Intellectual Stimulation” (encouraging innovation), and “Individualized Consideration” (providing personalized support).
In this study, “Idealized Influence” showcases how nurse managers act as role models by embodying professional values, which in turn helps them earn the respect of their teams. “Inspirational Motivation” is about creating motivation that energizes the team members and aligns them with shared goals. When there is a lack of this kind of inspirational leadership, perceptions of the SC can take a hit, leaving staff feeling disconnected from the organization's safety priorities (Zhang et al., 2025). “Intellectual Stimulation” is essential for promoting innovation and effective problem-solving in the bustling clinical environments. Nurse managers lead the charge in strategic planning and innovation initiatives (Zhang et al., 2025). Finally, “Individualized Consideration” highlights the value of personalized mentorship and support, which can greatly enhance the safety climate, boost psychological safety, and reinforce the overall safety culture (Zhang et al., 2025).
Transformational leadership positively influences organizational climate, employee satisfaction, and patient outcomes. The transformational leadership approach is particularly effective in high-stress environments like healthcare, where relational leadership tends to lead to fewer adverse events and better team performance (Ystaas et al., 2023). Moreover, organizational climate is a key link between transformational leadership and work engagement, highlighting how a leader's style can shape feelings of job satisfaction and SC (Zhang et al., 2025).
When looking at the application of the 4Is, it is important to recognize the connection between transformational leadership behaviors and perceptions of SC. Nurse managers might face a growing need for CL, as they are expected to embody transformational qualities. These qualities, especially inspirational motivation and individualized consideration, are directly tied to how staff perceive the SC in their work environment. There is also the assumption that any differences in how SC is perceived could reflect variations in the practice or interpretation of transformational leadership across various positions. Thus, exploring these differences helps clarify how transformational leadership contributes to shaping a safety-oriented culture. Furthermore, differing scores in SC suggest a lack of inspirational motivation and individualized consideration, two crucial traits expected of transformational leaders (Khan et al., 2022).
Literature Review
Many professional organizations have recognized the importance of cultivating CL, with the International Council for Nurses (ICN) highlighting this as a core competency for nurse leaders (Blanck-Köster et al., 2020). CL has been acknowledged as a vital component of nursing practice and advanced practice roles (Blanck-Köster et al., 2020; Stanley & Stanley, 2018); therefore, CLeeNs should be assessed and promoted.
Clinical Leadership: Clinical Leadership Needs
As CL plays a crucial role in enhancing healthcare by cultivating innovative work environments, the demand for effective CL goes beyond personal abilities; CL necessitates customized development programs that are intricately integrated into organizational frameworks. The evolution of CL is a continuous and dynamic journey that is built on CLeeNs; therefore, it necessitates the amalgamation of individual skill development with systemic strategies.
CL is multifaceted; it has different roles, characteristics, and outcomes (Mrayyan et al., 2023b). More specifically, the roles associated with CL involve having a vision, upholding professionalism, fostering teamwork, engaging in ongoing medical education, executing tasks efficiently, and ensuring patient safety. Effective CL is characterized by approachability, strong communication skills, the capacity to advise and guide, serving as a role model, and the ability to facilitate change. Key competencies in CL include maintaining clinical engagement, showcasing clinical expertise, and understanding the intricacies of clinical decision-making (Mrayyan et al., 2023b).
There are many skills necessary for and actions produced by clinical nurse leaders (Mrayyan et al., 2023b; Mrayyan, 2022a, 2022b; Stanley & Stanley, 2018). The authors reported that CL skills comprise (1) a clinical focus, which involves being clinically oriented, delivering evidence-based care, and comprehending CL and decision-making processes; (2) a focus on personal qualities, which includes initiating change, engaging in reflective practices, possessing advocacy skills, and ensuring safe and healthy work environments; and (3) a team focus, which entails being an effective communicator, providing support to colleagues, and exemplifying role-model behavior. The actions associated with CL involve enhancing healthcare systems, adhering to personal values and beliefs, being accessible, delivering safe and high-quality care to clients, delegating responsibilities related to safety and quality, executing strategic plans, and fostering the organization's SC (West, 2021), which is the primary focus of the current study.
CL plays a significant role in enhancing outcomes for nurses, patients, and healthcare organizations (Mrayyan et al., 2023b; Stanley & Stanley, 2018). However, it is essential to assess the degree to which CL influences these outcomes (Duignan et al., 2021). Clinical nurse leaders are instrumental in delivering effective nursing care and ensuring patient safety; therefore, it is imperative to develop and customize leadership training programs that focus on fostering CL and cultivating a culture of safety within nursing (Mrayyan, AL-Atiyyat et al., 2023a; Mrayyan et al., 2023b).
Safety Climate
Establishing a safe climate is an essential objective for all healthcare organizations. The term SC broadly refers to the policies in place, as well as the attitudes and beliefs of employees regarding safety in the workplace (Dirik & Intepeler, 2017; Mrayyan, AL-Atiyyat et al., 2023a). Effective CL contributes to improved outcomes for patients, nursing staff, and healthcare institutions by reducing adverse incidents (Akbiyik et al., 2020), enhancing control, fairness, and values, decreasing costs, and aiding in the retention of clients (Dirik & Intepeler, 2017; Dutra & Guirardello, 2021; Mrayyan, AL-Atiyyat et al., 2023a), thereby strengthening the SC. Consequently, clinical leaders must serve as role models and exemplars of expertise (Mrayyan et al., 2023b; Stanley & Stanley, 2018). Merely adhering to standards is insufficient to ensure the safety and engagement of employees (Mrayyan, AL-Atiyyat et al., 2023a). Clinical leaders are essential for fostering a workforce and institutions that are dedicated to a safe climate (Mrayyan, AL-Atiyyat et al., 2023a). The Australian Commission on Safety and Quality in Health Care (2024) emphasized that the workforce must possess the appropriate qualifications, skills, and oversight to deliver safe, high-quality healthcare to patients. In this context, clinical leaders play a vital role in addressing safety-related matters.
The existing literature indicates a scarcity of nursing research pertaining to CL and SC, highlighting the necessity for CL that fosters an SC conducive to enabling nurses to deliver high-quality care and be safe to their patients. Consequently, this study was undertaken to address the identified gap in nursing leadership literature by examining the CL requirements and SC and comparing these variables among nurses as compared to nurse managers in Jordan. The study may serve as a foundation for the development of leadership competencies encompassing both CL and SC.
Methods
Design, Sample, and Settings
Guided by STROBE (2014), data were gathered using a quantitative cross-sectional comparative design based on the sample's characteristics. A cross-sectional design was used as it allows the study of outcomes and numerous attributes (Polit & Beck, 2019). A convenience sample of registered nurses (RNs) and nurse managers in Jordan was recruited using the CLeeNA instrument (Mc Carthy et al., 2019a, 2019b) and the Safety Climate Survey (SCS) (Sexton et al., 2006). Of 391 Jordanian nurses and nurse managers, there were 252 (64.50%) nurses and 139 (35.50%) nurse managers who were working in different hospitals in Jordan; three governmental, three private, and two teaching hospitals were recruited. The response rate in the current study was 71.09% (391/550).
The sample size was determined using Thorndike's rule, N ≥ 10(k) + 50, where k is the number of independent variables. With seven CLeeNA subscales, one SC scale, and 15 sample characteristics (k = 23), the minimum N was 10 × 23 + 50 = 280. The current authors enrolled 391 participants.
Data Collection Procedures
This study is a continuation of the authors’ work on CLeeNA, which started in 2020. The Institutional Review Board (IRB) at the university affiliated with the authors approved the study's protocol (No. 1,2/1/2020/2021, dated October 18, 2020). However, a new data collection occurred online in October 2023 through a survey created with Google Forms. This current wave of data collection focused on CLeeNs and SC. The current study was preceded by a pilot study that confirmed the survey's effectiveness. The researchers promoted the study across various electronic platforms. Given that English serves as the instructional language for nursing education in Jordan, the survey was conducted in English.
The survey link was disseminated via the personal and professional Facebook accounts of the researchers, as well as the Faculty of Nursing's pages, to broaden the potential respondent base. Participants were encouraged to share the survey within their networks through Facebook and WhatsApp. The survey remained accessible for 1 month, with a reminder sent after 10 days. To prevent duplication, the survey was configured to accept only one response per participant by enabling Google Forms’ “Limit to 1 response” feature, which required sign-in and tracked submissions. Additionally, participants were instructed not to complete the survey more than once, and no duplicate entries were detected during data cleaning. No incidents were reported during the data collection phase. Effective communication was used to minimize attrition and emphasize the study's importance by sharing clear, concise, and participant-focused information.
Participation in the survey was entirely voluntary, allowing individuals to skip questions or refrain from submitting their responses. To maintain privacy, the primary researcher stored the coded responses of participants in Google Forms, which is secured by a password. Google Forms utilizes HTTPS to encrypt data during transmission, ensuring the security of information as it moves from the participant to Google's servers. Additionally, the primary researcher employed Two-Factor Authentication (2FA) for personal email to enhance security measures. To uphold confidentiality, the aggregated findings were shared with nursing and hospital administrators at the higher management level.
Instruments
A demographic questionnaire was created and aimed at assessing various characteristics of the sample (see Table 1).
The Total Mean Scores and Standard Deviations of the Perceived Clinical Leadership Needs Scale and Subscales and the Safety Climate Scale in the Whole Sample (n = 391).

Note. Scale scores were summarized with means and standard errors.
The Clinical Leadership Needs Analysis (CLeeNA)
The CLeeNA was employed to gather data (Mc Carthy et al., 2019a). Prior to data collection, authorization for the use of this tool was obtained. The instrument primarily evaluates the significance of leadership requirements for nursing professionals. In the present research, the CLeeNA was utilized in its original English version, which is culturally appropriate and aligns with the fact that English serves as the official language for nursing education in Jordan. The CLeeNA comprises a seven-factor framework consisting of 56 items, rated on a 7-point adjectival scale ranging from 1, indicating not important, to 7, denoting highly important. In their foundational study aimed at developing and validating the CLeeNA scale, Mc Carthy et al. (2019a) employed a cross-sectional design with 324 RNs and midwives. They conducted principal component analysis, parallel analysis, and item reduction to identify the scale's structure, resulting in the reduction of 103 items to seven factors encompassing 56 items. The seven factors identified included the following: self and team development (10 items); staff and care delivery (six items); technology and care initiatives (six items); financial and service management (six items); leadership and clinical practice (11 items); patient safety and risk management (nine items); and standards of care (eight items).
Sample questions included the following: “Assess the significance of recognizing the influence of your actions on others,” “Evaluate the importance of acquiring, analyzing, and responding to feedback regarding your leadership approach,” “Consider the importance of reflecting on how nursing/midwifery decisions affect the overall healthcare organization,” and “Determine the importance of ensuring that written clinical procedures and policies are reviewed and updated in line with evidence-based practices.”
The CLeeNA was developed based on current literature concerning nursing and midwifery leadership and demonstrated both face and content validity, as reported by Mc Carthy et al. (2019a). A comprehensive literature review and the insights of an expert panel supported the scale's validity. The CLeeNA scale demonstrates an adequate reliability coefficient for the whole scale; it was 0.98 (Table 1), which is higher than the 0.89 reported in the original scale (Mc Carthy et al., 2019a, 2019b). Reliability coefficients were also reported in detail for the CLeeNA subscales (Table 1); they were all high, similar to Mc Carthy et al. (2019a, 2019b).
The Safety Climate Survey (SCS)
The SCS is commonly employed to evaluate the SC among nursing professionals, with an increasing body of evidence supporting its validity and reliability (Sexton et al., 2006). Professor Sexton granted permission to utilize the SCS. The 19-item SCS is rated on a 5-point Likert-type scale, where 1 signifies strong disagreement, 2 indicates slight disagreement, 3 represents neutrality, 4 denotes slight agreement, and 5 reflects strong agreement, with an additional option of 6 for “not applicable.” Items rated as 6 were excluded from the final analysis. Item 18 was reverse scored, stating, “Personnel frequently disregard rules that are established for this clinical area.” A score of 4 or higher suggests positive perceptions of the SC, while a score of three or lower indicates negative perceptions (Sexton et al., 2006).
The scale demonstrates adequate psychometric properties, including those of the translated versions (Gehring et al., 2015). The reliability of the translated SCS is confirmed, with Cronbach's Alpha values of 0.86 for German and 0.84 for French. In the current study, the reliability coefficient of the SCS was 0.93 (Table 1), which is higher than the 0.84 reported in the French version by Gehring et al. (2015), and also higher than the original English version reported by Sexton et al. (2006). This suggests strong internal consistency of the instrument in the present sample.
Data Analyses
Means, standard deviations, standard errors, numbers, and frequencies were reported for the sample's variables according to the level of measurement, using SPSS (Version 25; IBM, 2017). Data were tested for normality using the Shapiro–Wilk test prior to analysis. Shapiro–Wilk results were acceptable for both scales: CLeeNs (W = 0.962, p = .064) and SC (W = 0.984, p = .078). No interventions were taken to handle missing data.
The total mean score of the perceived CLeeNs and SC was used to decrease Type I error. The total mean score and the individual items of the perceived CLeeNs (independent variable) and SC (dependent variable) were compared between RNs and nurse managers using a t-test, and sample characteristics were compared using chi-square. Finally, Cronbach's alpha for the CLeeNA and SCS instruments and means and standard deviations were generated for the overall scale and subscales.
Results
Sample's Characteristics
In the whole sample, most nurses and nurse managers were single females aged less than 35 years, held Bachelor's degrees, worked day or rotating shifts on a full-time basis, worked in units that used primary nursing in governmental hospitals, had less than 4 years of nursing or leadership experience, and had no formal leadership/management-related education. The “mixed” was the common decision-making model and organizational structure. The chi-square showed that nurse managers were different from nurses in most sample demographics, except for time commitment, area of work, and the reported decision-making style in their area of work. More details about sample characteristics are presented in Table 2.
Sample's Characteristics (n = 391).
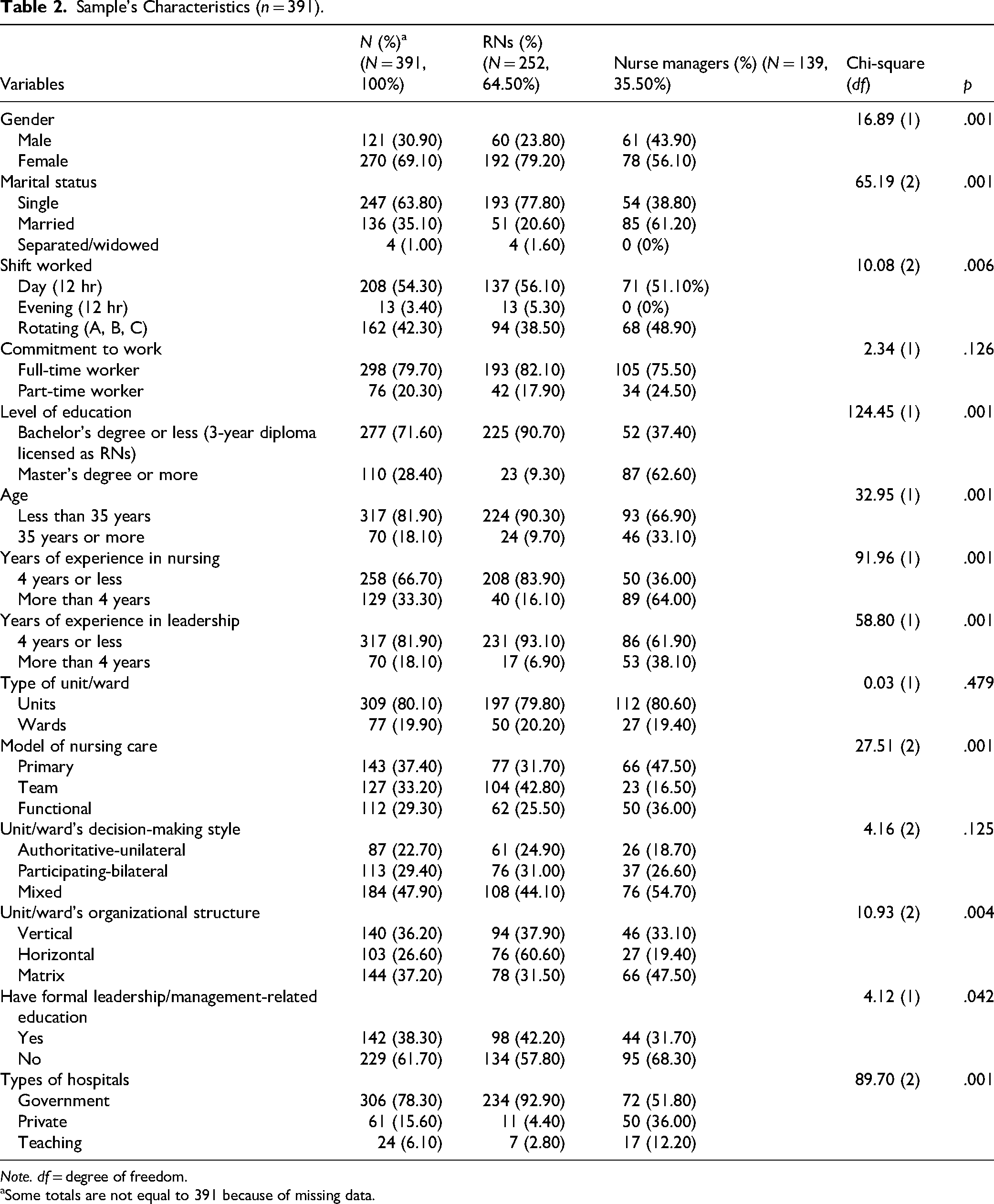
Note. df = degree of freedom.
Some totals are not equal to 391 because of missing data.
The Perceived CLeeNs and SC
On a 7-point scale (1–3 = not important, 4 = neutral, 5–7 = highly important), the mean score of the overall scale of CLeeNs was “very important” (M = 6.05, SE = 0.072), which also applied to the seven subscales. Detailed means and standard errors for all subscales are listed in Table 1. The highest mean of the subscales was for “standards of care.” In contrast, the lowest mean of the subscales was for “financial and service management” (see Table 1). The mean score of the SCS for the total sample was 3.41 (SE = 0.032), indicating negative perceptions of the SC. Sexton et al. (2006) required a score of 4 or higher (out of 5) for a positive perception (see Table 1).
Differences in the Perceived CLeeNs
To have a comprehensive overview of the CLeeNs, the authors reported the highest and the lowest individual means in the whole sample (Table 4). The highest two means were for obtaining and acting on patient/service user feedback and experiences (M = 6.27, SD = 1.71) and monitoring clinical activities to identify both expected and unexpected risks (M = 6.24, SD = 1.62), both related to the “patient safety and risk management” subscale (M = 6.03, SD = 1.55). On the other hand, the lowest two means were for promoting staff retention (M = 5.76, SD = 2.09), related to the “staff and care delivery” subscale (M = 5.98, SD = 1.64), and ensuring compliance by staff with all required standards (M = 5.77, SD = 2.19), related to “patient safety and risk management” subscale (M = 6.03, SD = 1.55) (Table 4).
The t-tests revealed that the total mean score of CLeeNs was higher among nurse managers as compared to that of nurses (6.52 ± 1.01 vs. 5.79 ± 1.55, p = .001), which held the same trend for all subscales (see details in Table 3). T-test revealed that there were many differences in most of the individual mean scores of CLeeNA for the privilege of nurse managers (Table 4). Both nurse managers and nurses were similar in their ratings of “promoting staff retention” related to the “staff and care delivery” subscale (5.96 ± 1.96 vs. 5.64 ± 2.15, p = .138), “developing a leadership succession plan” related to the “financial and service management” subscale (6.22 ± 1.74 vs. 5.85 ± 2.04, p = .062), and “identifying areas of risk/liability” related to the “patient safety and risk management” subscale (6.24 ± 1.53 vs. 5.89 ± 2.04, p = .057) (Table 4).
Differences in the Total Mean Scores and Standard Deviations of the Perceived Clinical Leadership Needs Scale and Subscales of the Safety Climate Scale Between Nurses and Nurse Managers (n = 391).

Note. Equal variances are not assumed, SD = standard deviation; RNs = registered nurses.
Differences in the Total Mean Scores and Standard Deviations of the Perceived Clinical Leadership Needs Scale Between Nurses and Nurse Managers (n = 391).

Note. 7-point Likert scale, equal variances are not assumed. SD = standard deviation.
Differences in the Perceived SC
To have a comprehensive overview of the safety, the authors reported the highest and the lowest individual means in the whole sample (Table 5). The highest two means were related to “briefing personnel before the start of a shift (having plans for possible contingencies) is an important part of safety” (M = 3.62, SD = 0.96), and the “institution was doing more for patient safety now than it did one year ago” (M = 3.54, SD = 1.00). However, the lowest two means were related to the fact that management/leadership did not knowingly compromise safety concerns for productivity (M = 3.14, SD = 0.96) and that medical errors are handled appropriately in this clinical area (M = 3.30, SD = 1.01). The t-tests revealed that there were no significant variances in the total mean score of SC, but it was higher among nurse managers as compared to that of nurses (3.46 ± 0.64 vs. 3.38 ± 0.62, p = .252) (Table 3). The same trend took place for the individual mean scores of SC for the privilege of nurse managers (Table 5).
Differences in the Total Mean Scores and Standard Deviations of the Perceived Safety Climate Between Nurses and Nurse Managers (n = 391).
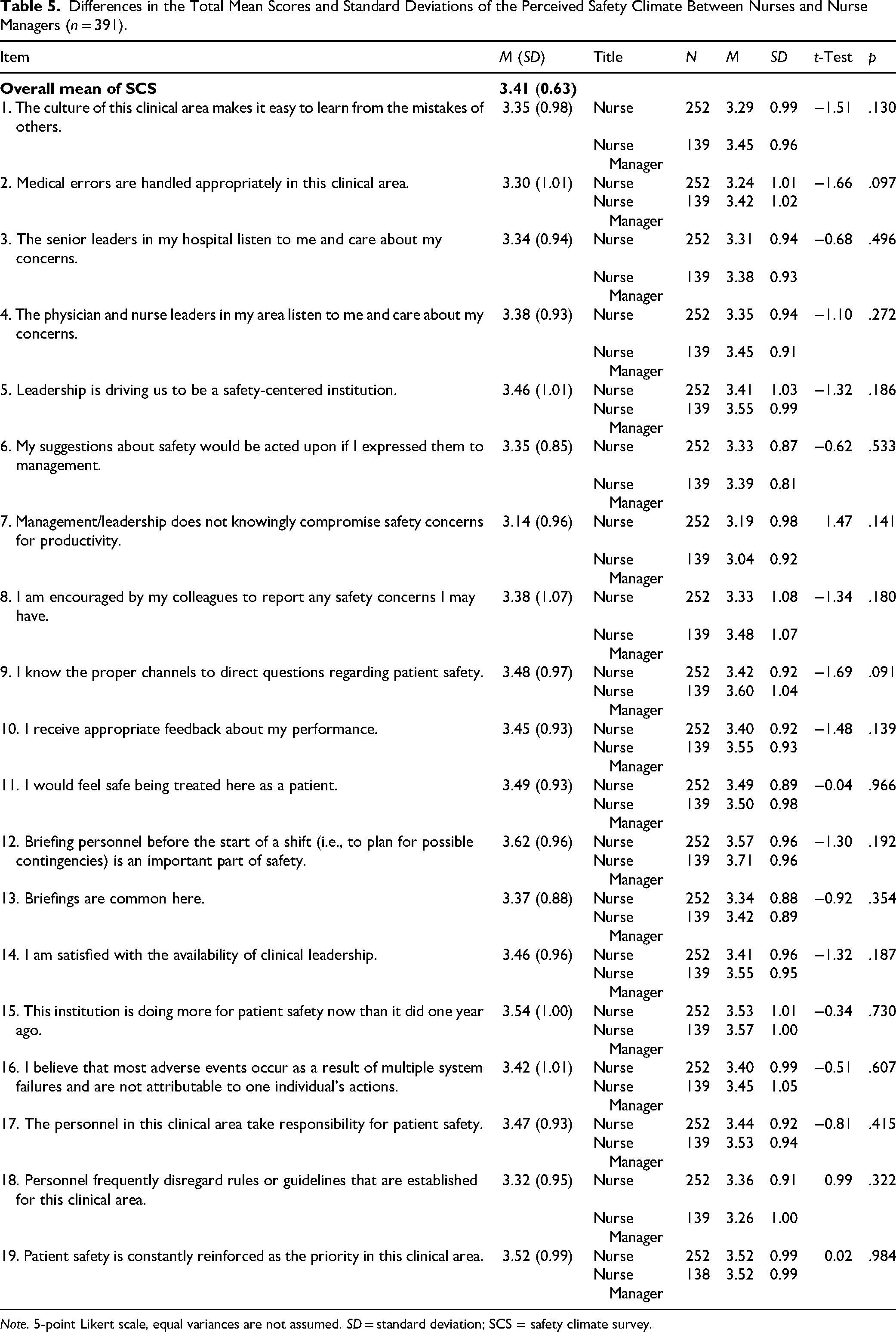
Note. 5-point Likert scale, equal variances are not assumed. SD = standard deviation; SCS = safety climate survey.
Discussion
This research examined the differences in CLeeNs and SC perceptions between nurses and nurse managers. The characteristics of the current sample align with the typical demographics of nurses and nurse managers in Jordan. It was surprising to find that a significant portion of the sample, particularly among nurse managers, indicated a lack of formal education in leadership or management. Nurse managers often attain their roles based on seniority rather than their effectiveness; this practice necessitates reform. Overall, the sample was predominantly young, with most nurse managers working in the private sector. This sector tends to invest in capable nurses, promoting them to managerial positions based on merit and effectiveness rather than seniority; such a practice should be embraced in governmental and educational hospitals as well.
While both nurses and nurse managers acknowledged the existence and importance of CLeeNs, the SC was viewed unfavorably. The authors did not anticipate this outcome; consequently, a correlation coefficient was calculated between the overall scores of the two concepts of the study, yielding an insignificant, low, and negative result (−0.023), which corroborates the initial finding of low perceived SC among participants. One possible explanation is the differing viewpoints of nurses and nurse managers. These two groups operate at different levels within the healthcare system. Nurse managers often have a wider perspective on the organization's major goals and challenges, while frontline nurses are more focused on the immediate care of their patients. This difference in focus can lead to varying perceptions of what kind of leadership is necessary and how safe the work environment feels (Ystaas et al., 2023). Another factor could be the absence of transformational leadership behaviors in practice. Transformational leadership, especially traits like Inspirational Motivation and Individualized Consideration, has been shown to promote a positive SC. If staff feel these behaviors are lacking or not strong enough, even a high recognition of leadership needs might not lead to better safety perceptions (Bass & Riggio, 2006; Zhang et al., 2025). It is also crucial to think about how these concepts were measured. The tools used might be capturing different aspects of the organizational experience. While CLeeNA looks at how important leadership competencies are perceived to be, SCS focuses on how safety culture is viewed. This mismatch in concepts could explain the weak correlation. To gain a better understanding of the relationship between CLeeNs and SC, future studies should consider using qualitative methods, longitudinal studies, and mixed-method approaches.
It is important to highlight that the healthcare landscape in Jordan is undergoing rapid transformation, characterized by limited resources, a nursing shortage, an increase in chronic diseases, and numerous demanding quality and accreditation initiatives. Additionally, nurses’ salaries in Jordan are generally low, compounded by a variety of leadership styles, particularly the autocratic approaches of older nurse managers still active in the field; these factors may contribute to the negative perceptions of the SC reported by the sample.
Finally, cultural norms, values, and expectations play a significant role in shaping perceptions of leadership and SC. In collectivist societies such as Jordan, some studies suggest that hierarchical structures and deference to authority are more common (Huang et al., 2024). These cultural tendencies may influence how leadership roles are assigned and how staff interact within organizational hierarchies (Huang et al., 2024). For example, there may be a tendency to prioritize seniority over merit in leadership appointments, which could discourage open communication and make staff hesitant to voice safety concerns (Huang et al., 2024). However, such claims should be interpreted with caution and supported by further empirical research within the local context. Unfortunately, this dynamic can negatively impact SC ratings and limit psychological safety. Traits typical of transformational leadership, such as inspirational motivation and individualized consideration, may be interpreted differently according to cultural expectations around communication and independence. Given Jordan's rapidly modernizing healthcare system, these cultural aspects could contribute to the low SC scores we have observed and the disconnect between leadership needs and safety outcomes (Huang et al., 2024).
Application of the Transformational Leadership Theory
Applying the Transformational Leadership Theory in light of the current findings shows that the differences in CLeeNs between nurses and nurse managers fit well with the core ideas of this theory. Nurse managers are likely more in tune with the visionary and motivational sides of leadership (Zhang et al., 2025). On the other hand, the consistently low SC scores from both groups point to a potential gap in how transformational behaviors are being put into practice, especially when it comes to nurturing a culture of safety.
Taking a closer look at the current findings, Idealized Influence corresponds with the observation that nurse managers rated CL needs higher than staff nurses. This result might be because they feel a strong responsibility to lead by example and maintain care standards. On the other hand, Inspirational Motivation resonates with the differences noted in SC scores, even if those discrepancies are not statistically significant, hinting at a possible oversight in this area. A deficiency in inspirational leadership could lead to an overall negative view of the SC, as staff members may feel distanced from the organization's safety objectives (Fischer, 2016). When it comes to Intellectual Stimulation, it seems that nurse managers might be more involved in strategic thinking and innovation (Zhang et al., 2025), which helps explain why they place a higher value on leadership skills tied to service and financial management, even if that aspect received the lowest ratings overall. Lastly, the lower SC scores among nurses suggest there is a perceived lack of individualized support, which is essential for enforcing psychological safety as well as open communication (Zhang et al., 2025).
In conclusion, applying the Transformational Leadership Theory gives us a solid framework to understand the differences in CL needs and SC perceptions observed here. It emphasizes the necessity for leadership development programs that nurture the 4 Is in both nurse managers and staff nurses, ultimately aiming to enhance both leadership capabilities and the safety culture in healthcare organizations.
The Perceived CLeeNs
On a 7-point scale, the mean score of the overall scale of CLeeNs was “very important.” The subscale that received the highest mean score was “standards of care,” contrasting with (Mrayyan, 2022a, 2022b) in Jordan, where “leadership and clinical practice” ranked highest, and “staff and care delivery” in Mc Carthy et al. (2019b) in Ireland, highlighting the variations in healthcare systems. The elevated mean rating for the “standards of care” subscale is particularly encouraging in an era that prioritizes quality of care. In Jordan, numerous initiatives aimed at improving quality and accreditation are currently underway across various sectors, including hospitals. In contrast, the subscale with the lowest mean score in this study was “financial and service management,” which is consistent with the findings of Mc Carthy et al. (2019b) and Mrayyan (2022a, 2022b). This outcome is expected, as nursing staff generally leave budgetary decisions to higher management, regardless of the country.
The two highest means identified were the collection and utilization of patient/service user feedback and experiences, as well as the oversight of clinical activities to detect both anticipated and unanticipated risks, which pertain to the “patient safety and risk management” subscale; existing studies corroborate these findings. Gathering patient feedback enables healthcare providers to comprehend patient needs and experiences better, thereby fostering a more patient-centered approach to care, as supported by Wong et al. (2020) in their comprehensive systematic review. Also, the monitoring of clinical activities is crucial for the early assessment and management of potential risks, which is vital for upholding high standards of patient safety, as noted by Niv and Tal (2024) in their recent book chapter. The processes of obtaining patient feedback and monitoring clinical activities are instrumental for nurse managers in cultivating a safe environment within their units or wards (consistent with Mudd et al. (2023) across Australia, Denmark, and New Zealand.
Conversely, the two lowest means pertain to the promotion of staff retention within the “staff and care delivery” subscale and the assurance of staff compliance with all necessary standards in the “patient safety and risk management” subscale. The low mean associated with promoting staff retention indicates potential difficulties in maintaining staff satisfaction and engagement in their roles. Thus, it is critical to use actionable leadership interventions, such as improving leadership styles, including team leadership, and refining staffing policies (similar to Singh et al. (2024) in the United Arab Emirates (UAE). A strategic political approach is necessary to tackle the issue of nursing staff retention, which Felder et al. (2024) refer to as “job crafting” in the Netherlands. This retention strategy aims to develop meaningful roles for nursing personnel while also reorganizing, revaluing, and repositioning the nursing profession, which could be applicable to nursing staff in Jordan. Additionally, the low average concerning compliance with required standards indicates potential shortcomings in following safety protocols and risk management practices. Such an inadequate level of compliance may contribute to the observed decline in the SC within the current sample, as adherence to safety protocols and risk management is essential for fostering a positive safety environment (supported in Niv & Tal, 2024); such a problem is global.
The findings from the t-test analysis revealed that nurse managers achieved a significantly higher mean score in CLeeNs compared to their nurses. This trend was evident across all subscales and corroborated the research findings of Hassan et al. (2020) in Egypt, Mc Carthy et al. (2019b) in Ireland, and Mrayyan et al. (2022a, 2022b) in Jordan. Nurse managers need to embody leadership qualities, acting as role models for their nursing teams and cultivating an environment conducive to learning and support (aligned with Mc Carthy et al., 2019b). The beneficial effects of nurse managers on patient care in clinical settings are well-established (supported by Hassan et al., 2020; Mc Carthy et al., 2019a, 2019b). This influence plays a crucial role in improving patient safety and effective risk management, as evidenced by decreases in the use of restraints, medication errors, and patient mortality rates (as reported by Mrayyan et al., 2022a, 2022b). To achieve positive outcomes for both nurses and patients, nurse managers should prioritize the empowerment of clinical nurses’ leadership skills (proposed by Hassan et al., 2020), which can be initiated through the encouragement of staff development and collaborative teamwork.
The t-test analysis indicated significant differences in the majority of individual mean scores of CLeeNA, reflecting the perceived advantages associated with nurse managers’ roles, such as greater authority, broader responsibilities, and increased access to leadership development opportunities, compared to staff nurses. Notably, when examining the highest and lowest two mean scores, it was found that nurse managers outperformed nurses in gathering patient feedback and overseeing clinical activities for identification purposes. This function is critical for nurse managers in patient safety and risk management-related areas, as reported by Lee et al. (2023) in their systematic review. As anticipated, nurse managers also demonstrated superior performance in promoting staff retention within the “staff and care delivery” subscale and ensuring that staff adhered to all necessary standards related to the “patient safety and risk management” subscale, as corroborated by the comprehensive international systematic review of Lee et al. (2023) and the study of Singh et al. (2024) in the UAE.
Nurse managers and nurses demonstrated similar assessments regarding “promoting staff retention” within the “staff and care delivery” subscale, “developing a leadership succession plan” in the “financial and service management” subscale, and “identifying areas of risk/liability” related to the “patient safety and risk management” subscale. These results underscore a shared focus among nursing professionals on staff retention (Vizor, 2023, in Canada), innovative leadership (Vizor, 2023), and liability issues (Lee et al., 2023). Together, these three factors play a crucial role in fostering an “SC” in hospitals (Lee et al., 2023), which is not limited to developed countries and can be applied in developing countries as Jordan.
The Perceived SC
On a 5-point scale, the average score of the SCS for the entire sample was below four, reflecting unfavorable views of the SC, and such negative perceptions of the SC are overwhelming and require immediate intervention. It is well-documented that a poor SC increases the likelihood of workplace incidents. Workers in unsafe environments are more likely to experience stress, dissatisfaction, and turnover (Aslan et al., 2025
The above result is akin to the findings of Mrayyan, AL-Atiyyat et al. (2023a) in Jordan. Such a negative perception of the SC can hinder efforts to enhance safety outcomes, leading to workplace incidents due to decreased compliance with safety protocols and an increase in risk-taking behaviors among staff (consistent with Arzahan et al. (2022) in a recent systematic review). The authors reported that nursing personnel with negative views of the SC are likely to experience higher levels of job-related stress and turnover. Urgent measures are necessary to rectify these harmful perceptions of the SC. Many interventions can be implemented to improve the SC in clinical environments, including (1) Leadership commitment, where clinical leaders must visibly commit to fostering a positive SC through open communication, a practice known as clinical safety leadership, synthesized by Jiang et al. (2024) in their recent bibliometric literature review. (2) Employee involvement, which involves actively engaging nursing staff in safety initiatives, supported by thorough training and education on current safety protocols, incident reporting and analysis, as well as regular audits. (3) The creation of a system that rewards safe behaviors will further strengthen the SC (Arzahan et al., 2022; Jiang et al., 2024). These results are strong and can be global, as they emerged from a comprehensive systematic review (Arzahan et al., 2022) and a bibliometric literature review (Jiang et al., 2024).
The two highest means were associated with the statements, “briefing personnel before the start of any shift is a milestone in safety” and “the institution is currently doing more for patient safety than it did a year ago.” However, perceptions of “briefing personnel before the start of shifts” were negative among the current nurses and nurse managers, which contrasts with the findings of Glarcher et al. (2022) in Austria. This negative sentiment indicates dissatisfaction among nurses and nurse managers regarding the hospital administrators’ responses to their expressed concerns. In fact, the present sample indicated that management and leadership did not intentionally compromise safety for productivity, which was one of the lowest two means, as supported by Glarcher et al. (2022). Furthermore, inadequate management and leadership in this study poorly addressed medical errors in clinical settings, highlighting the need for effective clinical safety leadership (Jiang et al., 2024). Consequently, it is not surprising that nurses and nurse managers believe their hospitals are currently making greater efforts toward patient safety; negativity is contagious.
T-tests indicated that there were no significant differences in the overall and individual mean scores of the SC. However, nurse managers reported higher scores compared to nurses. Nurse managers generally have a more favorable perception of the SC than their nursing counterparts, which aligns with the findings of Glarcher et al. (2022) in Austria. Nurses who engage directly with patients tend to have more critical views regarding aspects related to the SC.
Strengths and Limitations
This study utilized validated CLeeNA and SCS instruments with high reliability scores and included a diverse sample of nurses and nurse managers from multiple hospital types, enhancing internal validity. The comparative design provided valuable insights into role-based differences in leadership needs and SC perceptions. Finally, the integration of the Transformational Leadership Theory as a guiding framework provided a strong theoretical foundation for interpreting the findings and linking leadership behaviors to safety outcomes.
However, this research acknowledges several limitations and suggests future research directions. Generalizability is restricted due to a non-random, cross-sectional sample limited to Jordan, introducing selection and response biases (Polit & Beck, 2019). To improve representativeness, future studies should incorporate diverse demographics and stratified sampling methods. Cross-sectional designs also present challenges, including causality issues, temporal ambiguity, and a limited perspective (Polit & Beck, 2019). Addressing these requires complementing findings with longitudinal studies and implementing control measures to strengthen validity.
Because of its comparative nature, the study brings to light some valuable perspectives on how nurses and nurse managers view CLeeNs and SC; however, it misses the chance to look into how demographic factors influence these viewpoints. Variables such as years of experience, the type of hospital, educational background, and departmental setting could have provided important context if they were analyzed through a multivariate regression approach. By skipping this kind of analysis, the study might not capture some key details that affect how CLeeNs and SC are perceived in real clinical settings. Future research should consider utilizing regression models or structural equation modeling to explore these connections further and gain a richer understanding.
Online surveys may exclude less tech-savvy individuals, affecting data quality. Misinterpretations and disengagement further complicate findings. To tackle this challenge, we put a few strategies into place: The CLeeNA and SCS tools were crafted with user-friendly designs, straightforward instructions, and minimal technical requirements, making sure that everyone, regardless of their digital skills, could easily join in. Additionally, the survey was mobile-friendly, so participants could fill it out conveniently on their smartphones or tablets that healthcare workers often use during their shifts or breaks. Finally, the research should explore links between CL perceptions and actual behaviors, addressing challenges such as poor teamwork, reluctance to change, weak commitment at higher levels, role conflict, and recognition gaps (Guibert-Lacasa & Vázquez-Calatayud, 2022; Huang et al., 2024). As directed by the negative correlation between the studied concepts, future studies should explore why CLeeNs are not translating into improved SC.
Implications for Future Research, Practice, Policy, and Education
The current study has several implications. In practice, nurses and nurse managers are in positions to make a real difference in CL and SC. By stepping into roles as advocates, mentors, educators, and quality managers, they can significantly impact patient outcomes and shape organizational culture. Nurses and nurse managers’ hands-on experience allows them to spot gaps, suggest solutions, and ensure that both patient and staff perspectives are included in decision-making. Nurse managers should prioritize training programs that focus on transformational leadership, highlighting the 4Is: Idealized Influence, Inspirational Motivation, Intellectual Stimulation, and Individualized Consideration. Nurse managers must evaluate safety culture on a regular basis, using validated tools like the SCS, and tailor their leadership strategies based on the findings. With their higher scores in CLeeNs and standards of care, nurse managers should spearhead initiatives aimed at enhancing patient safety, improving quality, and boosting staff engagement (Mrayyan et al., 2023b). They also need to foster interprofessional teamwork and maintain open lines of communication to promote psychological safety and minimize errors (Buck et al., 2023; Raso & Fitzpatrick, 2021).
The correlation between CLeeNs and SC was low and negative at −0.023; thus, healthcare organizations need to understand that recognizing leadership needs is just the beginning. To genuinely enhance SC, these needs must be transformed into actionable steps—through structured leadership development, mentorship, and active engagement at the frontline. Nurse managers, who have identified greater leadership needs, should be empowered to lead safety initiatives and cultivate a culture of transparency and accountability.
Policymakers are essential in shaping the future of nursing leadership and fostering a safety culture. A pivotal step towards achieving this is the formal acknowledgment of CL as a core competency in professional nursing practice. This competency implies that leadership skills need to be woven into licensing requirements and performance evaluations, instead of being viewed as optional extras. Promotion practices in nursing leadership often rely on seniority rather than effectiveness, a trend that has been observed across various healthcare systems (Algunmeeyn et al., 2024). This approach, while rooted in tradition and organizational hierarchy, may inadvertently overlook individuals with strong leadership potential but fewer years of service. Such practices can hinder innovation, reduce motivation among high-performing early-career nurses, and perpetuate outdated leadership models. It is time to rethink promotions, based on effectiveness rather than seniority (Mrayyan et al., 2023b). Implementing merit-based promotion systems, grounded in demonstrated leadership competencies, performance outcomes, and peer evaluations, could lead to more dynamic, responsive, and effective leadership within healthcare organizations. Such a shift would not only celebrate exceptional leadership but also encourage ongoing professional growth. Another significant issue we face is nurse retention. Policymakers must address “financial barriers” by offering competitive compensation packages. By doing so, we can help stop the drain of skilled nurses to other areas and ensure that experienced professionals remain in the workforce, where their leadership and expertise are invaluable (Buck et al., 2023).
In education, nursing educators must integrate CL into nursing programs. This integration is crucial for ensuring that future nurses provide effective and safe care (Raso & Fitzpatrick, 2021). Educators must use real-world scenarios to teach essential skills like decision-making and communication; these skills have a direct effect on SC. Such hands-on experiences help connect theoretical knowledge with clinical practice. Finally, mentorship should be encouraged as it plays a major role in nursing education. Experienced nurses must mentor the newer staff; this would boost leadership development and strengthen safety practices, and nurture a supportive, collaborative environment (Buck et al., 2023).
Conclusion
CL is essential for a safe climate; however, little is known about how nurses and nurse managers differ in their perceived CLeeNs in practice as well as their perceptions of SC. As perceived as “very important,” CLeeNs and CL should be promoted and developed constantly. The low perceived SC is alarming and mandates immediate intervention at all leadership levels.
Given the negative correlation observed between the concepts studied, future research must delve into why CLeeNs are not translating into an improved SC. Healthcare organizations must understand that merely pinpointing leadership needs is just the start. To really boost the SC, those identified needs have to be transformed into tangible actions, which means organized leadership development, mentorship, and getting actively involved at the frontline. Nurse managers, who are aware of the increased leadership needs, should be empowered to lead safety initiatives and create a culture rooted in transparency and accountability.
Supplemental Material
sj-doc-1-son-10.1177_23779608251404084 - Supplemental material for A Cross-Sectional Study of Clinical Leadership Needs and Safety Climate: Differences Between Nurses and Nurse Managers
Supplemental material, sj-doc-1-son-10.1177_23779608251404084 for A Cross-Sectional Study of Clinical Leadership Needs and Safety Climate: Differences Between Nurses and Nurse Managers by Majd T. Mrayyan and Jamal M.A. Ismail in SAGE Open Nursing
Footnotes
Author Note
The authors listed meet the authorship criteria according to the latest guidelines of the International Committee of Medical Journal Editors, and the authors agree with the manuscript. The authors have approved the content before submission or resubmission. The authors have no conflicts of interest and no funding source.
Acknowledgments
The researchers acknowledge the input of all subjects who participated in the study.
Ethics Approval and Consent to Participate
All needed approvals were obtained before data collection, including IRB. The Hashemite University, Jordan, approved the study. IRB No. 1,2/1/2020/2021, dated October 18, 2020. In the invitation letter, nurses were informed that their participation is their consent to participate in the study.
Consent for Publication
This article includes data obtained from individual participants. Written informed consent for publication was obtained from all participants. All authors hereby give their consent for the publication of the article, including all associated data published by Sage Publications.
Author Contributions
Majd T. Mrayyan: conceptualization, abstract, methodology, investigation, data analysis and writing, limitations, original draft preparation, writing, review, editing, and supervision. Jamal M. A. Ismail: writing, reviewing, and editing of discussion and implications.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
During the preparation of this work, the authors used Grammarly to edit the language. After using this tool, the authors reviewed and edited the content as needed and took full responsibility for the content of the publication.
Availability of Data and Materials
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Patient or Public Contribution
There was no patient or public contribution, as the sample included nurses recruited from different hospitals.
Reporting Method
This study followed the STROBE checklist for cross-sectional studies.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.