
Abstract
Background
Pan-scan, which comprises computed-tomography (CT) scans of the head, cervical spine, chest, abdomen and pelvis, allows for the rapid evaluation of life-threatening injuries. We aimed to describe the utilisation of pan-scan in trauma patients in the Emergency Department (ED) of a level 2 trauma centre for detection of clinically significant injuries and their subsequent management.
Methods
This was a retrospective study involving trauma patients attended to by the hospital trauma team at the ED from 18 August 2018 to 31 December 2022. Information on demographics, mechanism of injury, injuries sustained, injury severity score (ISS), pan-scan findings, clinical management and outcome were collected and analysed.
Results
Among 496 patients, pan-scan was performed in 129 of them (26.0%). Eighty (62.0%) patients had pan-scans that were positive with clinically relevant findings, the top three findings were rib fractures, intracranial hemorrhage and vertebral fractures. Eighteen (22.5%) patients with positive pan-scans underwent intervention, of which the most common was craniectomy/craniotomy and/or intracranial pressure monitor insertion in the operation theatre. Patients with pan-scan had a longer median length of stay at the ED [113 minutes (interquartile range (IQR) 75.5 to 156.5 minutes)] than those without [93 minutes (IQR 63 to 136 minutes)] but this was not statistically significant when corrected for ISS (p = .089). The mortality rate for patients with pan-scan performed was 5.4%.
Conclusion
The proportion of patients with pan-scan performed was low and most of the findings did not require intervention. Considering the purpose of pan-scan to the patient, clinician and trauma system, as well as adaptation of existing criteria for pan-scan are necessary to better identify patients who would benefit from it.
Introduction
Patients with traumatic presentations to the Emergency Department (ED) may have multiple injuries involving different parts of the body with varying severities. Prompt diagnosis and treatment of injuries can greatly improve the chances of survival and reduce patient morbidity. Pan-scan, which comprises computed-tomography (CT) scans of the head, cervical spine, chest, abdomen and pelvis, can allow for a rapid evaluation of injuries and their severities, thereby hastening the process of decision making on patient management. 1
However, pan-scan is not without its risks – there can be potential harm from ionising radiation and contrast-induced nephropathy. In addition, CT scan in the ED is a valuable resource and indiscriminate use can cause delays to the diagnosis and management of other patients in the ED, as well as increase healthcare costs to patients and the healthcare system. Furthermore, the mortality benefit of pan-scan has not been proven. 2 Therefore, pan-scan is not routinely performed for every trauma patient and a standard reference for when to perform pan-scan has yet to be established in existing literature.
Previous works on the utility of pan-scan were predominantly done in level 1 trauma centres.1–13 In this study, we aimed to describe the utilisation of pan-scan in trauma patients in our ED of a level 2 trauma centre for detection of clinically significant injuries and their subsequent management. The insight gleaned from this work can help to guide decisions on when pan-scan should be considered in this setting, thus improving the care of trauma patients while optimising the utilisation of healthcare resources.
Materials and methods
Study setting
This study was conducted in the general ED of a restructured tertiary hospital in Singapore. The annual census was about 122,000 with trauma patients accounting for approximately 15% of the total census. The hospital is a level 2 trauma centre and forms part of a regional trauma system consisting of two other level 1 trauma centres.
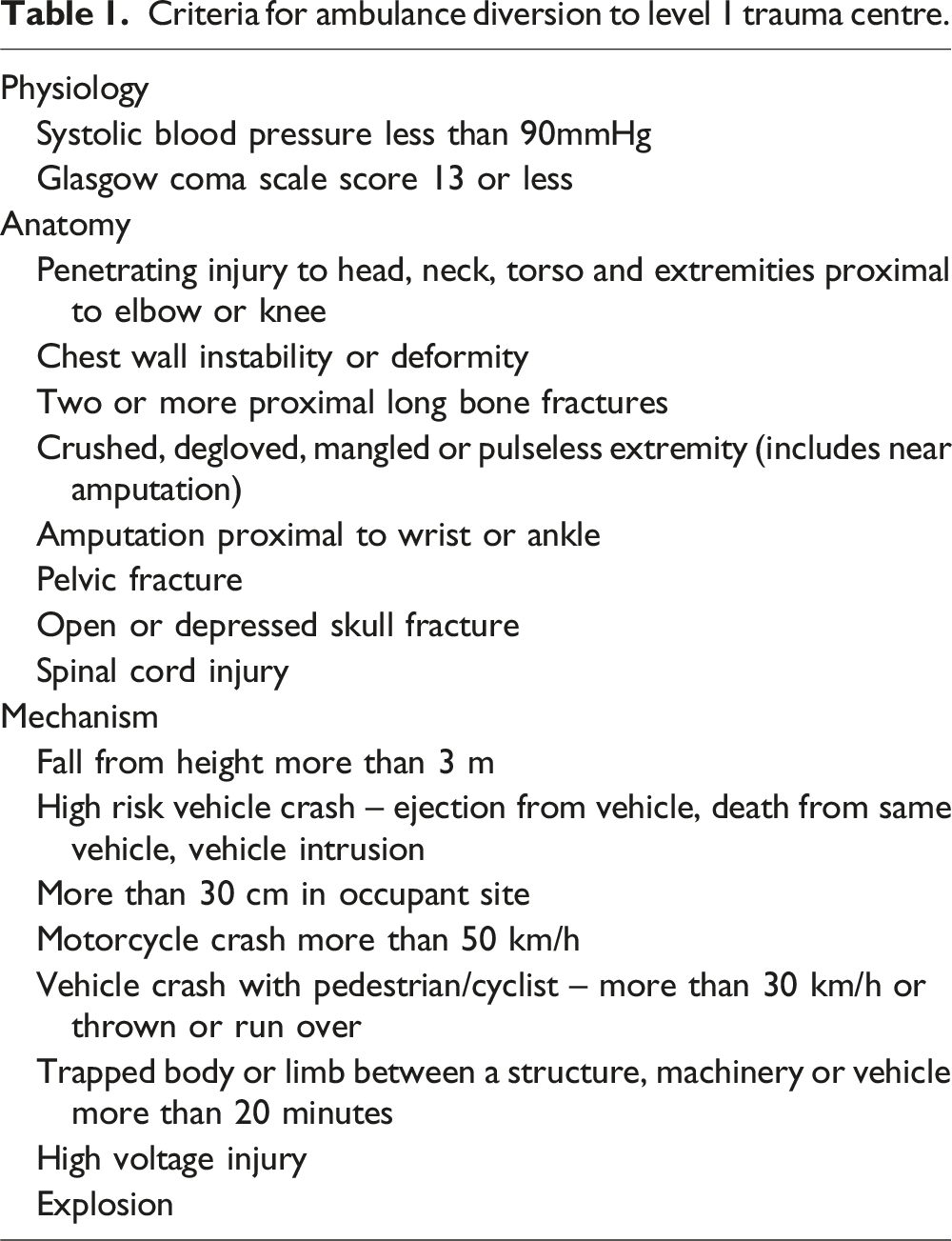
Criteria for ambulance diversion to level 1 trauma centre.
Criteria for activation of trauma team.

CT scan is performed using the Siemens Somatom Force (Siemens Healthcare, Germany) scanner and is available within the ED round the clock. The attending team will assess the patient and then decide if CT scan is needed or not – if needed, either pan-scan or selective scan of specific regions can be performed. A pan-scan will consist of plain CT scans of the brain and cervical spine, followed by CT scans (arterial and portovenous phases) of the thorax, abdomen and pelvis.
Patients may be transferred to one of the level 1 trauma centres in the regional trauma system if further trauma specific general surgery or intervention radiology expertise is deemed necessary after evaluation at the ED. Otherwise, patients may be admitted to the Extended Diagnostic and Treatment Unit within ED, or inpatient units under the relevant specialty for further assessment and management. The disposition decision could be made by the attending team based on findings on pan-scan or selective scan, in conjunction with clinical assessment.
Study design
This was a retrospective study involving trauma patients who presented to the ED from 18 August 2018 to 31 December 2022. Patients were included if they were attended to by the hospital trauma team at the ED. Information on demographics, mechanism of injury, injuries sustained, injury severity score (ISS), CT scan findings (if performed), clinical management and outcomes were collected in standardised forms and analysed. Patients were divided into two groups – pan-scan performed or pan-scan not performed in ED, with the latter consisting of patients with selective CT scan of specific regions or no CT performed.
Ethics
This study was approved by the Institutional Review Board of SingHealth, Singapore (CRIB Reference 2021/2417).
Statistical methods
Statistical analysis was performed using SPSS version 25 (SPSS, Chicago, IL). Continuous data were presented as median with interquartile range (IQR). Categorical data were presented as frequencies with percentages. Mann-Whitney U test was used to compare medians. Chi-square test was used to assess association between categorical variables. Statistical significance was taken as p-value less than 0.05.
Results
There were 77,132 trauma patients during the study period – 2100 (2.7%) were triaged as P1 (emergent), 30,823 (40.0%) were triaged as P2 (urgent) and 44,209 (57.3%) were triaged as P3 (ambulatory).
Patients attended to by hospital trauma team and pan-scan performed
Demographics and details of injuries.

a– One patient had missing information regarding the road traffic accident and two patients had missing information regarding the fall.
Positive pan-scan
Findings of positive pan-scan.
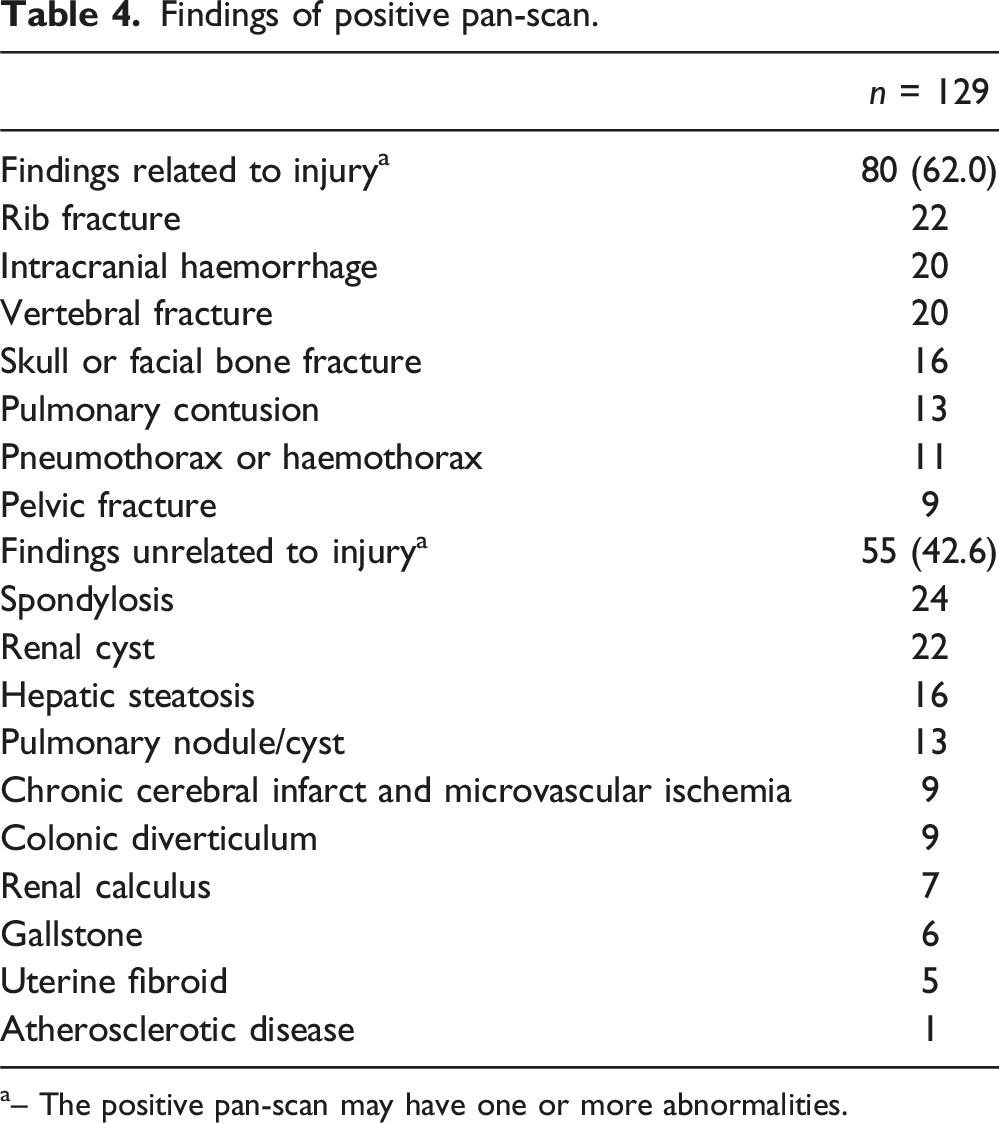
a– The positive pan-scan may have one or more abnormalities.
Clinical management of patients with positive pan-scan
Eighteen (22.5%) patients with positive pan-scans underwent intervention. Chest tube insertion or finger thoracostomy (n = 7) was the only intervention performed in ED. The other interventions were performed in the operation theatre with craniectomy/craniotomy and/or intracranial pressure monitor insertion being the most common (n = 6). The other interventions included laparotomy (n = 3), cervical decompression/laminectomy and fusion (n = 3), as well as cervical stabilisation of cervical spine fracture (n = 1).
The median length of stay at the ED for patients with pan-scan performed was 113 minutes (IQR 75.5 to 156.5 minutes), compared to 93 minutes for those without (IQR 63 to 136 minutes) (p = .006). After adjusting for ISS, the difference in median length of stay at the ED for patients with pan-scan and without pan-scan did not remain statistically significant (p = .089).
Disposition from ED and mortality.

a– Forty-nine patients who were dead on arrival at ED were excluded.
b– Three patients in the group of patients with pan-scan performed and 10 patients in the group of patients with no pan-scan performed were discharged against medical advice.
Discussion
Although pan-scan is readily available at the ED of a level 2 trauma centre, it was performed in about a quarter the patients who were attended to by the hospital trauma team – the majority of the patients receiving either selective CT scan of specific body regions or no CT scan. In these patients where a prompt diagnosis and timely management were important, pan-scan was positive in about three-fifths of them with findings related to the injury. However, among these only about a fifth required intervention and about two-fifths had incidental findings unrelated to the injury.
A systematic approach is necessary to identify injuries in the trauma patient. The attending team should consider all possible injuries given the mechanism, then take practical steps to identify them through clinical examination and use of adjuncts such as point-of-care ultrasound and x-ray. However, despite the best efforts, injuries can still be missed and therein lies the value of pan-scan to identify injuries. In our study, thoracic and head injuries were the most common on pan-scan. This finding was similar to a study conducted in an Iranian ED by Sabzghabaei et al. 3
However, rather than just focusing on detection of injuries, the value of pan-scan for the patient should be examined based on detection of findings which necessitate intervention. In our study, only about a fifth required intervention, and the rest of the findings did not require intervention either in the ED or operation theatre. Looking at the list of interventions performed, these findings could have been detected on x-ray and selective CT scans instead of a pan-scan. In the Iranian study mentioned previously, pan-scan led to a 16% increase in detection of thoracic injuries but similar detection of other injuries as compared to selective CT scan. 3 This increase in detection of thoracic injuries may have led to the attending team being compelled to take action such as chest tube insertion in ED which may not have been necessary if the patient was saturating well on room air and not showing any signs of respiratory compromise.
Other than whether the positive findings required intervention or not, the value of pan-scan for the patient could also be in terms of whether findings changed or expedited patient management. In a study by Hoffstetter et al, it showed that out of 109 patients with pan-scan performed, 15 obtained specialist review for a positive finding but only one patient had a change in treatment. 4 Furthermore, the patients in this study who underwent pan-scan did not receive intervention faster or get discharged earlier when compared to their counterparts who did not undergo pan-scan. However, in another study consisting of 1000 patients, Salim et al showed a higher proportion of patients who had a change in management at 19% and among these, eight patients proceeded directly to the operation theatre. 5 This wide variation in impact of pan-scan to change management could be attributable to the differing settings, populations, circumstances of injury, findings and clinical practices across the studies.1,4–6
Beyond the patient level, the value of pan-scan should also be examined at the level of the clinician based on detection of findings to guide decision making about need for monitoring or intervention, and the level of the trauma system to right-site the patient for care. This would be important as the clinicians need to know what injuries are present so decisions on management can be made. For the trauma system, it would determine if a hospital has the necessary expertise and support to manage the patient, or if the patient needs to be transferred to a level 1 trauma centre for definitive treatment. Compared to previous works on utility of pan-scan which were predominantly done in level 1 trauma centres, this work was done in a level 2 trauma centre where CT is available round the clock.1–13 In this setting, the decision for pan-scan versus selective CT should be made either for the purpose of detection of injury and need for intervention at a patient level, for aiding in decision making at a clinician level, or for right-siting of the patient at a trauma system level.
Unfortunately, pan-scan also can detect incidental findings unrelated to the injury. In this study, about two-fifths of patients with pan-scan performed had incidental findings. This was similar to several studies reporting the prevalence of incidental findings which ranged from 15 to 40%.7–9 Majority of these incident findings did not require intervention as the patient was asymptomatic and did not exhibit symptoms. Nonetheless, these incidental findings should be communicated to the patient and appropriate follow-up arranged. However, in this study, 42 out of 54 (77.8%) of the incidental findings were not mentioned in discharge summaries, and it was uncertain if these were acknowledged by the attending team, communicated to the patients or referred to relevant specialties for follow up.
In a meta-analysis of pan-scan in trauma patients by Jiang et al, they found that patients who had pan-scan had a shorter length of stay at the ED by about 28 minutes which could be attributable to quicker diagnosis of injuries by pan-scan. 14 However, our study found that the median length of stay at the ED was longer for patients with pan-scan performed by 20 minutes but this difference was not statistically significant after adjusting for ISS. This was not surprising as the higher proportion of patients with moderate to very severe injuries among the group with pan-scan performed required a longer time spent for clinical assessment and stabilisation before pan-scan, performing and reporting of pan-scan, as well as decision making about the findings instead of time taken for intervention since most of findings did not require intervention in our study. Pan-scan consists of a standardised protocol, thereby streamlining the scanning process and making it faster to perform the scan. However, time would still be needed to report the scan – the mean time for an initial interpretation of pan-scan by the radiologist could take 11 minutes and a preliminary report could take up to 32 minutes. 10 Once the findings were made known to the attending team, decisions on intervention and disposition had to be made. This may involve discussion with other healthcare professionals such as the trauma surgeon at the level 1 trauma centre for transfer, the anaesthetist in the operation theatre for emergency surgery, the intensivists in the Intensive Care Unit for admission, or relevant specialties such as neurosurgery for management of intracranial haemorrhage. Further studies would be useful to delineate the impact of processes, which are variable across EDs – such as assessing and stabilising patients, performing and reporting pan-scan, decision making and intervening on positive finding – on the length of stay at the ED.
The mortality rate for patients with pan-scan performed was about five times as high as that of those without pan-scan performed in this study. This finding would continue to complicate the debate on the mortality impact of pan-scan.2,11 For instance, a study originating from United Kingdom showed a higher mortality rate like our study, while a study originating from Thailand showed a lower mortality rate.1,12 Another study from Netherlands and Switzerland attempted to further shed light on this mortality impact by examining if pan-scan reduced mortality for patients compared to selective CT – however, pan-scan did not reduce mortality. 13
Despite the ongoing debate, the most often used criteria to determine need for pan-scan in trauma patients was a combination of high-risk mechanism of injury, compromised vital signs and clinical suspicion of severe injuries involving two or more body regions. 15 However, this systematic review of 30 eligible studies observed significant heterogeneity in defining high-risk mechanism of injury and cut-off values for compromised vital signs. When the criteria was applied to our study results, we found that among the 18 trauma patients with positive pan-scan requiring intervention, ten (55.6%) had high-risk mechanism of injury which included vehicle crash more than 50 km/h or fall from height more than two m; four (22.2%) had compromised vital signs on arrival to ED which included tachycardia and hypotension; and eight (44.4%) had clinical suspicion of severe injuries involving two or more regions. We further observed that ten (55.6%) patients had altered mental status or were intoxicated with a Glasgow Coma Scale score 13 or less. Therefore, there is no one-size-fits-all criteria as it would lack applicability to the different trauma settings and populations. Beyond the purpose of pan-scan to the patient, clinician and trauma system, there should be careful consideration of clinical context and local data in order to derive and validate the criteria to perform pan-scan in trauma patients.
Limitations
Firstly, this study was based on the experience of a single ED in Singapore which is a level 2 trauma centre. The recommendations based on our results must be considered in the context of our setting. Next, this was a retrospective study so there was missing information due to inability to standardise documentation. In addition, certain data relevant to this work such as the reason for performing or not performing pan-scan or selective CT of specific regions, whether the CT scan findings changed clinical management or affected length of stay at ED or during hospitalisation, as well as adverse outcomes from pan-scan were not available. Furthermore, we were unable to assess the impact of pan-scan on other aspects such as healthcare cost and impact of resource utilisation on other patients in ED.
Conclusion
The proportion of pan-scan performed at the level 2 trauma centre in our study was low. While most of the findings did not require intervention, results of the pan-scan could inform patients of their injuries and need for intervention, facilitate decision making by clinician on requirement for monitoring and right-siting the patient within the trauma system for further management. Further adaptation of criteria from existing evidence on when to perform pan-scan is necessary to better identify patients who would benefit from pan-scan at the ED, while balancing the potential for incidental findings and adverse events, as well as the increase in healthcare cost.
Footnotes
Acknowledgements
None
Author contributions
Yan Lin Shannen See – Data collection, statistical analysis, results interpretation, manuscript preparation. Chee Yun Eunice Chan – Results interpretation, manuscript review. Shiun-Hwa Chantal Lim- Manuscript review. Juinn Huar Kam – Results interpretation, manuscript review. Jen Heng Pek – Study design, statistical analysis, results interpretation, manuscript review. Hui En Hannah Ang – Results interpretation, manuscript review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The data of this study would not be available in accordance to approval by Institutional Review Board at SingHealth, Singapore.