
Abstract
More and more people suffering from chronic pain (CP) utilize the emergency department (ED). However, their needs are not properly addressed. Stigmatization toward people with CP can partially explain this gap. Most studies in the ED have been focused on measuring nurses’ pain management knowledge in general, not negative attitudes toward CP. Hence, understanding of the determinants of the stigma related to CP is needed. The objectives of this study were to (a) describe the knowledge, beliefs, and attitudes of ED nurses toward people suffering from CP and (b) identify nurses’ characteristics associated with these perceptions. A cross-sectional web-based survey design was conducted using the KnowPain-12 questionnaire and the Chronic Pain Myth Scale. A total of 571 participants from 20 different states across the United States were recruited among whom 482 completed the entire survey. The sample included about one third of the ED nurses suffering from CP. Negative beliefs and attitudes toward people with CP were present in a considerable proportion of participants (up to 64%), even in nurses suffering from CP (up to 47.5%). Nevertheless, our results suggest that higher levels of education and suffering from CP were associated with better beliefs and attitudes toward people with CP. The ED presents an increased risk of stigmatization of people with CP as compared with the general population. Identifying determinants of the stigma associated with CP is crucial, as it will help tailoring awareness and educational campaigns. In addition, CP patients utilizing the ED often have complex needs which are difficult to address in this clinical environment. This situation can contribute to negative beliefs and attitudes. Given the scarcity of specialized care clinics for this population, health-care stakeholders should devise solutions to improve continuity of care in primary care settings and between the latter and ED.
Introduction
Chronic pain (CP) affects approximately 100 million American adults and has been identified as a public health priority (Briggs, 2012; Institute of Medicine of the National Academies-Committee on Advancing Pain Research, Care, and Education, 2011; National Center for Complementary and Integrative Health, 2017). People suffering from CP typically consult health-care providers in primary care settings and, given the lack of accessible pain clinics and specialized care facilities (Fashler et al., 2016; International Association for the Study of Pain, 2012), their inability to cope with pain sometimes brings them to visit emergency departments (ED; Gauntlett-Gilbert, Rodham, Jordan, & Brook, 2015; McLeod & Nelson, 2013; Poulin et al., 2016; Todd, Cowan, Kelly, & Homel, 2010). Unfortunately, CP is still underrecognized and undertreated in primary care settings (Choiniere et al., 2010; Glowacki, 2015; Kingma & Rosmalen, 2012; Kress et al., 2015; Lalonde et al., 2015; MacDonald, Flegel, Hebert, & Stanbrook, 2011; Sarzi-Puttini et al., 2012; Sessle, 2012; Zuccaro et al., 2012). Moreover, it has been established that the needs of people suffering from CP are not properly addressed in the ED (Jambunathan, Chappy, Siebers, & Deda, 2016; McLeod & Nelson, 2013; Poulin et al., 2016; Wilson et al., 2014).
Lack of knowledge and stigmatization toward people with CP can partially explain this gap (Cohen, Quintner, Buchanan, Nielsen, & Guy, 2011; Newton, Southall, Raphael, Ashford, & LeMarchand, 2013). In the ED, patients often feel invalidated (Jambunathan et al., 2016; Poulin et al., 2016; Smith et al., 2015). Several studies have underlined this barrier to treatment, particularly in relation to physicians’ reluctance to prescribe opioids (Baehren et al., 2010; Bounes, Jouanjus, Roussin, & Lapeyre-Mestre, 2014; Chen, Tsoy, Upadhye, & Chan, 2018; Ernst, Mills, Berner, House, & Herndon, 2015; Gueant et al., 2011; Matthias & Bair, 2010; Motov & Khan, 2009). Patients suffering from CP repetitively seeking help in the ED often get labeled as frequent flyers or drug-seeking by physicians (Chen et al., 2018; Geiderman, 2003; Jambunathan et al., 2016; Poulin et al., 2016; Wilsey, Fishman, Crandall, Casamalhuapa, & Bertakis, 2008; Wilsey, Fishman, Ogden, Tsodikov, & Bertakis, 2008). Regarding ED nurses, one study with a small sample (n = 44) highlighted a few negative beliefs and attitudes related to symptom magnification, prescription counterfeit, and addiction (Wilsey, Fishman, Ogden, et al., 2008). In addition, a few studies looked at the discrepancies between nurses’ pain assessment and patients’ report of pain (Pierik, IJzerman, Gaakeer, Vollenbroek-Hutten, & Doggen, 2017; Vuille, Foerster, Foucault, & Hugli, 2018). Patients at risk for being underassessed by ED nurses included people already taking analgesics, being anxious, and presenting a lower urgency level (Pierik et al., 2017). However, most studies in the ED have been focused on measuring nurses’ pain management knowledge in general (Chen et al., 2018; Moceri & Drevdahl, 2014; Pretorius, Searle, & Marshall, 2015; Ucuzal & Dogan, 2015) not misconceptions and attitudes toward people with CP.
Nurses are in a first-line position where they have to advise and support patients suffering from CP. The study of negative attitudes toward people with CP is thus most useful. Hence, understanding of the determinants of these negative beliefs and attitudes is needed (De Ruddere & Craig, 2016), and it will allow nurses to advocate for patients with CP visiting the ED (Jambunathan et al., 2016; Wilson et al., 2014). This preliminary step is necessary for ensuring that the content of awareness campaigns and educational programs aimed toward improving the care of CP patients in the ED are appropriate. Therefore, the objectives of this study were to (a) describe the knowledge, beliefs, and attitudes of ED nurses toward people suffering from CP and (b) identify nurses’ characteristics associated with these perceptions.
Methods
Design
A cross-sectional web-based survey design was conducted. First, after obtaining ethical approval, the web-based questionnaire was pilot tested in a convenience sample of 30 graduate nursing students. The pilot study was advertised through the Florida State University College of Nursing’s website and through the graduate nursing students’ mailing list, where a link to an online survey (Qualtrics®) was posted. The instructions included to complete the questionnaire and to annotate any suggestions regarding the clarity. Each of the items was accompanied by a check box (clear vs. needs improvement) and a text box where they could include comments. No further modifications were necessary as only two participants made some minor comments. More details regarding this first phase are provided in a previous article reporting the validation study of the instrument (Martorella, Lacasse, Kostic, & Schluck, 2019).
Second, the recruitment process included a link to the survey advertised on the Emergency Nurses Association’s website and on the social media page of the different Emergency Nurses Association’s state chapters. A participant information clip of 35 seconds was posted that featured a nurse explaining the focus of the study and eligibility criteria. By clicking on the link, potential participants were taken to the introduction page where information about the study was provided to ensure informed consent. Before beginning the questionnaire, they were informed that by taking the survey they were agreeing to participate and giving their consent for the use of their responses.
Sample and Data Collection
A voluntary, convenience sample was used. Inclusion criteria included nurses who have worked in an ED for at least six months, who could read English, and had access to the Internet and the ability to fill out an electronic-based survey. Data were collected using a Qualtrics® electronic survey which allowed the direct transfer of data into an SPSS database. The survey was approximately 20 minutes in length to complete and was available from October 1, 2017 to November 1, 2017. Upon completion of the survey, participants were provided with the option to enter a drawing for one of the four US$25 Visa gift cards by providing an e-mail address. Responses were limited to one IP address to prevent duplicates.
Study Variables and Instruments
Sociodemographic questionnaire
The following sociodemographic characteristics were collected at the beginning of the survey: age, sex, ethnicity, highest degree, clinical role, current setting of practice, years of experience, and suffering from CP for more than three months (yes/no).
Pain management knowledge
The KnowPain-12 questionnaire was used (Gordon et al., 2014). The questionnaire included 12 items and was developed to provide a brief measure of chronic noncancer pain management knowledge in health-care providers. Six topics were addressed: (a) initial pain assessment, (b) definition of treatment goals and expectations, (c) development of a treatment plan, (d) implementation of a treatment plan, (e) reassessment and management of longitudinal care, and (f) management of environment issues. Items were scored on a 6-point Likert-type scale ranging from 0 (strongly disagree) to 5 (strongly agree). Negatively formulated items (1, 5, 10, and 11) needed to be reversed so a higher score reflected better knowledge. A total score was calculated (possible range: 0–60). Internal consistency (α = .67) and construct validity analyses supported the use of the scale for measuring health providers pain management knowledge (Gordon et al., 2014).
Knowledge, beliefs, and attitudes toward people suffering from CP
The Chronic Pain Myth Scale (CPMS) was used (Lacasse, Connelly, & Choiniere, 2016), more specifically the first subscale (Items 1–9). This subscale measured knowledge, beliefs, and attitudes toward people suffering from CP, as opposed to knowledge, beliefs, and attitudes toward the treatment and the impact of CP. Items were scored on a 5-point Likert-type scale ranging from 1 (completely disagree) to 5 (completely agree). Negatively formulated items (2, 3, 4, 5, 7, 8, and 9) needed to be reversed so a higher score reflected better knowledge, attitudes, and beliefs. A total score was calculated for the entire subscale (possible score: 9–45). Among French-speaking individuals from the general population, internal consistency of the CPMS’s first subscale was achieved (α = .82), in addition to its construct validity (Lacasse et al., 2016). In the validation study of the English version of the questionnaire (Martorella et al., 2019), the first subscale of the CPMS demonstrated good internal consistency (α = .86). The structural validity was reproduced, and evidence was provided regarding its construct validity in the translated version as well.
Data Analysis
Participant sociodemographic characteristics were summarized using frequencies and proportions. Scores on the KnowPain-12 scale and knowledge, beliefs, and attitudes toward people who suffer from CP (CPMS Subscale 1) were summarized using means and standard deviations (SD). In addition, sociodemographic characteristics; scores on the KnowPain-12; and knowledge, beliefs, and attitudes toward people who suffer from CP were stratified by whether or not the participant reported suffering from CP, which was found to be a determinant in previous studies (Lacasse, Choiniere, & Connelly, 2017). Finally, a multiple linear regression model was built to determine which sociodemographic characteristics had significant relationships with knowledge, beliefs, and attitudes toward people with CP (the CPMS first subscale score being used as the dependent variable). All independent variables were treated simultaneously in the model. All analyses were performed using IBM SPSS Statistics version 25 (IBM Corp., Armonk, NY).
Results
Participants’ Characteristics
Participants’ Demographics by Chronic Pain Status.

Note. AA/AS = Associate of Arts/Associate of Science; BSN = Bachelor in Science of Nursing; RN = Registered Nurse; CNS/ARNP = Clinical Nurse Specialist/Advanced Registered Nurse Practitioner.
Percentages are row percentages. For example, 44.2% of males suffer from chronic pain.
There were 15 cases who provided no information beyond the first question. These were deleted and assumed to be missing completely at random. In addition, there were 58 cases who provided sociodemographic information solely. Sociodemographic characteristics of these participants were compared with those who answered the entire survey. There were no differences among demographics and the 10.3% of cases which were missing are assumed to be missing completely at random. There was one case who provided no sociodemographic information but answered the rest of the survey. Finally, there were three cases who answered all questions except the question about ethnicity. As the proportion of cases which we are assuming may be missing systematically is quite small (<1%), these cases were also deleted. The resulting data set has 481 responses.
χ2 test p values.
Pain Management Knowledge
Main Knowledge Gaps as Measured by the KnowPain-12.
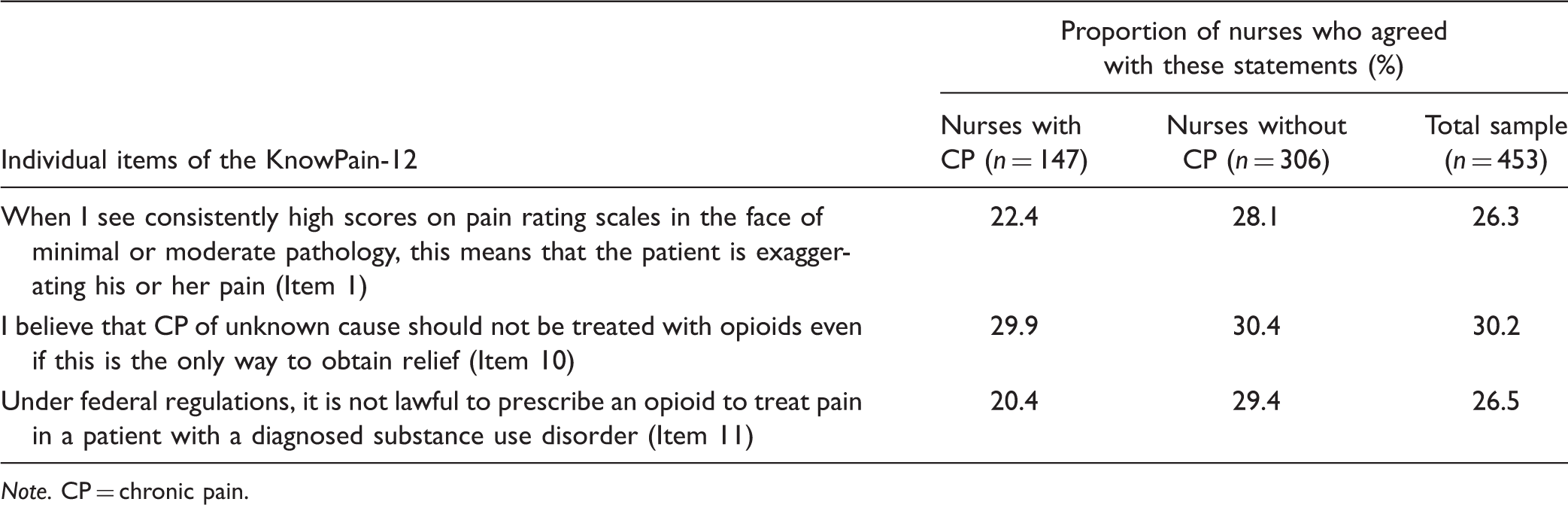
Note. CP = chronic pain.
Knowledge, Beliefs and Attitudes Toward People Suffering From CP
Beliefs and Attitudes Toward People Suffering From CP Reported by Participants (n = 481).

Note. CP = chronic pain.
Predictors of Knowledge, Beliefs, and Attitudes Toward People Suffering From CP
Multiple Regression of Knowledge, Beliefs, and Attitudes Toward People Suffering From CP on Demographics—Parameter Estimates.

Note. Bold values represent predictors with p values < .05. AA/AS = Associate of Arts/Associate of Science; BSN = Bachelor in Science of Nursing; RN = Registered Nurse; CNS/ARNP = Clinical Nurse Specialist/Advanced Registered Nurse Practitioner; ED = emergency department; CP = chronic pain; SE = standard error.
Discussion
To our knowledge, this is the first study describing the main negative beliefs and attitudes toward people suffering from CP in ED nurses and determining individual factors associated with these beliefs. Negative beliefs and attitudes toward people with CP were present in a substantial proportion of participants. It was also found that higher levels of education (graduate degree) and suffering from CP were associated with better beliefs and attitudes toward people with CP.
It is important to note that pain management knowledge, as measured by the KnowPain-12 (Gordon et al., 2014), was quite low (mean total score of 36.6 of a possible score of 60) as compared with a previous study with various health-care providers including registered nurses and advanced registered nurse practitioners (Gordon et al., 2014). The sample included about one third of the nurses suffering from CP. However, no significant difference in terms of pain management knowledge was observed between nurses suffering or not from CP. In agreement with the previous research, knowledge gaps were related to opioid administration and pain assessment (Moceri & Drevdahl, 2014; Pretorius et al., 2015; Ucuzal & Dogan, 2015).
Negative beliefs were mostly illustrated by the fact that 64.4% agreed that CP patients become dependent on their medications, 29.5% agreed that CP patients often tend to exaggerate the severity of their condition, and 24.7% agreed that CP patients complain about their pain but continue their activities, so their pain should not be that bad. These corroborated studies conducted with physicians (Bounes et al., 2014; Chen et al., 2018; Ernst et al., 2015; Gueant et al., 2011) and patients in the ED (Jambunathan et al., 2016; Poulin et al., 2016) underlining the stigmatization of CP patients in this clinical setting. It is noteworthy that the main themes (addiction and symptom magnification) were the same as the ones identified a decade ago (Wilsey, Fishman, Ogden, et al., 2008), which suggests a lack of improvement in this matter. Many nurses reported that people suffering from CP become dependent on their medications like drug addicts (Item 8). This finding could be expected considering the increasing negative attention given to opioids that is clearly conducive to the stigmatization of people with CP (Brooks, Unruh, & Lynch, 2015; Goodyear, Haass-Koffler, & Chavanne, 2018; Lynch, 2016). Nonetheless, this result is concerning and even more so as a previous study had identified this belief in 23% of a sample from the general population (n = 1,958), including health-care providers in which this belief was present for 16% (Lacasse et al., 2017). Moreover, surprisingly, 47.5 % of nurses suffering from CP agreed with this statement as well, whereas a previous study identified this belief in 14% of CP sufferers (Lacasse et al., 2017). The two other most common misconceptions were related to symptom magnification by CP patients (Items 9 and 7) and were present in a quarter to a third of participants. Again, although the proportion was slightly lower, nurses suffering from CP also had these beliefs. In the study by Lacasse et al. (2017), solely 7.9% of participants from the whole sample had this belief (Item 7) and it was a similar proportion for health-care providers and people suffering from CP. These results, when compared with those from the general population, suggest that the ED presents an increased risk of stigmatization for people with CP.
Regarding predictors of negative beliefs and attitudes toward people with CP, the level of education was not previously found to be a predictor in the general population (Lacasse et al., 2017). Similarly, a previous study with ED nurses’ (n = 91) did not show a relationship between education level and knowledge and attitudes about pain (Moceri & Drevdahl, 2014). Furthermore, a study found that physicians reading various sources of information such as scientific journals were more likely to apply pain management practice guidelines (Duenas et al., 2018). Our findings, in light of the work of Duenas et al. (2018), suggest that nurses with a graduate degree may be more likely to be involved in evidence-based practice, namely, searching literature and updating their knowledge and practice, which could contribute to a better attitude toward people with CP. Regarding the characteristic of suffering from CP, similarly to our results and expectedly, it has been identified as a predictor of better attitudes in the general population (Lacasse et al., 2017). However, nurses suffering from CP still showed important levels of negative beliefs and attitudes as reflected by some specific items of the CPMS. Interestingly, it was previously found that physicians who experience or have experienced CP are less likely to apply pain management practice guidelines (Duenas et al., 2018). It was also observed in the general population that people with CP had more negative beliefs toward its treatment than others (Lacasse et al., 2016). These results could be explained by the fact that people experiencing CP are often reluctant toward the effectiveness of treatment and are highly dissatisfied with the care they receive (Chen et al., 2018; Duenas et al., 2018; Jambunathan et al., 2016; Poulin et al., 2016).
It is nothing new to state that continuing education efforts must be made to improve pain relief and the Institute of Medicine’s blueprint helped spread the word (Institute of Medicine of the National Academies-Committee on Advancing Pain Research, Care, and Education, 2011). However, it seems logical that besides improving and updating knowledge regarding CP mechanisms, assessment and management, efforts should be made toward modulating beliefs and attitudes regarding people with CP as well. Indeed, limited knowledge along with negative attitudes toward CP were found to inhibit the implementation of pain management guidelines (Duenas et al., 2018). Identifying determinants of the stigma associated with CP is crucial, as it will help tailoring awareness campaign and educational programs (De Ruddere & Craig, 2016). In addition, although health-care providers suffering from CP have better attitudes toward patients with CP, it does not necessarily translate into better pain management practice (Duenas et al., 2018). Further studies should be conducted to address the specific needs of this subgroup. Finally, CP management in the context of the ED is particularly challenging. CP patients utilizing the ED often have complex needs which are difficult to address in this clinical environment (Jambunathan et al., 2016; Poulin et al., 2016). This situation can be frustrating for clinicians and could result in creating or increasing negative beliefs and attitudes. For instance, the lack of longitudinal care in the ED is one of the factors contributing to care provider dissatisfaction related to CP management (Chen et al., 2018). Given the scarcity of specialized care clinics for this population, health-care stakeholders should devise solutions to improve continuity of care in primary care settings and between the latter and ED.
Strengths and Limitations
Strengths of this study included the minimization of a possible confounding bias for the identification of predictors by utilizing a multiple regression model. A potential type II error was also minimized through a large sample size (Austin & Steyerberg, 2015). Although it was not possible to calculate a response rate, which kept us from evaluating the risk of a nonresponse bias, participants came from 20 different states across the United States and had sociodemographic profiles similar to the U.S. national statistics which contributed to the external validity of our results (Bureau of Labor Statistics, 2003). As it is the case for many surveys, a possible bias was social desirability (Grimm, 2010). However, given the considerable proportion of some negative beliefs and attitudes that was recorded, there is a reason to think that participants were transparent when completing the survey. In addition, participants in the sample were self-selected which could have led to bias in the results. Of note, one third of the participants suffered from CP which could mean that they had a particular interest in responding to the survey. Yet, descriptive statistics were stratified according to the CP status of participants and all characteristics were included in the multiple regression model to address this limit (Lacasse et al., 2017). Finally, the survey did not test the impact of continuing education training regarding pain management on knowledge and attitudes scores. Nonetheless, pain management knowledge was measured.
Conclusion
To our knowledge, this study is the first to describe beliefs and attitudes toward people with CP in ED nurses and to identify potential predictors of these perceptions. The results show a high proportion of misconceptions toward people suffering from CP. Hence, ED nurses with higher level of education and suffering from CP seem to be more likely to show positive beliefs and attitudes toward people with CP. Tailoring educational efforts according to these characteristics holds promise for better care of people with CP. However, the acute clinical environment of the ED presents a challenge to address the needs of CP patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Martorella received funding from the Florida State University’s College of Nursing. This work was supported by Florida State University.