
Abstract
Background
Cardiac surgeries rank among the most frequent surgical procedures and present a risk of chronic postsurgical pain (CPSP). A continuum approach is required to prevent the development of CPSP. As a first step, a tailored web-based intervention was developed and successfully tested to tackle pain management during hospitalization. Before proceeding to further development, preliminary acceptability of the intervention including the postdischarge phase must be evaluated.
Purpose
The purpose of this study was to examine nurses’ perception of a tailored Web-based intervention for pain management in the early recovery phase. The objectives were to evaluate intervention’s acceptability and to identify ways to enhance its acceptability.
Methods
A parallel mixed methods approach was used to assess the acceptability of the intervention in the early recovery phase (first month after surgery).
Results
In total, 249 participants completed the online survey and 10 participants were individually interviewed. Overall, the intervention was rated as acceptable. No difference was found in acceptability ratings by demographics. The intervention was rated as appropriate to very much appropriate by 79% of participants. Although nurses seemingly would recommend it to their patients, they did not perceive that their patients would be as highly willing to use it. Interviews highlighted several strengths of the intervention, such as postoperative pain awareness, customization of content, and flexible dosage and schedule. However, the main weakness was related to patient adherence. Opting for a hybrid format and integrating individual preferences could enhance the coaching experience.
Conclusion
The innovative intervention was judged as acceptable for pain management in the early recovery phase. Considering that the intervention has demonstrated positive effects on the pain experience in the first week after cardiac surgery, it seems logical to explore its potential impact after discharge on the transition to CPSP.
Introduction
Death rate caused by cardiovascular diseases has decreased because of progress in cardiac surgery (Mozaffarian et al., 2015). However, about two thirds of patients suffer from moderate to severe pain in the 7 days after surgery, which predicts the presence and severity of pain after discharge and is a risk factor for the development of chronic postsurgical pain (CPSP) (Choiniere et al., 2014; Guimaraes-Pereira, Reis, Abelha, Azevedo, & Castro-Lopes, 2017; Kamalipour, Vafaei, Parviz Kazemi, & Khademi, 2014). Indeed, a recent meta-analysis found that CPSP affects 37% of patients in the first 6 months and is present for more than 2 years in 17% of adults following cardiac surgery, with 50% reporting moderate to severe pain intensity (Guimaraes-Pereira et al., 2017), potentially compromising their recovery and daily functioning (Choiniere et al., 2014; Guimaraes-Pereira et al., 2017; Kamalipour et al., 2014).
Sex and gender differences are individual risk factors that have gained great interest in pain-related research in general. These differences are currently an important concern in the context of postoperative pain after cardiac surgery where women have been underrepresented (Bjornnes, Parry, et al., 2016; Bjornnes, Parry, Leegaard, et al., 2018; Bjornnes, Parry, Lie, et al., 2018; Parry et al., 2018). Previous studies on pain after cardiac surgery indicate that sex is an independent predictor of CPSP with more women experiencing relatively high levels of pain up to 2 years postoperatively (Choiniere et al., 2014; Van Gulik et al., 2011). Women also report more pain interference with daily activities than men at 1 month and 12 months after surgery (Bjornnes, Parry, et al., 2016; Parry et al., 2010).
Various other risk factors have been highlighted and considerable advances have been made in understanding the transition from acute to CPSP (Katz & Seltzer, 2009; Katz et al., 2015; Kehlet, Jensen, & Woolf, 2006). These factors include perioperative pain and use of opioids, and negative affect reflected in pain-related attitudes (Choiniere et al., 2014; Fletcher et al., 2015; Van Gulik et al., 2011). Patients’ attitudes regarding pain and its relief partially explain inadequate levels of analgesia in the immediate postoperative phase, but also 12 months after surgery (Bjornnes, Parry, et al., 2016; Bjornnes, Rustoen, Lie, Watt-Watson, & Leegaard, 2016; Cogan et al., 2013; Martorella, Cote, Racine, & Choiniere, 2012; Watt-Watson et al., 2004). Moreover, it has been shown that pain cognitions, such as pain catastrophizing, influence postoperative pain intensity and activity levels contributing to the development of CPSP (Burns et al., 2015; Khan et al., 2011, 2012; Theunissen, Peters, Bruce, Gramke, & Marcus, 2012).
In an effort to address postoperative pain and its potential transition to CPSP, risk factors need to be targeted in the different perioperative phases (Katz & Seltzer, 2009; Katz et al., 2015). Hence, findings suggest that postcardiac surgery patients could benefit from a pain management intervention, not only during the perioperative period, but also after discharge from the hospital (Bjornnes et al., 2017; Fredericks & Yau, 2013; J. Lapum, Angus, Peter, & Watt-Watson, 2011; J. L. Lapum et al., 2016; Martorella, Gelinas, & Purden, 2014). However, very few interventions for this population include both of these phases, and of those which have, they are usually not tailored to CPSP risk factors (Guo, 2015; Koranyi, Barth, Trelle, Strauss, & Rosendahl, 2014; Ramesh et al., 2017). Information technologies can support patients and clinicians in a busy care setting and contribute to improving clinical outcomes in the perioperative setting (Van Der Meij, Anema, Otten, Huirne, & Schaafsma, 2016). Tailored Web-based interventions have multiplied over the past decade to address pain management. Albeit, they mainly target chronic pain, allowing opportunities for the development of interventions aimed at acute pain and its transition to chronic pain (Martorella et al., 2017).
Background
A tailored Web-based intervention for the self-management of pain after cardiac surgery was developed to tackle pain in the immediate postoperative phase (Martorella, Cote, & Choiniere, 2013). This intervention consists of a brief assessment of two risk factors, that is, patients’ pain-related attitudes and pain catastrophizing, and a 30-minute tailored preoperative session on a laptop computer coached by a virtual nurse (see Figure 1). Based on this assessment, information and strategies are then specifically tailored to the participants’ profile according to an algorithm. Two tailored reinforcements of 5 to 10 minutes are also provided in person after surgery. A pilot randomized controlled trial (N = 60) was conducted (Martorella et al., 2012). Findings provided evidence that the intervention was feasible and helpful in minimizing pain interference with several postoperative activities, especially breathing and coughing in the first few days after surgery. The intervention also influenced the way people coped with pain in modulating some individual barriers toward pain relief and opioid analgesic consumption. One month after discharge, patients’ perception of the intervention were quite positive and similar between women and men, although they differed in their reasons for its acceptability (Martorella et al., 2014).
Tailored web-based intervention’s home page.
These results substantiate the need for the development of an updated version of the current intervention (Martorella et al., 2013) that encompasses the postdischarge phase (first month). Although the required dose of intervention in this phase is still unclear (Veronovici, Lasiuk, Rempel, & Norris, 2014), a qualitative study underlined that providing support in the first few weeks after discharge is important for patients after cardiac surgery (J. L. Lapum et al., 2016). It is then proposed to add two sessions in the early recovery phase (first month postdischarge), which would require additional content. However, before proceeding to further refinement, as it was done with patients, it is essential to evaluate nurses’ perceptions of the intervention and its possible expansion. Health-care professionals who judge an intervention as unacceptable to patients may avoid it and not recommend it or use it (Sidani & Braden, 2011). Acceptability, the extent to which people delivering or receiving a health-care intervention consider it to be appropriate (Sekhon, Cartwright, & Francis, 2017), must be examined for interventions that are in the process of being refined in terms of content, mode of delivery or dose, or being implemented in a newly selected setting (Sidani & Braden, 2011).
Therefore, the purpose of this study was to examine nurses’ perceptions of a tailored Web-based intervention aimed at improving pain control in the early recovery phase of cardiac surgery. The objectives were two-fold: (a) to evaluate intervention’s acceptability (perceived effectiveness, appropriateness, suitability, and willingness to adhere) from the perspective of nurses caring for patients undergoing cardiac surgery and (b) to identify ways to modify aspects of the intervention to enhance its acceptability for the hospitalization and postdischarge phases.
Methods
Design
A parallel or convergent mixed methods design (QUAN + QUAL; Creswell & Plano Clark, 2017) was used to assess the acceptability of the preliminary version of the intervention for pain management after cardiac surgery including both the hospitalization and the postdischarge phases (i.e., early recovery). This design allowed us to describe to which extent the intervention is acceptable and in what ways. Quantitative and qualitative data were collected concurrently, compared and combined to offer a more comprehensive understanding of nurses’ perception. A mixed methods convergent study design combines the strengths of both quantitative and qualitative approaches and have been recognized as a relevant approach for addressing contemporary and complex issues in health services research (Fetters, Curry, & Creswell, 2013).
Sample and Data Collection
After obtaining approval from the Florida State University institutional review board, quantitative data were collected between May and June 2017 through an online survey (Qualtrics©). Based upon an a priori sample size calculation using GPower for a one-way analysis of variance Main Effects F test, an α = 0.05, medium standardized effect (0.25), three groups (clinical setting: inpatient, outpatient, other), and power = 0.8, 159 participants were needed for this study. Participants were included in the study if they had at least 2 years of experience working with the cardiovascular surgical population.
Outline of the Proposed Intervention Presented During the Survey and Interviews.

Note. CPSP = chronic postsurgical pain.
In order to complement quantitative data and identify the intervention’s refinement possibilities, qualitative data were collected through individual face-to-face interviews with a convenience sample of 10 nurses (Guest, Bunce, & Johnson, 2006; Hennink, Kaiser, & Marconi, 2016) working with cardiovascular surgical patients for at least 2 years. Participation in individual interviews was advertised through the Florida State University, College of Nursing's Facebook page. Anyone interested was invited to contact the Principal investigator (PI). During the 45-minute interview conducted by a trained research assistant, participants read a description of the intervention supported by screenshots of Web pages. Interview participants were asked to rate the intervention prior to initiation of the semistructured individual interview. A semistructured interview guide was used to facilitate discussion.
Instruments
Sociodemographic questionnaire
A researcher-developed survey was used to gather the following sociodemographic data: age, sex, level of education, clinical role, clinical practice setting, years of experience with the cardiovascular surgical population, specific pain management training (y/n), and experience working in a pain clinic (y/n). A questionnaire also was developed by two of the investigators (GM, CG) to assess knowledge about CPSP. This CPSP questionnaire included 10 Likert-type items on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). The questionnaire was not validated but the specific items can be found in the Results section.
Treatment Acceptability and Preference questionnaire
The Treatment Acceptability and Preference (TAP) questionnaire is a valid and reliable instrument used to measure an intervention’s acceptability (Sidani, Epstein, Bootzin, Moritz, & Miranda, 2009). The specific intervention acceptability attributes included in this questionnaire are: (a) effectiveness in managing the problem, (b) intervention appropriateness, (c) suitability of the intervention to individual reality, and (d) convenience or willingness to apply and adhere to the intervention. The intervention acceptability questionnaire in this study included: (a) effectiveness in promoting pain self-management (4 items), (b) appropriateness in helping patients manage pain (2 items), (c) suitability (4 items), and (d) willingness to adhere (2 items). The specific items can be found in the Results section. The ratings refer to a 5-point scale ranging from not at all (0) to very much (4). A total scale score between 0 and 4 is obtained based on a mean of the four attributes’ subscales to reflect perceived intervention acceptability. The four items previously demonstrated internal consistency reliability in a population receiving behavioral interventions for insomnia (α > .80; Sidani, Epstein, et al., 2009). Validity was confirmed through factor analysis and discriminant validation as well (Sidani, Epstein, et al., 2009).
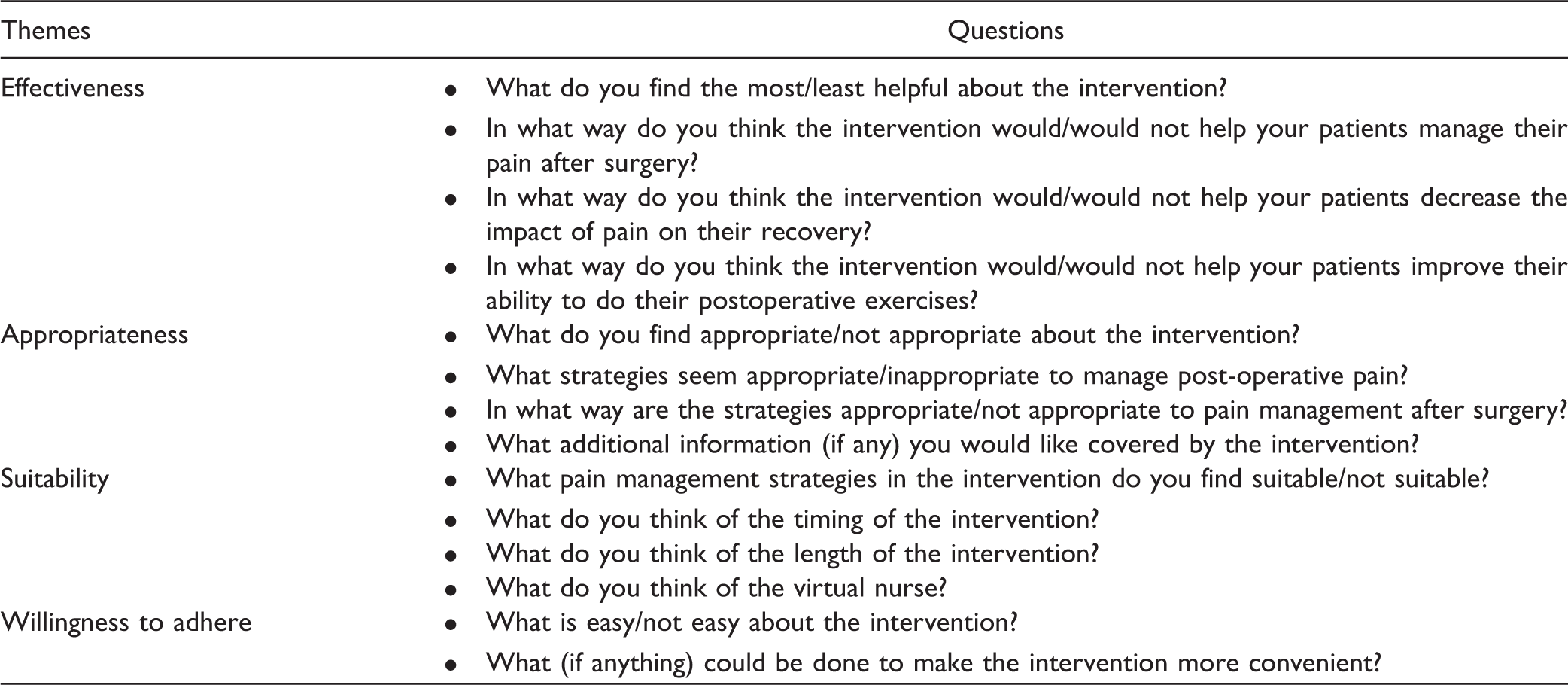
Semistructured interview guide
SemiStructured Interview Guide.
Data Analysis
Quantitative data
Sociodemographic characteristics (i.e., years of experience, clinical setting, role, CPSP knowledge) and TAP questionnaire scores were analyzed descriptively. Frequency tables, means, and standard deviations (SDs) were used to summarize data for each item and the total score on the TAP measure. One-way analysis of variance was conducted to determine differences in acceptability ratings among sociodemographic variables.
Qualitative data
Individual interviews were digitally recorded and transcribed verbatim, with concurrent data collection and analysis. NVivo™ software was used to analyze the transcripts and to generate themes derived from clinicians’ perceptions of the intervention and its acceptability (Miles & Huberman, 1994). A preliminary generation of codes was based on the attributes of acceptability highlighted by Sidani et al. (Sidani & Braden, 2011; Sidani, Epstein, et al., 2009): appropriateness, effectiveness, suitability, and willingness to adhere. Additional codes (subcategories) were created when necessary. To ensure reliability, double coding was conducted by the primary investigator (GM) and the research assistant. Discrepancies were discussed until a consensus was reached. Frequency counts were conducted to validate the emergence of a theme and participants were contacted when necessary to validate findings.
Results from the two data sets were then merged and synthesized in order to discuss how they converge or diverge. Examination of qualitative and quantitative data assisted understanding of the intervention’s acceptability (Creswell & Plano Clark, 2017).
Results
Sociodemographic and Clinical Characteristics
Sociodemographic Profile of Participants.
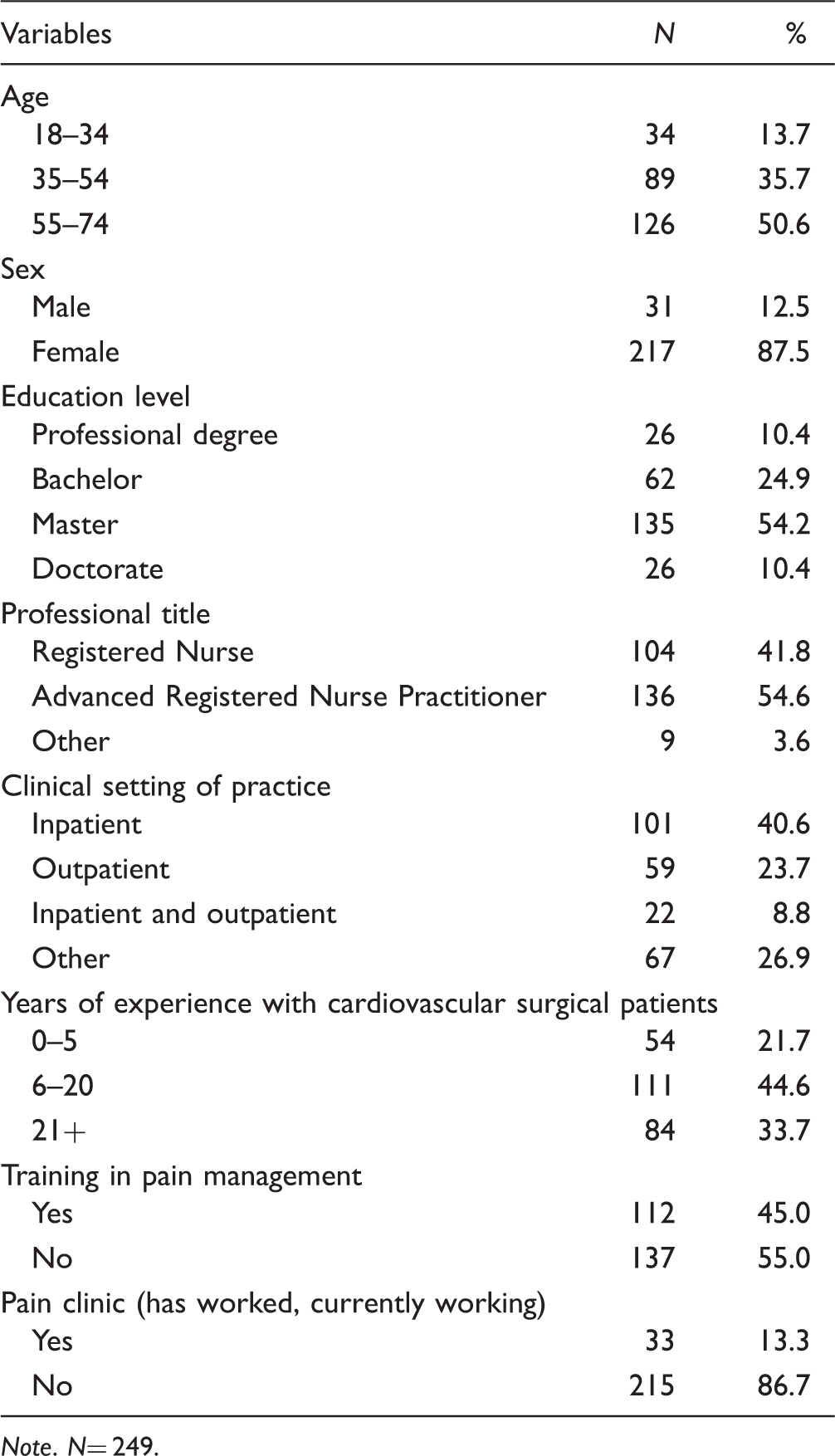
Note. N= 249.
CPSP knowledge
Mean (SD) for Each Item Related to CPSP Knowledge.

Note. SD= standard deviation.
Acceptability of the Intervention
TAP Mean Scores and Frequencies.

Note. SD= standard deviation; TAP= Treatment Acceptability and Preference.
Strengths and Weaknesses of the Intervention
Content Analysis Summary of Individual Interviews With Nurses.

Note. n= 10.
Effectiveness
When questioned about the effectiveness of the intervention, strengths were noted. Most of the time nurses found that the intervention provided patients an opportunity for increased awareness about postoperative pain and its management. This awareness included both postoperative pain representation as a mental preparation and also expectations regarding postoperative recovery and how the team will work with them. The intervention was perceived as a tool that equips patients with a better mindset and will help them cope with pain both during hospitalization and postdischarge. By equipping them, nurses thought that it would decrease some fears, engage them in their recovery, and allow better outcomes.
Appropriateness
When asked about appropriateness of the intervention, again several strengths were discussed. The main theme that emerged was customization both in terms of content and dosage of messages. Nurses appreciated the fact that patients’ individual experience and needs are acknowledged by tailoring the content of messages based on their on-screen answers and choices. Customization also addressed individual needs in terms of reinforcements or repetitions and learning pace. Repetition of information seemed to be an important aspect of education in this clinical setting. Hence, nurses saw some benefit in the flexibility of the Web application, allowing patients to pause, repeat, or go back at their convenience.
Suitability
When asked about suitability, the length of sessions was not an issue. Nurses also agreed on the benefits of using other patients’ stories to normalize the experience. The main theme that emerged in regard to format preferences was the provision of guidance and technology usability. Both strengths and weaknesses were identified. When asked about using videos of a nurse, most nurses appreciated that the application creates an individual nursing consultation and that the information is not just a text to read. According to the nurses interviewed, the presence of a nurse also added some credibility to the educational content. However, one nurse remained reserved mentioning that she preferred human contact. The Web-based format also generated some concerns about the usability in elderly patients, while others thought it was a great idea as many patients are now using smartphones or tablet computers.
Willingness
Both willingness of patients to comply with the intervention and willingness of nurses to recommend the intervention to their patients were discussed as a supplement to usual care. Some weaknesses were identified. The willingness of patients to comply with the intervention after discharge was the main concern. Different reasons were mentioned, such as living alone, being exhausted or depressed after surgery, and lack of motivation in general. Hence, the Web-based intervention seemed to be more acceptable if combined with guidance and monitoring from nurses (e.g., telephone or face-to-face). The willingness of nurses to recommend the intervention to their patients seemed to be influenced by their involvement in the success of the intervention. According to those interviewed, the Web-based intervention should be integrated and complementary to nursing care.
Discussion
This mixed methods convergent study sought to examine nurses’ perception of a tailored Web-based intervention for pain management after cardiac surgery (i.e., hospitalization and postdischarge phase). This approach is innovative by targeting CPSP risk factors before surgery, immediately after and in the first month postdischarge. The intervention was reported as acceptable by nurses and appropriate for pain management after cardiac surgery by the majority of respondents. Moreover, more than 80% of nurses would be willing to recommend it to their patients.
Acceptable Intervention Components
The intervention was rated as being effective for both the hospitalization and postdischarge phases mainly because of its potential to increase patients’ awareness of postoperative pain. This finding supports the perception of patients (Martorella et al., 2014). A recent study found that 80% of patients (n = 1,481) were unaware of the risk of persistent postoperative pain underlining the need for clinicians to discuss this significant risk with patients (Oliver, Kashef, Bader, & Correll, 2016). This finding is even more concerning considering that beliefs and attitudes toward pain and its treatment are common in this population and impede proper pain management (Cogan et al., 2013; Martorella et al., 2012). The intervention, not only provides information on pain management, but responds to the current needs of clinicians and patients in terms of CPSP prevention.
The intervention was rated as appropriate for pain management after cardiac surgery, with customization in terms of content and dosage being the most important feature. Tailoring has been previously acknowledged by nurses as an important component of interventions for this population (Fredericks, 2011; J. L. Lapum et al., 2016). Previous findings have specifically identified that standardized delivery of information, as opposed to tailored, affected the application of strategies by patients in their own lives (J. L. Lapum et al., 2016). Moreover, tailoring strategies allow targeting specific health determinants, such as risk factors for CPSP (Hawkins, Kreuter, Resnicow, Fishbein, & Dijkstra, 2008).
The schedule of the intervention (i.e., preoperatively and first month postdischarge) was also rated as appropriate. The preoperative period is a traditional timeframe for education in this population (Koranyi et al., 2014; Ramesh et al., 2017). However, when targeting the postdischarge phase, traditional interventions usually take place postoperatively at discharge while in the hospital, which has been recognized by both nurses and patients as not allowing an adequate amount of time for education (J. L. Lapum et al., 2016). Previous findings support the need for interventions during the early recovery phase at home (Bjornnes et al., 2017; Fredericks, 2009; Fredericks, Sidani, & Shugurensky, 2008; J. L. Lapum et al., 2016). The possibility to receive information reinforcements according to needs, and individual pace and convenience was clearly perceived as an advantage by nurses similarly to patients’ perceptions (Martorella et al., 2014). Web-based interventions offer this flexibility and have the potential to facilitate the delivery of perioperative interventions during the postdischarge phase (Van Der Meij et al., 2016).
Avenues for Improvement
Nurses identified two aspects of the intervention’s format that could be improved to optimize patient’s adherence to the intervention. Although the use of patients’ stories and videos of a nurse were rated as suitable, ease of use by patients, in terms of computer literacy, seemed to be more of a concern for nurses. Individual interviews corroborated this result. Moreover, in a previous study examining patients’ acceptability, the Web-based format was also identified as a potential barrier in the home setting (Martorella et al., 2014). Although participants had come to the conclusion that it was easier after a few minutes of use, this finding should be taken into consideration for further development. Nevertheless, patients’age seems to be less and less of an issue. A recent report from the Pew Research Center highlighted that seniors have similar use of technologies than adults under 65 of age. Demographic variables such as education and income levels are more determining (Anderson & Perrin, 2017). Moreover, undergoing a cardiac surgery is a stressful experience that can impede the use of technology. Evidence-based guidelines, such as those from the Office of Disease Prevention and Health Promotion of the U.S. Department of Health and Human Services (2016) can easily help improve and promote e-Health literacy.
Also, while nurses would recommend the intervention to their patients, they rated their patients’ willingness to comply with the intervention lower, with the interviews illustrating that patients may not comply with the intervention during the postdischarge phase if it relies solely on technology. This finding is similar to previous studies with this population highlighting the need for supportive follow-up in the home setting where patients could be coached in their daily life, as well as share their concerns (Bjornnes et al., 2017; J. L. Lapum et al., 2016; Parry et al., 2018; Veronovici et al., 2014). Some participants discussed the possibility of including contacts with clinicians in the postdischarge phase. This could not only increase adherence, but also provide technical support if needed. Interestingly, frequent contacts with health-care providers have been recognized as a significant ingredient to improve adherence to Web-based interventions by providing additional support through presence (Baumeister, 2014; Kelders, Kok, Ossebaard, & Van Gemert-Pijnen, 2012; Mohr, Cuijpers, & Lehman, 2011). Of note, hybrid formats, (e.g., addition of face-to-face or telephone contacts), are predominant in Web-based interventions for chronic pain, including tailored approaches (Buhrman, 2016; Martorella et al., 2017). Moreover, this alternative has also been recently used and successful in a trauma population also at risk of developing chronic pain after experiencing acute pain during their hospitalization (Berube et al., 2018; Bérubé et al., 2018). Besides, adding contacts with clinicians raises the question of dosage (how frequent and how long). This aspect of the intervention could be tailored as patients with moderate to severe levels of pain intensity or pain interference with activities could necessitate more contacts (Bérubé et al., 2018).
Last, enhancing patient engagement could be reached by making the intervention more relevant to specific subgroups and according to their preferences. Treatment preferences are determined by sociodemographic factors and they can influence adherence and clinical outcomes (Mills et al., 2006; Sidani, Epstein, & Miranda, 2006; Sidani, Fox, & Epstein, 2017; Sidani et al., 2015; Sidani, Miranda, Epstein, & Fox, 2009). For instance, the acceptability study with patients underlined that women felt that the most important aspect of the intervention was the awareness-raising content, while men focused on the convenience of the support provided (Martorella et al., 2014). It was also found that promoting hope, particularly for women living alone, could improve outcomes after cardiac surgery (Bjornnes, Parry, Lie, et al., 2018). Another study with patients suffering from chronic musculoskeletal pain illustrated the importance of sociodemographic factors in showing that women had better levels of pain acceptance while men experienced more fear of movement (Rovner et al., 2017). These gender differences in the pain management individual experience are determinant factors of the intervention’s success as they generate different therapeutic strategies.
Integrating these improvements could require a series of iterative cycles of formative and evaluative research (Whittaker, Merry, Dorey, & Maddison, 2012). Hence, incorporating iterative cycles involving end users will also serve as a means to enhance patient engagement, especially in the context of a chronic condition (Whitehead & Seaton, 2016). Moreover, the same way it was done for the development of the first version of the intervention (Martorella et al., 2013), this process will also involve clinical and policy decision-makers to ensure the future implementation of the intervention (Sidani & Braden, 2011; Whittaker et al., 2012).
Limitations
A few limitations can be outlined. Although the sample size is large, response rate could not be calculated, which keeps us from evaluating the risk of a nonresponse bias. In addition, participants in the sample were self-selected which could lead to bias in the results. Of note, a majority of respondents had a graduate level of studies (64.6%) which could have influenced their responses. For instance, they could be more willing to suggest the intervention through their practice being more influenced by evidence-based standards. Also, many respondents (40.6%) were practicing in an in-patient clinical setting. Acute care settings leave little opportunities for patients’ empowerment and autonomy which could hinder nurses’ acceptability for an intervention of this type. Last, the level of technology acceptance by nurses determined by various individual, contextual, and organizational factors could have influenced their acceptability perceptions of the intervention but were not assessed (Gagnon et al., 2012; Gagnon, Ngangue, Payne-Gagnon, & Desmartis, 2016). For instance, perceived usefulness, perceived ease of use, and attitudes toward technology are variables influencing the successful implementation of technology-based health interventions (Strudwick, 2015).
Conclusion
This mixed methods study described nurses’ perception of a tailored Web-based intervention for pain management in order to prevent CPSP. The results of the interviews and survey were merged and integrated to inform and guide further development of the intervention.
Nurses perceived the intervention as acceptable and appropriate for the early recovery phase and would recommend it. They highlighted the importance of several components, such as postoperative pain awareness, customization of content, and flexible dosage and schedule. One of the concerns was related to patients’ capability of using a Web-based format. Opting for an hybrid format seems to be a promising avenue to improve patients’ adherence, especially after discharge. This would allow to combine the flexibility of the Web-based format with an enhanced coaching experience through human contact. Moreover, integrating gender preferences in the intervention content seems to be a key ingredient for success.
Prior work has demonstrated the potential to influence postoperative pain experience with a brief intervention if educative messages are tailored and personally relevant for the individual. Considering that the intervention has demonstrated positive effects on the pain experience in the first week after cardiac surgery, a logical extension of this research is to explore its potential impact on pain after discharge and on the transition to chronic pain. After further refinement and large-scale evaluation, if results are positive among the cardiac surgery patients, the intervention could easily be adapted and offered to different patient populations experiencing postoperative pain and at risk of developing CPSP. Nurses are ideally situated to intervene in the prevention of pain at all levels of the perioperative continuum of care and this type of intervention can support them in fulfilling that mission.
Footnotes
Authors' Note
Geraldine Martorella is also affiliated with College of Nursing, Florida State University. Lucinda Graven and Glenna Schluck are also affiliated with TMH Center for Research and Evidence-Based Practice, College of Nursing, Florida State University.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Martorella received funding from the Florida State University Council on Research and Creativity and College of Nursing.