
Abstract
Problem
Communication has been found to be central to patient safety and colleague engagement. Poor communication was identified in a Level III trauma hospital in the midwestern US between “sitters” (staff members assigned to monitor patients identified as having safety concerns) and the nurses assigned to care for those patients, including lack of a formal handoff process.
Approach
A Patient/Problem, Intervention, Comparison, Outcome (PICO) statement guided an evidence-based project and identification of an intervention to improve the handoff process. Using the evidence-based format of Situation/Background/Assessment/Recommendation (SBAR), a Patient Safety Attendant Handoff Form was developed and implemented.
Results
Initially, Registered Nurses (RNs), Licensed Practical Nurses (LPNs), or Certified Nursing Assistants (CNAs) were used as sitters, taking them away from other responsibilities. A formal position, Patient Safety Attendant (PSA), was created to perform the sitter role. The Patient Safety Attendant Handoff tool was made an official hospital form and implemented as a new standard of practice. Analysis of data from completed forms identified the top reasons for assigning a sitter were mental health and behavioral concerns. In a six-month post-implementation survey, most PSAs reported receiving adequate information about the patients during handoffs using the new form.
Conclusion
Using SBAR for the Patient Safety Attendant Handoff Form improved communication between RNs and PSAs and also enhanced communication between PSAs. A key safety feature of the form is the Recommendation section which includes “triggers to avoid,” de-escalation techniques, and things the patient enjoys. Developing a structural model from the aggregated data on the completed forms helped in analyzing the information.
Keywords
Background
A Level III trauma hospital in the midwestern US invested in a nurse residency program to support new graduates ‘transition to professional practice. The hospital is a 342-bed licensed facility that serves 15 counties in northern Iowa and southern Minnesota, and also oversees the management of seven rural hospitals in the area (MercyOne North Iowa, n.d.). The residency program followed the Vizient/American Association of Colleges of Nursing (AACN) Program design, which supports the transition to practicing nurse, the development of effective decision-making skills, and opportunities to work as a member of the interprofessional team. The program also strengthens participants ‘commitment to nursing, evidence-based practice, and engagement in the health-care organization, to inform decision making at the point of care (Vizient Inc., 2022).
In May 2021 the hospital created the position of Patient Safety Attendant (PSA) to replace the previous role of “sitter,” individuals who provided one-on-one observation of patients at high risk for self-harm or injury when previous safety methods, including use of a video-monitoring system, moving the patient closer to the nurse's station, bed alarms, and/or removing objects that the patient could use to cause injury to themselves or others, had been deemed insufficient. The acute patient care departments most often utilizing PSAs include pediatric, medical, surgical, critical care, and emergency departments. Prior to the creation of the PSA position, Registered Nurses (RNs), Licensed Practical Nurses (LPNs), or Certified Nursing Assistants (CNAs) often performed the role of sitter on other units if their unit was overstaffed; this strategy was not cost-effective and created unsafe staffing ratios for other direct patient care needs.
As a result of these concerns, the PSA role was created. A PSA is responsible for proactively ensuring patient safety, under the direction of an RN. These colleagues monitor the safety and comfort of patients who are expressing suicidal thoughts or who require frequent or continual observation and contact due to psychiatric, medical, and/or safety reasons. This new position has been successful in decreasing the number of nursing staff pulled away from other patient care needs. However, two nurse residents identified safety concerns involving lack of communication between RNs and PSAs, because of lack of a formal handoff process. The communication concerns involved:
Basic patient information (e.g. patient name, code status, medical conditions, reason for hospitalization, need for sitter, routines)
Resources (assigned nurse's name and phone number, when and how to communicate need for assistance and breaks)
Patient triggers and de-escalation methods
The nurse residency program is one year in duration; nurses meet monthly as a group with a coordinator. Each session covers a wide variety of evidence-based practice (EBP) topics. One requirement of the program is for participants to complete a quality improvement EBP project, “which supports the development of critical thinking and clinical reasoning skills” (Vizient Inc., 2022, para. 9). According to the Johns Hopkins Medicine Center for Nursing Inquiry (2022), EBP allows nurses to review literature and analyze and translate the latest evidence. The first step in any EBP project is to develop a Patient/Problem, Intervention, Comparison, Outcome (PICO) question, to determine if there is an evidence-based solution, or if more research is needed.
Methods
After the handoff communication problem was identified as a priority, the nurse residents worked as a team to complete a literature search, develop PICO questions, design and administer a survey, summarize the survey results, and integrate their findings into a standard tool for handoff communication. Figure 1 shows the progression of the project.
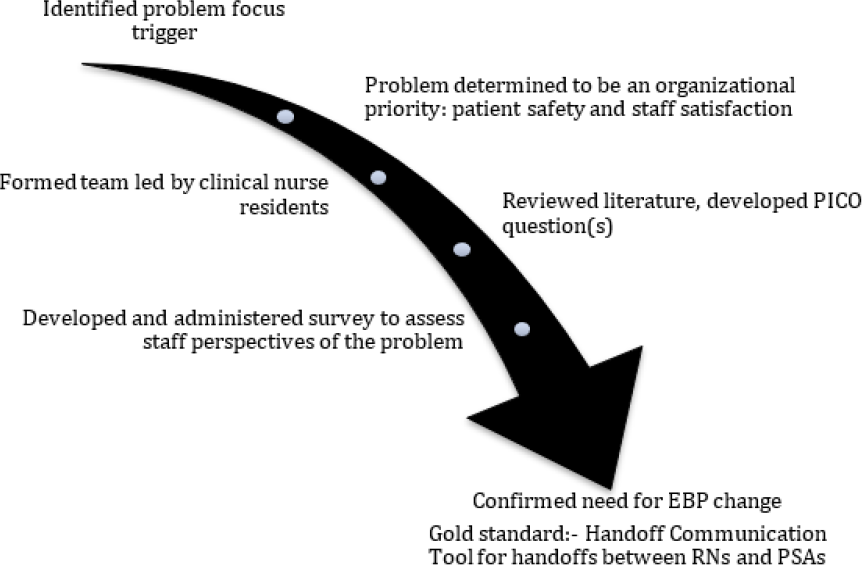
Progression of EBP Project
The PICO question asked, “If inconsistency in communication between PSAs and nurses causes safety concerns related to patient care, how does the implementation of a standard handoff impact staff satisfaction?” In retrospect, this could have been two questions, one focusing on the patient and one on staff engagement:
Question 1: Does inconsistency in communication between PSAs and nurses impact patient safety?
Question 2: Does the implementation of a standard handoff tool impact staff satisfaction?
Nursing Staff Survey
To explore the communication problems, a written qualitative survey (see Figure 2) was created and administered to the nursing staff on the pediatric unit, chosen because they were often utilized as sitters. All staff members including RNs, LPNs, and CNAs were made aware of the survey via email, and the survey was made available at the nurse's station for one month; participants returned the anonymously completed surveys to the mailbox of the designated nurse resident. Eight of the ten staff members employed on this unit completed surveys, for a completion rate of 80%.
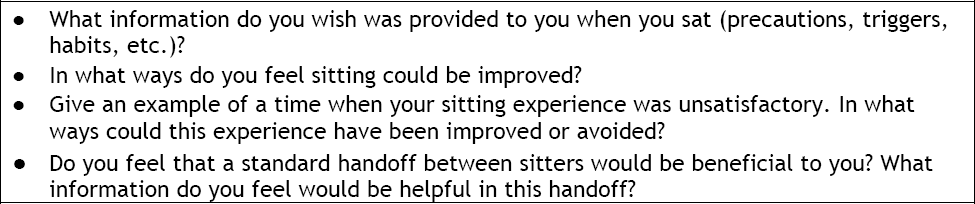
Nursing Staff Survey Questions
Survey results are summarized in Figure 3.
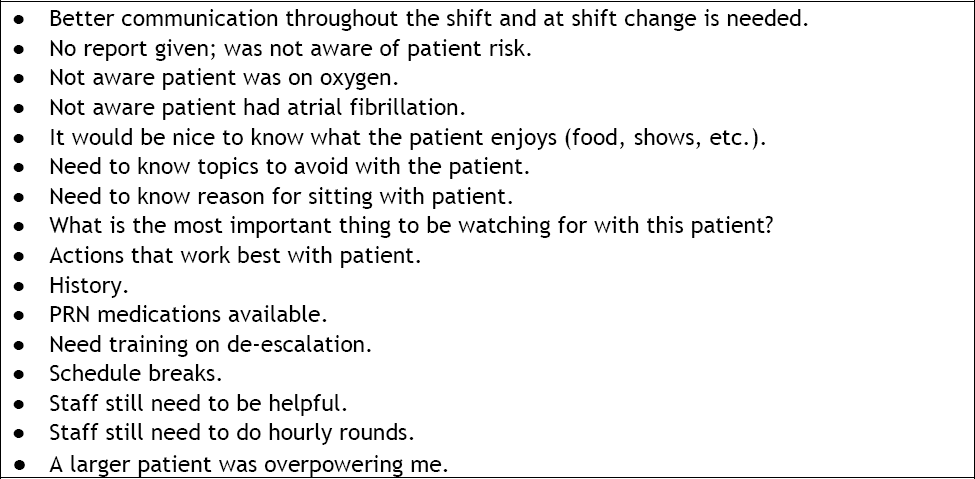
Summary of Feedback from Survey Questions
The survey results provided information related to personal experiences in the role of sitting, current problems with communication, and suggestions for ways to improve communication. This information supported suspected concerns that effective communication was not consistently taking place. Graham et al. (2020) reported similar findings in a survey taken by 139 sitters; only 27% of the sitters reported receiving a handoff from an RN (Graham et al. 2020).
Handoff Tool
The Agency for Healthcare Research and Quality's Team Strategies to Enhance Performance and Patient Safety (TeamSTEPPS) curriculum defines handoff as “the transfer of information [that] … includes the opportunity to ask questions, clarify, and confirm” (Pocket Guide, 2020, p.12). The nurse residents determined that the best way to conduct this transfer of information was to use the Situation/Background/Assessment/Recommendation (SBAR) format. Table 1 provides descriptors of each word in the SBAR mnemonic.
: SBAR Descriptors
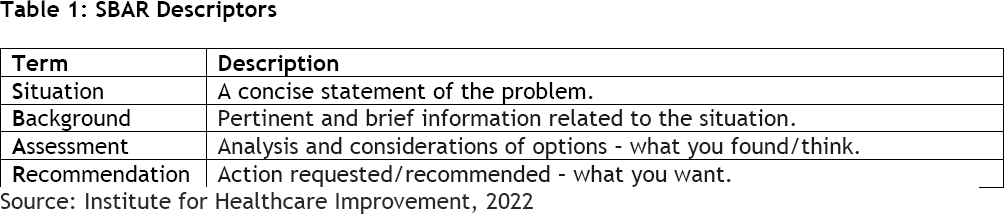
Source: Institute for Healthcare Improvement, 2022
In this transfer of information, the nurse residents felt that information should come from both the patient's off-going nurse and PSA to the oncoming PSA. To standardize this information, they created the Patient Safety Attendant Handoff Form (See Figure 4). To stay consistent with the SBAR format, the form was divided into 4 sections. Each category included subcategories to present information in an easy-to-view format for both those giving and those receiving handoff information.
Of greatest importance in the Recommendations category of the handoff form were the “trigger” and “de-escalation” sections alerting the PSA about behaviors to watch for and interventions to maintain safety.
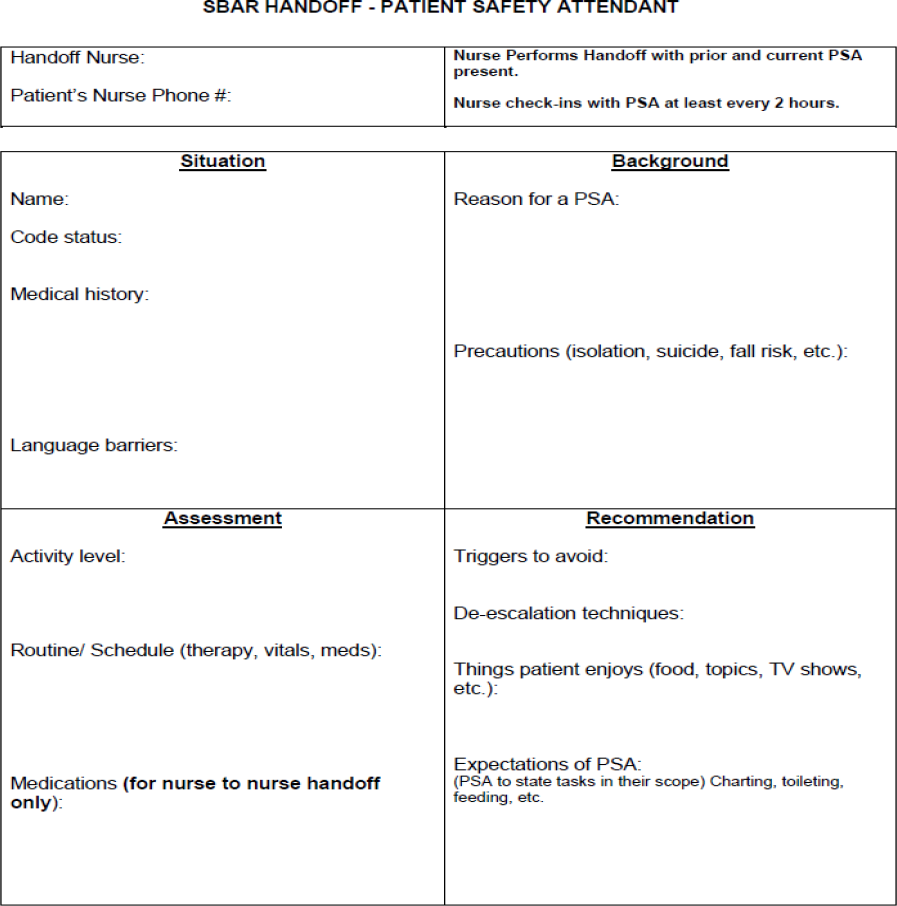
Patient Safety Attendant Handoff Form
Implementation of Patient Safety Attendant Handoff Form
To implement the handoff form, the creators spoke with representatives of the hospital's Forms Committee and incorporated their input into an updated form. The Forms Committee then entered the tool into the hospital's intranet page, so that it could be printed.
A summary of data from 100 completed handoff forms shows more than 80 communication variables, which demonstrates how complex the patient story can be for someone requiring constant observation.
Once the form was published on the intranet page, the creators submitted information about it to the hospital newsletter, which was emailed out to staff to inform them about updates and changes within the organization. The creators then presented the form and the structural model of summarized data (see Figure 5) to the Nursing Practice Standards and Performance Improvement Council to receive feedback on the use of the form within the organization.
Results
The intended outcome of implementing the handoff form was to improve safety, communication, and staff satisfaction. To assess the impact of the form on these outcomes at six months post-implementation, the nurse residents conducted three follow-up activities:
Reviewed 100 completed handoff forms and summarized the data.
Provided post-implementation surveys to PSAs along with the handoff form, to complete during their assignment.
Discussed findings with members of the Nursing Practice Standards and Performance Improvement Council to obtain feedback.
Handoff Form Review and Synthesis
Figures 5 and 6 represent the story summarized from 100 handoff forms using the first four steps of Nelson et al.'s (2021) methodology for health-care analytics. These steps are:
Step 1: Identify the variable of interest (the outcome variable).
Step 2: Identify the predictor variables (variables that impact the variable of interest).
Step 3: Organize the predictor variables by similarity in a structural model.
Step 4: Rank variables based on how directly they appear to relate to the variable of interest (the outcome variable). (Nelson et al., 2021)
In the middle of both Figure 5 and Figure 6 is the variable of interest: Communication between the RN and the PSA. According to Nelson et al. (2021), Figure 5 is considered a Structural Model of RN-PSA communication, with the outer circles representing those variables that drive the need for good communication between the RN and the PSA and that can impact patient safety. In this model there are more than 80 communication variables, which demonstrates how complex the patient story can be for someone requiring constant observation.
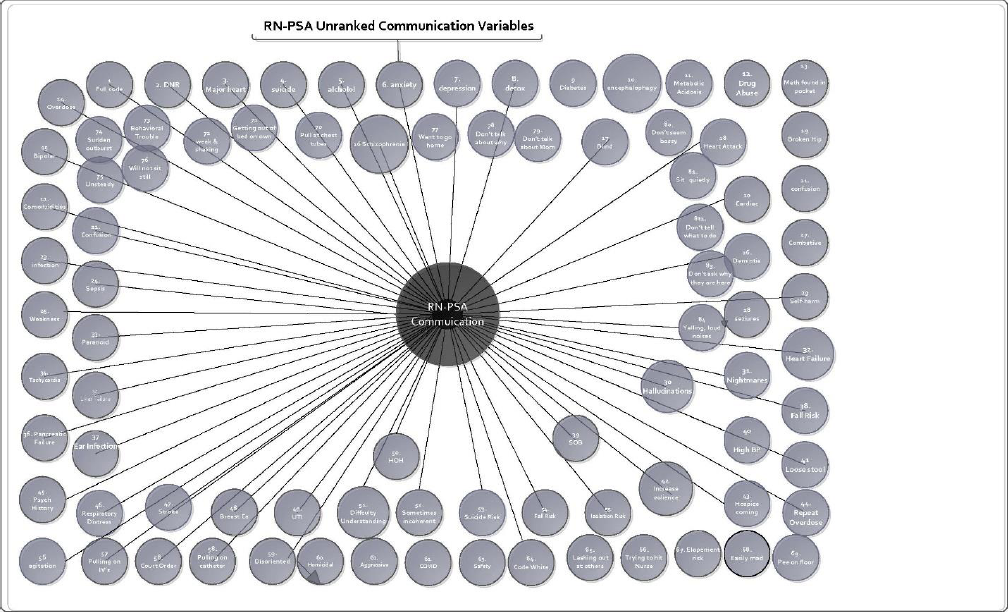
Structural Model: RN-PSA Unranked Communication Variables
Figure 6 advances the structural model of summarized data, organizing the data by SBAR categories and ranking the variables by their importance based on the number of times the information appeared on a handoff form (steps 3 and 4 of Nelson et al.'s methodology). The larger the circles, the more often the variables were reported about a patient requiring a PSA. The Situation category on the handoff form includes Medical History; the top three reasons for requiring a PSA are all mental/neurological health issues: chemical dependency, dementia, and depression. The only medical diagnosis in the top five reasons is cardiac issues. As a result, the reasons for needing a PSA listed in the Background section are predominately in two categories: behavioral or mental health. Of greatest importance in the Recommendations category of the form were the “trigger” and “de-escalation” sections alerting the PSA about behaviors to watch for and interventions to maintain safety.
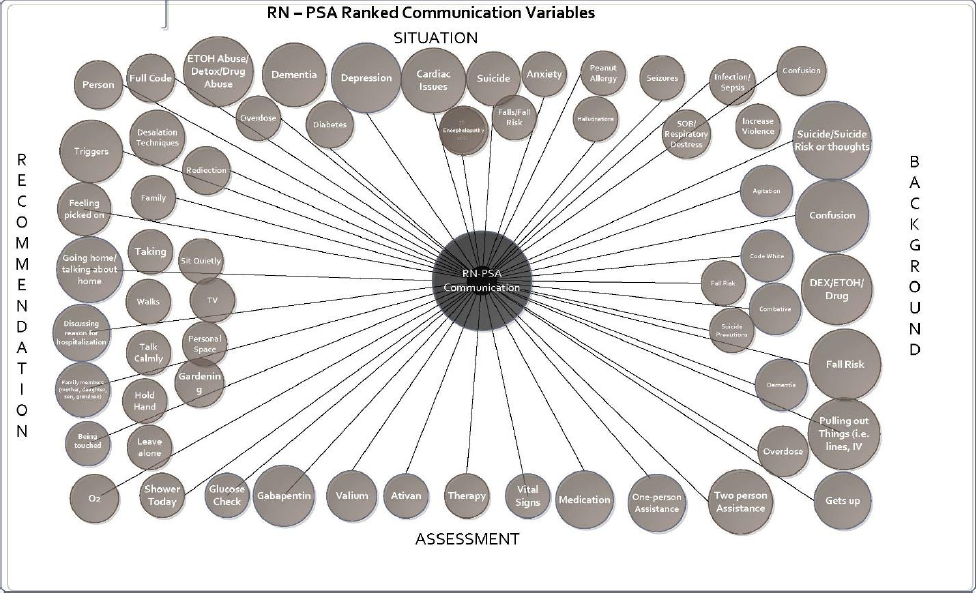
Structural Model: RN-PSA Ranked Communication Variables
Post-Implementation Survey Results
A 5-question survey administered 6 months post-implementation by the PSAs ‘manager was completed by 8 of the 12 PSAs included in the study.
Question 1: Was a handoff completed? If not, why?
All 8 PSAs answered “yes.”
Question 2: Did you feel you had adequate information for a safe and successful shift?
Seven PSAs answered “yes.” One PSA stated, “Not all the time. Sometimes you're not given much information, or you're given wrong info. Sometimes you have to rely on the white board, which can be old info or wrong.”
Question 3: Were check-ins with RNs completed (to give breaks, check on the patient, etc.)? how often?
Answers varied from 1 hour into the shift to every 3 hours. Three PSAs stated that consistency of check-ins varied by unit. One respondent stated they were on a unit “notorious” for not checking in, while others stated they were in another location known for consistent check-ins. One stated that check-ins varied from nurse to nurse rather than unit to unit.
Question 4: Do you feel this handoff form has improved your experiences sitting? Give examples of positive impacts it has had if any apply.
Six PSAs stated “yes.” One stated, “I feel a lot more comfortable going into nights not sitting blind. I document everything.” Answers to this question revealed that instead of only nurse-to-PSA handoffs, sometimes the handoff form was being used for PSA-to-PSA handoffs. Several PSAs stated that they preferred receiving handoffs from other PSAs rather than from nurses. “PSAs always do a great job [with handoffs]! It's when it's someone other than a PSA that they don't tell you what is going on with the patient.”
Question 5: Suggestions for improving the handoff form.
Three PSAs responded “none.” Two requested that handoffs be conducted from PSA to PSA rather than from nurse to PSA. Two responses were related to handoff format:
“I think that [the form] needs to have more room for the patient's behaviors/less about the medications because most times you don't know what medications they are getting if you're a PSA. I personally think it is more set up like how a nurse would be using it and not so much for a PSA.”
“Make two-sided so if [we] get moved to a new patient [we] have one to fill out.”
Discussion with Nursing Practice Standards and Performance Improvement Council The Nursing Practice Standards and Performance Improvement Council had several suggestions to improve the form:
Add a section for mental health.
Add a section for lines/tubes/drains.
Add reason for a PSA, such as diagnosis information and behavior descriptions.
Add a second page with suggestions for activities to keep the patient busy.
Make the form a rolling form rather than single use, so that each shift can add information from the previous shift.
The nurse residency program provided a pathway for new nurses to identify problems in the work setting and problem-solve their way through an issue to create a solution.
There was also conversation about the importance of the information on the form and how it could be shared with the interprofessional team, including whether these forms should be included in the patient's medical record. The information gathered on the forms can be beneficial to document what actions were taken by the PSA to maintain patient safety, but the PSAs can chart this information in the electronic medical record, using the handoff form only to organize their work.
After the meeting, all the information was summarized for any needed changes to the form, which will then be taken back to the Nursing Practice Standards and Performance Improvement Council for a final review.
Discussion
In the PSAs ‘post-implementation survey, multiple responses suggested that handoffs be conducted from PSA to PSA rather than from nurse to PSA, a new way for the form to be used. This could be tested with a “trial run” to gather information on how the form would be used differently. In support of this, another response stated that the form seemed to be designed for “how a nurse would be using it,” suggesting a restructure of the form to better fit the work of PSAs rather than the work of nurses. In the future, the form may be restructured to better fit the work of PSAs, and the handoff process may be broadened to include both the on-coming and the off-going PSAs but will still include the nurse.
Limitations
The sustainability of the Patient Safety Attendant Handoff Form is still unknown. This is a new process, of which some staff other than PSAs are still unaware. The initial survey used to gather staff feedback about the sitter communication issues may have been completed only by the most motivated staff (positive or negative) and therefore could have response bias. The same is true for the post-implementation surveys.
A challenge of implementing any new standard is creating awareness of the practice change and enforcing the change itself. The sole creators of this form were nurses; a more collaborative approach with PSAs when designing the form may have been beneficial. The Patient Safety Attendant Handoff Form was created at the same time as the PSA position was being developed; it may have been more useful to collect pre-implementation data from the newly hired PSA staff rather than from the pediatric nursing staff, but the PSA role at the start of the project was not yet established.
To ensure the success of a process change, colleague input is critical, as these are the individuals who will be incorporating the change into their practice.
Conclusion
Lessons Learned
The nurse residency program provided a pathway for new nurses to identify problems in the work setting and problem solve their way through an issue to create a solution. Now that the foundation of a quality improvement project has been established, it has shown the nurse residents how to create a solution for a workplace problem, including the order of steps required. Any facility can create and utilize a handoff form with simple background knowledge of what in formation is necessary to improve communication among colleagues. Colleague input is vital in creating a successful process change.
Communication is one of the most important aspects of health care to ensure a safe and successful environment for patients and staff. Through the literature search, pre-and post-implementation surveys, and colleague meetings, the importance of communication as a method to improve safety was repeatedly discussed, reiterating the importance of this process change as a way to raise communication standards in direct patient care.
Implications for Practice
The implementation of a Patient Safety Attendant Handoff Form or a similar form may be useful in improving communication in other facilities. To ensure the success of a process change, colleague input is critical, as these are the individuals who will be incorporating the change into their practice. The success of the handoff form lies in the hands of those who use it; it must be used consistently by staff, which is why those directly involved should take an active part in creating and implementing the new process.
Analysis of the content recorded on the handoff forms led to the development of structural models that can be used to build predictive models to direct resources and identify areas of high risk. Adding information obtained from the handoff form to the medical record could also improve the sharing of important information with other members of the interprofessional team. Nurse residency programs are becoming more than just a tool to bridge the transition of new nurses into practice; this program is also valuable in developing quality improvement efforts to improve patient safety and staff satisfaction.
Cite this article
Hawley, P., Holst, R., Bredlow, J., & Nichols, T. (2023). Development of a communication tool for handoffs involving patients cared for by sitters: An evidence-based practice project. Creative Nursing 29(1), Article 9.
Footnotes
Paige Hawley, BSN, RN, (she/her) is a nursing graduate of Allen College, after receiving a bachelor's degree in Sociology from Central College. She is currently an RN at MercyOne North Iowa Medical Center, with professional experience in COVID-19 care, orthopedics, and ambulatory surgery. She aims to make a positive impact on her patients by providing holistic care, connecting on a personal level with each patient. She is passionate about quality improvement projects that benefit her patients and her colleagues.
Rachel Holst, RN, ADN, (she/her), is an ADN honors graduate from Marshalltown Community College, and aims to obtain a bachelor's degree in nursing. She is pursuing her dream career as a pediatric RN at MercyOne North Iowa Medical Center, where she excelled in the nurse residency program. She is inspired to help others by improving patient and staff safety; she asks, “What could be done to create a better working environment?” in every situation.
Jennifer Bredlow, MSN, RN, (she/her), is Nurse Residency Program Coordinator at MercyOne North Iowa Medical Center, where she enjoys watching nurse residents become more confident and competent in their nursing skills throughout the program. Her goal is to help guide and strengthen new nurses ‘commitment to the organization and the nursing profession as a whole. She enjoys helping to solve problems and build relationships on a personal and professional level.
Tara Nichols, DNP, ARNP, CCNS, AGCNS, PMGT-BC, (she/her), is Director of the RN-BSN Program at Waldorf University in Forest City, Iowa, US, where she intends to inspire associate degree nurses to complete bachelor's degrees and to find their passion and a purpose-driven life in health care. Dr. Nichols is starting a private practice and consulting business, Matters of Comfort, in Mason City, Iowa. Her private practice focuses on the right combinations of pharmacologic and nonpharmacologic treatments, and her consulting focuses on mentoring and coaching nurses.