
Abstract
The increasing complexities of health care coupled with the decreasing importance of ethical values held by college students, including nursing students, compel nurse educators to step up efforts to strengthen the moral courage values of their students. While the nursing curriculum is the ideal breeding ground for building moral courage values, few studies describe how these values were embedded in any nursing curriculum, much less an accelerated bachelor’s degree in nursing (ABSN) curriculum. This study outlines an ABSN curriculum with teaching-learning activities designed to build moral courage values in its classroom and clinical settings. Faculty perceptions of 29 ABSN students’ honesty, respectfulness, responsibility, fairness, and compassion were surveyed 4 weeks after beginning, and again at the end of the ABSN program. The ABSN exit questionnaire administered annually by the College Office of Institutional Research, assessed the effectiveness of the ABSN curriculum. Of the 20 learning outcomes on the questionnaire, five related to moral courage values. The 5-point response scale ranged from Not at All, to Somewhat, Moderately, Well, and Extremely Well. t-test calculations revealed significant growth for four of the five values surveyed. Honesty, responsibility, fairness, and compassion were each positively significant at the p < .05 level. For the 27 of the 29 ABSN students who responded to the exit questionnaire, the Well and Extremely Well responses ranged from respectfulness and responsibility at 73%, to compassion and honesty at 78%, and fairness at 82%. Teaching-learning activities to build moral courage values successfully promoted the nursing program objective that the student will demonstrate proficient clinical, technological, and ethical competence in the delivery and management of health care.
Keywords
Introduction
The increasing complexities of health care coupled with the decreasing importance of ethical values held by college students, including nursing students, compel nurse educators to step up efforts to strengthen the moral courage values of their students (Bickhoff, Sinclair, & Levett-Jones, 2017; Jimenez-Lopez, Roales-Nieto, Seco, & Preciado, 2014, p. 87; Kaya, Isik, Senyuva, & Kaya, 2016, p. 3). No other profession incurs more of a moral obligation to serve its constituents than nursing. When polls repeatedly endorse nursing as the most trustworthy of all professions (Norman, 2016), “teaching and learning ethical comportment requires … good curricular and pedagogical development” and should be uppermost on the minds of nursing faculty (Benner, Sutphen, Leonard, & Day, 2010, p. 167). And yet, while the nursing curriculum is the ideal breeding ground to build students’ moral courage values, few studies describe how these values were embedded in any nursing curriculum, much less an accelerated bachelor’s degree in nursing (ABSN) curriculum.
Literature Review
Numminen, Repo, and Leino-Kilpi (2017) reviewed the concept of moral courage in nursing, to conclude that despite the ambiguity and elusiveness of its definitions, moral courage remains closely related to nursing values (p. 11). They analyzed 31 studies for seven core attributes of moral courage in nursing including true presence, moral integrity, responsibility, honesty, advocacy, commitment and perseverance, and personal risk, and their relationship to being and “acting as a courageous nurse” (pp. 5–6). Moral courage, they concluded, needs more comprehensive definitions, better connections with theory, and broader, deeper research on morally courageous behaviors—all aimed at educational programs and nursing management as they strive to develop nurses’ moral courage (p. 11).
The call for “consistent demonstration of core values by nurses and other professionals to achieve optimal health and wellness outcomes” has been well documented (American Association of Colleges of Nursing, Essential VIII, 2008, pp. 26–27). The ethical demands of health care hold nurse educators responsible for developing the value-based behaviors of nursing students. Iacobucci, Daly, Lindell, and Griffin advised that nursing curricula must “contribute to the feelings of preparedness and proactive coping behaviors [students need] when facing an ethical dilemma” (2012, p. 488).
Murray (2010) aptly referred to venues where nurses must demonstrate moral courage such as the classroom, the boardroom, even the waiting room. Weiss and Schank (2000) concurred that values are beliefs that individuals and groups uphold. They distinguished between personal and professional values: Personal values reflect individual attitudes, while professional values are standards for action preferred by practitioners and professional groups and provide a framework for evaluating behavior (Weiss & Schank, 2000, p. 201).
Examples of morally stressful situations and unethical behaviors are documented in academia, sports, entertainment, research, and health care (Kidder, 2005b; Murray, 2010; Zangaro, Yager, & Proulx, 2009). College students—regardless of the area of study—grapple with morally tempting situations such as copying a classmate’s answers with or without permission; neglecting to report a colleague's cheating; outsourcing an assignment, then submitting it as original work; or claiming research as one’s own without crediting the author (Blum, 2009; Payan, Reardon, & McCorkle, 2010; Retherford, 2011).
Regardless of feeling a moral obligation to act, nursing students may “lack the moral courage to intervene or speak up when faced with poor practice” (Bickhoff et al., 2017, p. 71). Despite claiming they “want to do what is in the best interest of their patients”—nursing students described feeling unqualified or unprepared enough to provide quality patient care (Escolar-Chua, 2016, p. 1). They reported instances of ignoring when patients were given insufficient information to sign an informed consent; ignoring the call bell for a patient with an infectious disease; and not taking action after a colleague admitted administering the wrong medication (Escolar-Chua, 2016; Nash, Mixer, McArthur, & Mendola, 2015). Several studies found that regardless of feeling a moral obligation to respond, most millennial nursing students (aged 22–37 years) were reluctant to advocate for their patients or to assert themselves during morally stressful situations (Bickhoff et al., 2017; McLeod-Sordjan, 2013).
Benner et al. (2010) emphasized that teaching ethical comportment and the acquisition of professional nursing values are achieved by engaging students “with clinical problems and particular patients and patient populations, [to] broaden their moral imagination, just as they broaden it by literature, nursing knowledge, bioethics, and the ethics of care and responsibility” (pp. 166–167).
College students, including nursing students, hesitate—even refuse—to address morally stressful situations for reasons of inexperience, limited ethical knowledge, lack of ethical confidence, fear of retaliation, or even fear of litigation (Bickhoff et al., 2017; Escolar-Chua, 2016, p. 1; Iacobucci et al., 2012). Hoskins, Grady, and Ulrich chronicled the gaps of ethics education in nursing curricula and the importance of ethics education in academic and clinical settings (2018). Murray (2010) advised that “most scholars who study ethics agree … that everyone, regardless of profession, can benefit from education and training in the area of moral courage” (See Developing Moral Courage in the Face of Ethical Challenges).
Purpose
The purpose of this study was threefold. First, to describe a moral courage campaign instituted in an ABSN curriculum. Second, to outline the curriculum redesign process to build moral courage values in its ABSN courses. And third, to compare faculty perceptions of 29 ABSN students’ honesty, respectfulness, responsibility, fairness, and compassion (Kidder, 2005a, 2005b) 4 weeks after beginning and again at the end of the 12-month ABSN program. Examples of course and clinical objectives were aligned with relevant teaching-learning activities.
Methods
Curriculum Redesign Process
The process to embed moral courage values in the nursing curriculum began with the faculty’s analysis of the recently revised College Mission and its emphasis on justice and ethics: The College empowers its community of learners to excel, lead, and serve with integrity and to engage responsibly in the pursuit of a more just, ethical and sustainable world. (Dominican College, 2015a) Grounded in the liberal arts, the nursing curriculum assists students to learn reflective understanding and compassionate involvement, and a sense of ethical, civic, and social responsibility. (Dominican College, 2015b)
Theoretical Foundation
During earlier stages of their curriculum design, the nursing faculty designated Rogers’ Science of Unitary Beings (1986) and Watson’s Theory of Transpersonal Caring (1988a, 1988b) as the theoretical foundation of their nursing curriculum. They agreed that Rogers (1988) understood the importance of moral courage when she wrote: “the future demands new visions, flexibility, curiosity, imagination, courage, risk-taking, [and] compassion … ” (pp. 99–102). They supported Rogers’ emphasis on the “inseparability of one's values and one's work” (Butcher, 1999, p. 116).
At the same time, the faculty endorsed Watson’s (1988a) moral, ethical, and philosophical emphases in all nursing curricula (p. 422). They supported Watson’s statements that “ethical caring is the essence of professional nursing … [and] the most central and unifying source to sustain its covenant to society … ” (Sitzman & Watson, 2017, p. 5). Rogers’ and Watson’s philosophies affirmed the moral courage campaign they sought to implement.
Moral Courage Campaign
Recognizing the fundamental role of moral courage and moral courage values in ethical decision-making and the disappointing condition of moral courage in nursing curricula worldwide (Choe, Kang, & Lee, 2013; Escolar-Chua, 2016, p. 1; Gallagher, 2007; Hawkins & Morse, 2014; Lin, Wang, Yarbrough, Alfred, & Martin, 2010; Monteverde, 2014), the nursing faculty at Dominican College, in conjunction with the Nursing Division’s Curriculum Committee, embarked on a campaign to strengthen moral courage values in their ABSN curriculum.
To start, the faculty concurred that moral courage is the will to speak out and do the right thing, even when constraints or forces to do otherwise are present (Butts & Rich, 2013, p. 79). They affirmed that values are central to any act of moral courage and that “standing up for one’s values” was the defining feature of moral courage (Kidder, 2005b). They acknowledged that values are ongoing beliefs that define social and professional behavior and affect moral judgment (Rokeach, 1973, pp. 23–24), and they agreed that values are extracted from one’s cultural environment, education, societal norms, family traditions, religious principles, and life experience (Rassin, 2008, p. 628).
Moral Courage Values and Behaviors
The emphasis on ethical responsibility in the Missions of the College and the Division of Nursing and the relationship of moral courage values to nursing as an ethical practice inspired the faculty in this study to thread moral courage values throughout their 12-month ABSN curriculum. A one-group pre- and posttest study compared faculty perceptions of the 29 then enrolled ABSN students’ moral courage values 4 weeks after the program began and again just before their graduation.
Moral Courage Values and Behaviors.

ABSN Curriculum
Accelerated Bachelor of Science in Nursing (ABSN) Curriculum: 58 Credits.

Note. Numbers inside parentheses are the number of credits awarded per course.
aClinical Nursing Course.
Prior to starting the ABSN program, all students must have completed the minimum of a nonnursing bachelor’s degree plus 11 prerequisites—four social sciences, six sciences, and statistics. The ABSN curriculum is identical to the traditional 3-year nursing curriculum for the number of nursing courses, the credits allotted, and the classroom and clinical hours required. However, while each 5-credit nursing course in the traditional program takes place over a 15-week semester with one 3-hr class and one 6-hr clinical experience per week, the same course in the ABSN program takes place over 4 weeks, with two 6-hr classes and three 8-hr clinicals per week. Each student must achieve a minimum grade of B− (80%) for each nursing course and maintain a minimum 2.7 grade point average to advance to the next trimester. Given the compressed nature of the curriculum, and the structured sequence of its back-to-back courses, there is no opportunity to repeat a course while matriculating in the 1-year ABSN program. A student who is unable to progress academically in the ABSN program can apply to the 2-year weekend accelerated program or the 3-year traditional nursing program at the College.
The majority of ABSN courses are offered in a hybrid format and use an online learning system for announcements, course information, discussions, testing, and posting grades. NR 353 (Nursing Research) is the only course offered totally online. Clinical sites include acute medical-surgical units, medical-surgical intensive care units, in-house hospice, pediatric and psychiatric-mental health units, maternity and pediatric units, neonatal intensive care units, paramedic facilities, schools, shelters, and home care agencies. ABSN clinical groups range from four to eight students each.
ABSN Faculty and Student Characteristics
Thirteen of the 14 ABSN courses in this study were taught by faculty employed full time by the College and held the minimum of a master’s degree in nursing; two were additionally prepared at the doctoral level: one Doctor of Nursing Practice and one Doctor of Education in Higher and Adult Education. All clinical faculty held the minimum of a master’s degree in nursing, while two held a Doctor of Nursing Practice degree. All full- and part-time clinical faculty were certified in the discipline of their teaching assignments.
All students then enrolled in the ABSN program participated in the study. The 22 women and 7 men participants ranged in age from 21 to 39 years and held prior nonnursing college degrees in majors such as biology, finance, psychology, and teacher education. Most were single, some were parents, and many deferred outside employment for the duration of the program. They embodied the habits of inquiry and intellectual curiosity typical of accelerated nursing students looking to complete a bachelor’s degree in nursing: They were older, motivated, excellent learners, and eager to gain knowledge and clinical experience from their faculty (American Association of Colleges of Nursing, 2012).
Course Objectives and Teaching-Learning Activities
Examples of Course- and Clinical Objectives Aligned With Teaching-Learning Activities.

Survey Process
Once the teaching-learning activities had been embedded across the curriculum, the faculty planned to survey perceptions of their students’ moral courage values 4 weeks after beginning the ABSN program, and again just before graduation. After the first 4 weeks, the students had completed 2 of the 14 accelerated nursing courses: NR 223 (Introduction to Professional Nursing I), a 5-credit clinical nursing course comprised of 45 lecture hours and 90 clinical hours, and NR 229 (Pharmacological Agents), a 3-credit nonclinical nursing course comprised of 45 lecture hours—comparable in hours to the entire Fall semester of the Sophomore year in the traditional option at this institution.
Of the eight faculty expected to complete the first survey, four would have taught the ABSN students in both the classroom and the clinical agency, and four would have taught exclusively in the clinical agency. Of the eight faculty expected to complete the last survey, all were full time and would have taught the ABSN students in both the classroom and the clinical agency. Two nursing faculty reviewed the survey for content validity and their suggestions were incorporated. The Pearson correlation coefficient for the survey was calculated at r = .93, and the Spearman Brown prophesy formula established the expected reliability of the full instrument at r(e) = .96.
A minimal risk application was submitted to the internal review board of the College. Once the Board’s approval was obtained, the Informed Consent Form and initial Moral Courage Survey were administered as planned. The Consent Form acknowledged the purpose of the project, that participation was voluntary, that faculty could withdraw at any time, and that all surveys would be destroyed after 3 years. The Form guaranteed the anonymity and confidentiality of all survey responses.
Survey Components
Moral Courage Values and Ethical Questions Analyzed by Students in NR 467 (Nursing Seminar).

Note. RN = registered nurse; CPR = cardiopulmonary resuscitation.
Moral Courage Survey.

Note. ABSN = accelerated bachelor’s degree in nursing.
Directions: Given that moral courage is the bridge between talking ethics and doing ethics, with a readiness to endure danger for the sake of principle (Kidder, 2005b), please assess the moral courage dispositions and behaviors of the ABSN students, as an aggregate. Indicate with an X, your relative agreement or disagreement with each statement below, from Strongly Agree (SA) to Strongly Disagree (SD). All responses will be treated anonymously and confidentially.
Statistical Analysis
The results of the surveys indicated a significant positive change in four of the five the moral courage values of 29 students surveyed by their faculty from 4 weeks after beginning to just before graduation from an accelerated bachelor’s degree nursing program. t-test scores for honesty, responsibility, fairness, and compassion showed statistically significant growth, while respectfulness did not show statistically significant growth. The mean pretest scores ranged from 9.25 to 10.38, and the mean posttest scores ranged from 12.75 to 13.13. The growth for all five values ranged from honesty (with the most growth), to fairness, responsibility, compassion, and respectfulness (with the least growth).
Comparison of Early-in- and End-of-Program Surveys (Unpaired Samples t Test).
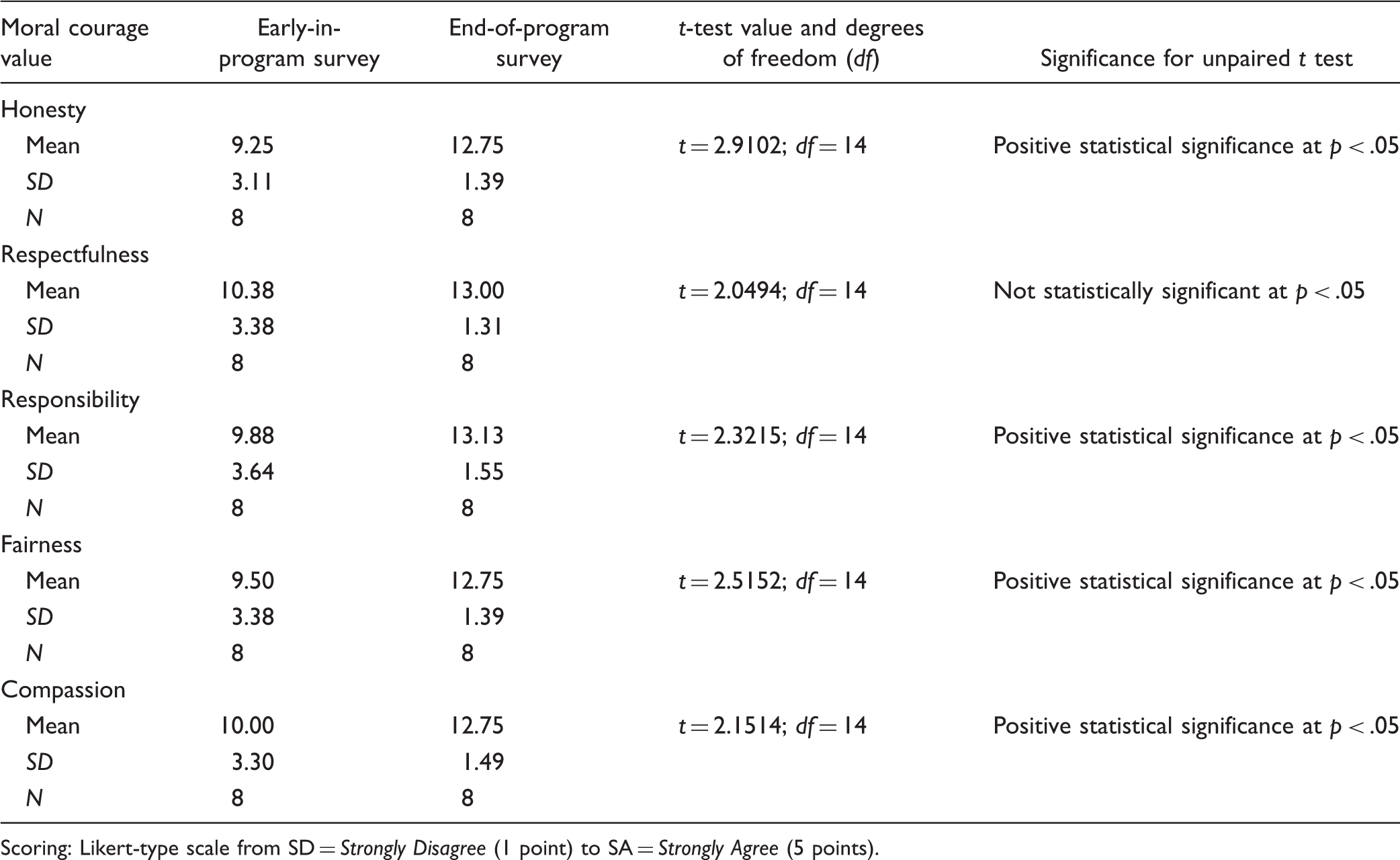
Scoring: Likert-type scale from SD = Strongly Disagree (1 point) to SA = Strongly Agree (5 points).
Results
ABSN Exit Questionnaire
Each year, the Office of Institutional Research at the College sends an exit questionnaire to its current ABSN graduates to assess the effectiveness of the ABSN curriculum. Twenty seven of the 29 ABSN graduates in this study responded. Of the 20 learning outcomes on the questionnaire, five aligned with the moral courage values specified in this study. The 5-point response scale ranged from Not at All, to Somewhat, Moderately, Well, and Extremely Well. The Well and Extremely Well responses for these five values and their outcomes ranged from 73% to 82%:
Respectfulness: collaborating with health-care teams (73%; Mean: 3.73/5.0) Responsibility: using technology to assess sociopolitical, ethical, and historical issues related to nursing practice (73%; Mean: 3.77/5.0) Compassion: making and defending ethical decisions related to health-care issues (78%; Mean: 3.81/5.0) Honesty: providing and evaluating nursing care for patients and their families (78%; Mean: 3.85/5.0) Fairness: understanding sociocultural diversity and cultural competence (82%; Mean: 4.00/5.0)
Discussion
Although this study supports the premise that the nursing curriculum can strengthen students’ moral courage values, a direct correlation cannot be presumed. The results do however shed a positive light on the influence of education on values formation and the importance of teaching-learning activities related to moral courage values that are systematically embedded across the nursing curriculum (Lin et al., 2010, p. 652). The importance of incorporating teaching-learning activities that promote moral courage values cannot be dismissed, especially when there is no designated ethics course in the nursing curriculum (Bosek & Savage, 2007, p. 39), as was the case in this study.
Strengths and Limitations
After defining the five moral courage values they deemed most important in nursing practice, the faculty designed teaching-learning activities across the curriculum for students to learn, develop, and implement them. Surveys of the progress made were significantly positive for honesty, responsibility, fairness, and compassion—each an integral aspect of ethical decision-making. However, since this study was limited to an ABSN class of 29 students at one institution, similar studies in traditional baccalaureate nursing programs and associate degree programs are warranted. As with any research, the results and conclusions of this project must be acknowledged with caution and repeated in other ABSN programs. Other factors that could have led to the difference seen in the pre- and postfaculty surveys are the extent of the students’ experience in the clinical setting, the impact of the nursing faculty as role models, and the influence of culture and politics on values formation.
Implications
Building the moral courage values of nursing students through curriculum design holds promise for nursing practice worldwide. Follow-up studies after 1 year of nursing practice could determine if the growth of the values in this study was sustained. Surveying faculty perceptions of students’ values in several nursing programs at the same time would increase the number of student and faculty participants and the likelihood of generalizing the results. Analyzing teaching-learning activities to develop moral courage values in clinical nursing courses could distinguish the theoretical acquisition of one’s values from their clinical implementation. Comparing teaching learning activities to build the moral courage values of nursing students worldwide would be valuable given the increased focus on population-based health care.
Conclusions
When society consistently trusts that nurses hold moral courage values strong enough to make ethical decisions that protect them (Norman, 2016), the nursing curriculum is a prime opportunity to build and measure those values. The teaching-learning activities described in this study aimed to promote the ABSN program objective that the student will demonstrate proficient communication skills as well as clinical, technological, and ethical competence in the delivery and management of health care.
Kidder and Bracy (2001) remind us that “finding ways to establish and enhance a culture of moral courage is surely one of the noblest goals of humanity” (p. 13). In this study, systematic curriculum redesign driven by a solid theoretical foundation and unwavering faculty perseverance contributed to significantly positive perceptions by faculty for four of the five moral courage values surveyed. Three criteria supported the moral courage development in this study—awareness, passion, and energy: awareness from “staying-in-touch” with one’s environment (Rogers, 1988); passion from believing in the power of one’s values (Kidder, 2005b); and energy from the feedback incurred by using moral courage to generate the healing and wholeness of others (Watson, 2008).
We cannot overestimate the importance of moral courage in nursing practice or in nursing education (Gallagher, 2010). When nursing faculty believe their students must serve the common good, they are obliged to strengthen moral courage in their curricula. Kidder and Bracy (2001) leave us with no choice: “Without it, our brightest virtues rust from lack of use. With it, we build piece by piece a more ethical world” (p. 2).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.