
Abstract
Abstract
Despite the documented clinical efficacy, the injection of subcutaneous heparin can be associated with adverse drug reactions including bruising at the injection site. This study sought to systematically assess current evidence regarding the effect of cold application as a fundamental nursing intervention on the occurrence and size of bruising at the injection site in patients receiving subcutaneous heparin. A systematic review and meta-analysis of randomized controlled trials and quasi-experimental studies was performed. Web of Knowledge, PubMed (including MEDLINE), Scopus, Embase, Cochrane library, gray literature, and cross‐referencing from reference lists were searched from 2000 to 2019. Quality of selected studies was assessed using the Cochrane risk of bias appraisal tool for randomized controlled trials and the JBI MASTARI appraisal tool for quasi-experimental studies. The search yielded 3,220 articles, but consideration of inclusion criteria led to final selection of 9 articles. The meta-analysis showed that cold application significantly reduced the relative occurrence of bruising at the subcutaneous heparin injection site by 40% (relative risk, 0.60; 95% confidence interval [0.39, 0.91]) and reduced the bruising size (standardized mean difference, −2.78; 95% confidence interval [−4.34, −1.22]). Cold application as a fundamental nursing intervention can be an effective intervention to prevent adverse drug reactions at the injection site in terms of the occurrence and size of bruising in patients receiving subcutaneous heparin.
Keywords
Introduction
The safe prescription and administration of medicines is an essential part of safe nursing care (Lehne, 2013). The administration of some medicines, especially subcutaneous injections, poses greater responsibilities on clinical nurses to assess related adverse drug reactions (ADRs) and the quality and safety of medication process (Hunter, 2008). ADR is a noxious and unintended response to a drug, which can occur at doses normally used for therapeutic purposes (International Conference on Harmonisation, 1996).
Subcutaneous heparin is administered extensively to patients who need anticoagulant medicines to reduce the harmful clot formation during hospitalization (Ansell et al., 2008). It can create a more predictable anticoagulant effect, increase bioavailability from the subcutaneous site of injection, and has less frequent dosing requirements. Also, its simple subcutaneous administration permits short- and long-term prescriptions (Katzung, Masters, & Trevor, 2012). However, similar to other medicine, the use of subcutaneous heparin has its own side effects and ADRs including pain at the injection site, local irritation, skin lesions, and bruising (Karch, 2012; Kuzu & Ucar, 2001; Potter & Perry, 2008; Schindewolf et al., 2009). They can result in patients’ anxiety, rejection of treatment, and distrust in nurses’ competency for medicines management (Chan, 2001; Klingman, 2000).
Cold application have various therapeutic benefits and can relieve injection-related complications of subcutaneous heparin (Kozier, Erb, Berman, Snyder, & Frandsen, 2016; Ross & Soltes, 1995). Bruising has been reported as one of the most frequently observed ADRs and side effects of subcutaneous heparin injection. For example, it is estimated that 26% to 90% of low-molecular-weight heparin injections cause bruising at the injection site (de Campos, da Silva, Beck, Secoli, & de Melo Lima, 2013). Therefore, the effect of cold application as a fundamental nursing intervention on such a complication is of great importance for improving the quality and safety of clinical practice. Studies on appropriate nursing strategies for reducing bruising associated with subcutaneous heparin injections can improve the quality of nursing care and decrease patients’ stress with the medication process (Morissette, 2015). Previous clinical trials in nursing (Amaniyan, Varaei, Vaismoradi, Haghani, & Sieloff, 2016; Avşar & Kaşikçi, 2013; Sendir, Büyükyilmaz, Çelik, & Tasköprü, 2015) have demonstrated the efficacy of cold application to reduce the occurrence of bruising at the injection site. However, some studies have reported controversial results (Kuzu & Ucar, 2001; Ross & Soltes, 1995). Given variations in the studies’ results, making a consistent conclusion on the efficacy and direction of causality between cold application and reduction of bruising at the injection site of subcutaneous heparin becomes difficult. Therefore, this study aimed to (a) systematically review the randomized controlled trials (RCTs) and quasi-experimental studies on cold application and the occurrence and bruising size of subcutaneous heparin at the injection site and (b) to carry out a meta-analysis to evaluate whether the evidence supports the effectiveness of cold application as a conservative and fundamental nursing intervention for the reduction of bruising at the injection site.
Methods
Study Design
This was a systematic review and meta-analysis of RCTs and quasi-experimental studies comparing the application of cold to the injection site versus no application of cold on bruising in patients receiving subcutaneous heparin. We adopted the Preferred Reporting Items for Systematic Reviews (PRISMA) and Meta-Analyses statements as the equator to carry out this review (Moher, Liberati, Tetzlaff, Altman, & PRISMA Group, 2009).
Search Strategy
Online platforms and databases of Web of Knowledge, PubMed (including MEDLINE), Scopus, Embase, and Cochrane library were searched for all relevant studies published from January 2000 to March 2019, using the Boolean search strategy (Table 1). Also, gray literature and cross‐referencing from the bibliographies of included studies were searched to extend the search coverage.
Search Strategy of This Review.

Eligibility Criteria
According to the PICOS framework which considers the characteristics of Participants, Intervention, Comparison, Outcomes, and Study design, those studies that met the following criteria were selected for data analysis: (a) RCTs or quasi-experimental designs (allocation of patients into different groups that was not truly random such as allocation by the clinical setting), (b) patients were administered the subcutaneous heparin injection, (c) application of cold to the injection site, (d) control group received the no cold application intervention, and (e) description of ADRs as the primary outcome in terms of the occurrence and size of bruising. Studies published in languages other than English or Farsi were excluded.
Data Extraction
Two of the authors (S. A. and A. G.) independently screened each retrieved study as definitely or potentially meeting the inclusion criteria and obviously not meeting the inclusion criteria. Also, they read the full text of articles in terms of definitely or potentially meeting the criteria for eligibility. A pre-piloted data extraction table was used to extract the studies’ data regarding the author’s name, year of publication, country, type of trial, sample size, age range of subjects, type of subcutaneous heparin injection, cold application, and examined outcomes. Disagreements between the authors were resolved through discussions and consultation with a third author (M. V.). The details of the selection process are displayed in Figure 1.

The selection process according to the PRISMA flow diagram.
Risk of Bias Assessment
The Cochrane risk of bias appraisal tool was used to assess the quality of RCTs. It addressed six specific methodological domains, and each domain was rated as unclear bias risk, low bias risk, and high bias risk (Higgins et al., 2011). Furthermore, the JBI MASTARI appraisal tool for experimental studies was used for the appraisal of quasi-experimental studies (Joanna Briggs Institute, 2006). Quality assessment was conducted independently by two authors (S. A. and A. G.), and potential disagreements were resolved through discussions and consultation with a third person (M. V.).
Statistical Analysis
For the meta-analysis of ADRs in terms of the occurrence and size of bruising at the subcutaneous heparin injection site, the relative risk (RR) and standardized mean difference (SMD) along with 95% confidence intervals (CIs) were calculated for each study. The fixed-effects model or the random-effect model in case of heterogeneity was used to conduct pooled analyses. Subgroup analysis was conducted based on the study design. Homogeneity was examined using the DerSimonian and Laird method (DerSimonian & Laird, 1986). The I2 statistic was used to evaluate heterogeneity among selected studies. Although there can be no absolute rule for when heterogeneity becomes important, the Cochrane Handbook for Systematic Reviews of Interventions (Higgins & Green, 2011) tentatively suggests that the adjective of substantial heterogeneity for I2 values ranges from 50% to 90%. Therefore, heterogeneity was assumed when I2 was over 50%. For all cases, forest plots were drawn. The forest plot summarized information on individual studies and the observed effects of the intervention along with the overall result. Also, if standard deviation was reported zero, it was considered 0.5 for further analysis (Higgins & Green, 2011; Li et al., 2016). When the analyzing ratio was measured in the binary variable of bruising incidence, the log ratio with its standard error was used as inputs to the analysis (Harris et al., 2008). Threshold for statistical significance was set at 0.05. All statistical analyses were performed using the STATA software (version 14 MP).
Results
The search strategy led to the identification of 3,811 articles, of which 3,786 articles were duplicated or did not meet the inclusion criteria and hence resulted in the selection of 25 articles. After full-text appraisal, nine articles remained: five were RCTs and four were quasi-experimental studies. The characteristics of all nine studies were summarized in Table 2.
Summary of the Characteristics of the Selected Studies.

RCT = randomized controlled trial; NA = not applicable.aReported sample size may not be equal to the total number of included patients in the corresponding study. Other groups that received a different intervention were not considered.
Occurrence of Bruising at the Injection Site
Six studies (Amaniyan et al., 2016; Avşar & Kaşikçi, 2013; El-Deen & Youssef, 2018; Kuzu & Ucar, 2001; Sendir et al., 2015; Varghese, Walia, Sharma, & Kaur, 2006) consisting of four RCTs and two quasi-experimental studies reported the occurrence of bruising as the study outcome. Bruising was assessed at different time intervals in different studies, including 12, 48, and 72 hours. Since the 48-hour measurement was reported in all of the included studies, occurrence of bruising for the 48-hour interval was analyzed. Bruising was identified by observing any discoloration of the injection site such as pink, red, blue, purple, pale green, yellow, and brown (El-Deen & Youssef, 2018).
Since no overall heterogeneity was observed in the RCTs (p = .898, I2 = 0.0%), a fixed-effects model was employed. The subgroup analysis was conducted based on different study designs. According to the pooled analysis of RCTs, the cold application intervention reduced the occurrence of bruising at the injection site by 33%. On the other hand, the two quasi-experimental studies were highly heterogeneous (p = 0, I2 > 90%). The meta-analysis of the quasi-experimental studies demonstrated that cold application had no statistically significant effect on the occurrence of bruising. In general, cold application was associated with a decreased risk of bruising at the injection site compared with the control group (RR, 0.60; 95% CI [0.39, 0.91]; Figure 2).

Meta-analysis of the bruising incidence in the RCTs (based on the fixed effect model) and the quasi-experimental studies (based on the random-effect model). RCT = randomized controlled trial; RR = relative risk; CI = confidence interval.
Bruising Size
All of the included studies reported the bruising size as the outcome. The bruising size was assessed using a transparent millimeter ruler or film in mm2 (measures in cm were converted to mm). As of the bruising occurrence outcome, 48-hour measurements were analyzed. All studies reported the quantitative measure of the bruising size, except the Varghese et al.’s study (2006). This outcome was reported as a categorical variable. Also, El-Deen and Youssef (2018) reported it in different units and did not provide more data to be included in the data analysis. Such heterogeneities reduced the comparability of the results of these two studies with other trials. Therefore, only the description of their results was provided.
The subgroup analysis was conducted due to different study designs. Regarding four RCTs (Amaniyan et al., 2016; Kuzu & Ucar, 2001; Sendir et al., 2015; Shijila & Tresa, 2016), pooled results showed a statistically significant effect of the intervention (SMD, −5.27; 95% CI [−9.81, −1.63]). In addition, for three quasi-experimental studies (Avşar & Kaşikçi, 2013; Batra, 2014; Rupam, Sheoran, & Sharma, 2018), pooled results demonstrated that the cold application group had a smaller bruise size compared to the control group (SMD, −1.12; 95% CI [−1.72, −0.11]). Overall, the pooled analyses of RCTs and quasi-experimental studies revealed that the intervention group had a smaller bruising size compared with the control group (SMD, −2.78; 95% CI [−4.64, −1.22]; Figure 3). Sensitivity analysis for the type of cold application (pre- or postinjection) was performed by excluding the two studies, in which cold application was administered before the injections (Avşar & Kaşikçi, 2013; Batra, 2014). The sensitivity analyses still supported the effectiveness of the intervention (SMD, −2.02; 95% CI [−3.36, −0.18]). Varghese et al. (2006) concluded that the use of moist ice pack resulted in a significant lower bruise size compared to the control group. El-Deen and Youssef (2018) found that the two intervention groups who received cold application had a lower size of bruising than the control group.

Meta-analysis for the bruising size in the RCTs (based on the random effect model) and the quasi-experimental studies (based on the fixed-effect model). RCT = randomized controlled trial; SD = standard deviation; SMD = standardized mean difference; CI = confidence interval.
Risk of Bias
The results of the assessment of risk of bias in the RCTs and quasi-experimental studies were reported in Tables 3 and 4.
Risk of Bias in the Randomized Control Trials.

 = low risk of bias;
= low risk of bias;  = high risk of bias;
= high risk of bias;  = unclear risk of bias.
= unclear risk of bias.
Risk of Bias in the Quasi-Experimental Studies.
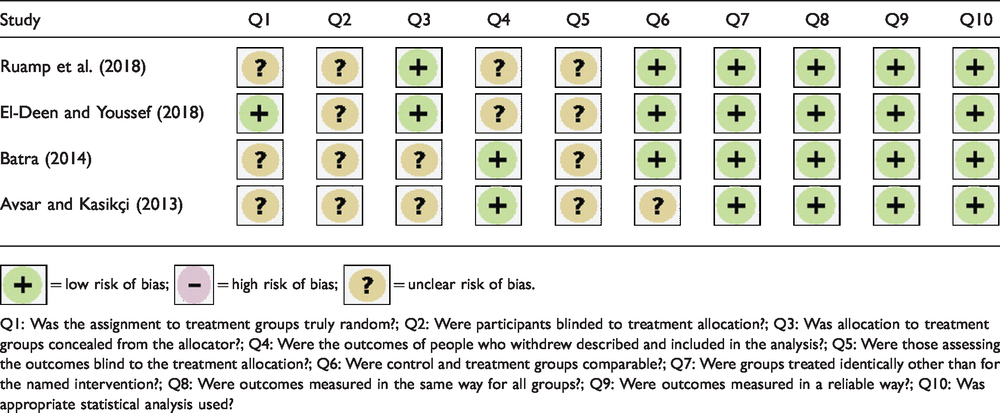
= low risk of bias; = high risk of bias; = unclear risk of bias.
Q1: Was the assignment to treatment groups truly random?; Q2: Were participants blinded to treatment allocation?; Q3: Was allocation to treatment groups concealed from the allocator?; Q4: Were the outcomes of people who withdrew described and included in the analysis?; Q5: Were those assessing the outcomes blind to the treatment allocation?; Q6: Were control and treatment groups comparable?; Q7: Were groups treated identically other than for the named intervention?; Q8: Were outcomes measured in the same way for all groups?; Q9: Were outcomes measured in a reliable way?; Q10: Was appropriate statistical analysis used?
Random sequence generation
Among the five RCTs, only one study (Kuzu & Ucar, 2001) lacked the description of the random sequence generation. However, most of the included quasi-experimental studies were unclear in terms of the process of assignment to treatment groups (Avşar & Kaşikçi, 2013; Batra, 2014; Rupam et al., 2018).
Allocation concealment
There were differences in the allocation concealment between the studies. Five studies (Amaniyan et al., 2016; El-Deen & Youssef, 2018; Rupam et al., 2018; Shijila & Tresa, 2016; Varghese et al., 2006) adequately described allocation concealment from the allocators. Therefore, they were considered at a low risk of bias. Four others did not describe it clearly (Avşar & Kaşikçi, 2013; Batra, 2014; Kuzu & Ucar, 2001; Sendir et al., 2015).
Blinding
Amaniyan et al. (2016) reported that the assessor of the bruising size was blinded and had no information about the patient’s group within the process of study. However, none of the included studies explained the blinding of patients. The reason could be the identity of the intervention that hindered the blinding of patients.
Incomplete outcome data
Five studies (Amaniyan et al., 2016; Avşar & Kaşikçi, 2013; Batra, 2014; Kuzu & Ucar, 2001; Varghese et al., 2006) presented a suitable description of patients who withdrew from the studies. They were regarded to be at a low risk of bias. In one study (Sendir et al., 2015), 6.25% dropouts were found with no explained intention-to-treat analysis. So, it might lead to a high risk of bias.
Selective outcome reporting
All studies reported all expected outcomes and were supposed to have a low risk of bias.
Other sources of bias
Some characteristics of the injections of subcutaneous heparin such as needle gage and air lock were not described in the included studies, which could influence their outcomes.
Publication Bias Assessment
To assess the funnel plot asymmetry test, at least 10 studies should be included in the review (Higgins & Green, 2011; Mohammady, Janani, & Sari, 2017). Since the number of included studies in this meta-analysis violated this assumption, it was impossible to prepare a funnel plot.
Discussion
The subcutaneous injection of heparin is a common and fundamental clinical intervention in various healthcare settings performed by clinical nurses. However, it is accompanied with a number of ADRs and side effects, of which bruising at the injection site is more frequent (de Campos et al., 2013). To minimize it, it is incumbent to nurses to investigate the potentially effective interventions such as cold application to reduce it as much as possible and improve the quality and safety of patient care. Noninvasive and safe strategies that can result in less and smaller bruising at the injection site of subcutaneous heparin should be suggested by nurses to promote the safety of medicines management and prevent nonadherence to the therapeutic regime.
Summarizing Main Findings
To our knowledge, this is the first meta-analysis on the effectiveness of cold application on bruising at the subcutaneous heparin injection site. To control the probability of missing relevant data, a comprehensive search was performed to detect and retrieve articles and to evaluate the selected studies in terms of methodology and risk of bias. Due to a lack of sufficient numbers of RCTs on the study phenomenon, the authors broadened inclusion criteria and included quasi-experimental studies to this review. All studies reported the expected outcome and had a relatively low risk of bias. However, the majority of them did not report anything about the characteristics of injection of subcutaneous heparin. Therefore, it could affect on the statistical power of analysis. Overall, the significant effects of the cold application intervention on the reduction of occurrence and size of bruising at the subcutaneous heparin injection site after 48-hour follow-up compared to the control group were reported.
Mechanism
The mechanism of why cold application can reduce the bruising occurrence and its size is attributed to vasoconstriction (Kuzu & Ucar, 2001; Lynn, 2018). Cold application at the subcutaneous injection site can control bleeding through arterioles’ vasoconstriction, decrease blood flow to the affected site, and control the development of bruising through the reduction of capillary permeability and metabolic needs (Kilic & Midilli, 2008).
Previous Meta-Analysis of Bruising at the Subcutaneous Heparin Injection Site
Yi et al. (2016) pooled the results of five RCTs and three quasi-experimental studies, investigating the effect of the duration of subcutaneous injection on patients receiving low-molecular-weight heparin. They found that slow injection technique would be beneficial to the patients in terms of both the occurrence and size of bruising compared to the fast injection techniques.
Limitations of This Study
The limitations of this meta-analysis should be considered during the interpretation of findings. The presence of more RCTs could afford the researchers to provide a more in-depth insight into the study topic. Due to the nature of meta-analysis, the use of aggregated group data for calculating the effect size can ignore the effect of other potential confounding factors influencing the outcomes of interest. In addition, the heterogeneity in the duration of cryotherapy applied in the included studies could have some effects on the study outcomes. Cold application is recommended only for 5 to 10 minutes in terms of effectiveness, but cooling is considered enough (Ward, 2000).
Implications for Practice
This study provides knowledge about the prevention of bruising associated with the subcutaneous heparin injection. Accordingly, clinical nurses are suggested to use cold packs to reduce the occurrence and size of bruising associated with subcutaneous heparin injection. Implementation of this nursing intervention is inexpensive, easy to administer, and readily acceptable to patients in various health conditions even at home. Nevertheless, during the application of cold, efforts by nurses are needed to assess the patient’s response, preserve his or her privacy, and prevent possible negative consequences of cold application on the skin. Further studies are required to understand the effectiveness of cold application and cryotherapy on other health-related indicators including pain and psychological indicators.
Conclusion
According to this study, cold application can reduce ADRs in terms of the occurrence of bruising and its size at the subcutaneous heparin injection site. Therefore, cold application as a safe and fundamental nursing intervention can be used along with other caring modalities to reduce the side effects of the subcutaneous heparin administration such as bruising and hematoma. More studies are required to investigate the effects of fundamental nursing interventions on the reduction of medicines’ side effects and ADRs in line with the nurses’ role and involvement in medicine management initiatives and patient safety.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We received no financial support for the research and authorship, but publication charges were covered by Nord University.