
Abstract
Registered nurses (RNs) in heart failure (HF) nursing care have a key role in providing family support, which positively affects the outcome for the patient. Telephone interventions conducted by RNs have been reported to be successful in HF nursing care, but Family Health Conversations (FamHCs) involving the patient and the family, have not previously been tested. The purpose of the current study was to explore the experiences and feasibility of nurse-led FamHCs conducted by telephone with patients and their family caregivers. A single-group intervention study with a pretest–posttest design was conducted in three regional hospitals that had a nurse-led HF clinic. Five RNs, eight patients, and eight family caregivers participated. Three FamHCs were conducted by telephone with each family every 2 weeks. Qualitative and quantitative data were collected through semistructured interviews and questionnaires. FamHCs improved the nurse–family relationships and relationships within the families and provided RNs with new knowledge about the families. FamHCs conducted by telephone were considered to be feasible for both families and RNs, although RNs preferred fewer and shorter FamHCs. The RNs preferred meeting face-to-face with the families as nonverbal communication between the family members could be missed because of lack of visual input. On the other hand, RNs appreciated to focus entirely on the conversation without the need to perform illness-related routine checks. In conclusion, the advantages of FamHCs conducted by telephone outweighed the disadvantages. Visual contact, provided by video telephony, and a shorter version of the tested FamHC would facilitate the use in HF nursing care.
Keywords
Background
Heart Failure and Family Support
Heart failure (HF) is an increasingly prevalent chronic condition, affecting more than 26 million persons globally (Ambrosy et al., 2014) and is associated with high morbidity and mortality (Benjamin et al., 2017; Clark et al., 2014, 2016). Family support increases quality of life for both the patient and their family caregiver, improves self-care, and leads to fewer hospitalizations and reduced mortality (K. Årestedt, Saveman, Johansson, & Blomqvist, 2013; Buck et al., 2015; Stamp et al., 2016; Strömberg, 2013). Thus, family support is valuable for all parties, but its challenging consequences for family function and relationships within the family also need recognition (Dalteg, Benzein, Fridlund, & Malm, 2011; Gusdal, Josefsson, Thors Adolfsson, & Martin, 2016; Lum, Lo, Hooker, & Bekelman, 2014; Trivedi, Piette, Fihn, & Edelman, 2012). The challenging consequences include changes in family behavior and communication, together with relational incongruence in the family (Kitko, Hupcey, Pinto, & Palese, 2014; Retrum, Nowels, & Bekelman, 2013; Strömberg & Luttik, 2015). Furthermore, family caregivers express a need for involvement together with health-care professionals in the patient’s care, in order to reduce their own worry and uncertainty (Gusdal et al., 2016; Mårtensson, Dracup, & Fridlund, 2001).
Currently, most HF nursing interventions primarily focus on the patient to improve outpatient self-care (Lum et al., 2014), while guidelines for the management of HF recommend involving family members in education, in the provision of psychosocial support, and in the planning of care at discharge (Ponikowski et al., 2016; Yancy et al., 2013). Research also emphasizes the central role that registered nurses (RNs) have in providing psychosocial support and meeting the needs of the family members of a patient (Ågren, Evangelista, Hjelm, & Strömberg, 2012; Jaarsma & Strömberg, 2014). Dionne-Odom et al. (2017) recommend further targeting family communication skills and relational congruence. These recommendations are in line with those of other researchers (Hartmann, Bäzner, Wild, Eisler, & Herzog, 2010; Lum et al., 2014; Sebern & Woda, 2012) who emphasize that future HF nursing interventions should recognize the importance of family relationships and an improved understanding of family relationship quality.
Family Systems Nursing, Family-Centered Nursing, and Family Health Conversations
Educational and psychosocial support is important for both patients and family caregivers, and relational support has also been recommended in order to support and involve families (Evangelista, Strömberg, & Dionne-Odom, 2016; Strömberg & Luttik, 2015; Wingham et al., 2015). For the purpose of sustaining health and promoting healing in families living with a challenging chronic illness, the work of Wright and Leahey (2013) merits special attention. Concerned with the relationship between family dynamics and health, they developed Family Systems Nursing, with the specific goals of changing, improving, and maintaining family functioning (Bell & Wright, 2015; Wright & Leahey, 2013). A core assumption in Family Systems Nursing is that a change in one part of the system will inevitably bring a change in the other parts; thus, living with chronic illness is not solely an individual concern but also has a profound impact on family members. In Family Systems Nursing, each family member’s view is acknowledged as equally valid, even when single events, situations, or activities are perceived differently.
The practice models of the Illness Belief Model (Wright & Bell, 2009) and Calgary Family Assessment Model and Calgary Family Intervention Model (Wright & Leahey, 2013) were first developed and used in Canada within Family Systems Nursing. They have been adapted to the Swedish context and are offered through Family Health Conversations (FamHCs) within the Swedish family-centered nursing (Benzein, Hagberg, & Saveman, 2008, 2012; Saveman, 2010). FamHCs aim to create a context for change, to facilitate new beliefs, new ideas, and possibilities specific to the stories described by the family (Benzein et al., 2008, 2012). FamHCs primarily focus on the families’ internal strengths and external resources, which may be unrecognized because of the families’ illness beliefs and experiences. In this context, beliefs are understood as the experience of a subjective reality that influences a person’s thoughts, feelings, and behavior. Beliefs can be constraining or facilitating and are often not reflected upon. Illness beliefs are thought to either increase or reduce illness suffering (Wright & Bell, 2009).
Intervention studies in the area of Family Systems Nursing and the Swedish family-centered nursing have shown promising results (Östlund & Persson, 2014) such as positive outcomes for RNs’ job satisfaction, conceptual skills, strengthened nurse–family relationships (Dorell, Östlund, & Sundin, 2016; Duhamel, Dupuis, Reidy, & Nadon, 2007; Voltelen, Konradsen, & Østergaard, 2016), as well as cost-effectiveness (Lämås, Sundin, Jacobsson, Saveman, & Östlund, 2016). Family-centered nursing interventions can alleviate suffering and are psychologically empowering for the families (Benzein, Olin, & Persson, 2015; Dorell, Bäckström et al., 2016; Dorell, Isaksson, Östlund, & Sundin, 2017; Östlund, Bäckström, Saveman, Lindh, & Sundin, 2016; Sundin et al., 2016). In view of the central role families play in HF care and self-care to improve health outcomes (K. Årestedt et al., 2013; Strömberg, 2013), it is essential to prepare RNs for the challenges and opportunities of involving families and to provide appropriate support. To date, there are only few published studies, with various design and outcomes, of Family Systems Nursing and family-centered nursing interventions in HF nursing care (Duhamel & Talbot, 2004; Duhamel et al., 2007; Voltelen et al., 2016). Thus, the empirical research evidence from Family Systems Nursing and family-centered nursing interventions in HF nursing care needs to be strengthened if a relationship-focused family nursing approach is to be achieved in HF clinical practice.
Telephone Interventions
Telephone interventions have been found to be successful methods of intervention in HF nursing care (Chiang, Chen, Dai, & Ho, 2012; Inglis, Clark, Dierckx, Prieto-Merino, & Cleland, 2017; Piamjariyakul, Smith, Russell, Werkowitch, & Elyachar, 2013; Piamjariyakul et al., 2015; Piette, Striplin, Marinec, Chen, & Aikens, 2015). However, these interventions primarily concerned patients’ self-care, and not family relationships and illness beliefs.
Furthermore, the challenge today is to find an optimal cost-effective care model for the growing number of patients with HF. The “classic” HF clinic still has its place but with new components such as tele-monitoring or tele-education (Jaarsma & Strömberg, 2014). Given the complex and unpredictable nature of HF, which at times hinders patients from leaving their home, conversations conducted by telephone may be a suitable alternative to the face-to-face conversation. As FamHCs have not previously been tested as a telephone intervention in HF nursing care, the families’ and RNs’ experiences of FamHCs conducted by telephone will add considerably to the knowledge of family nursing interventions in HF nursing care. The purpose of this study was thus to explore the experiences and feasibility of nurse-led FamHCs conducted by telephone with patients and their family caregivers.
Methods
Design
Study Design—Single-Group Intervention Study With a Pretest–Posttest Design.

Note. FamHCs = Family Health Conversations.
aFive patients and five family caregivers participated in the joint interviews.
Study Setting and Participants
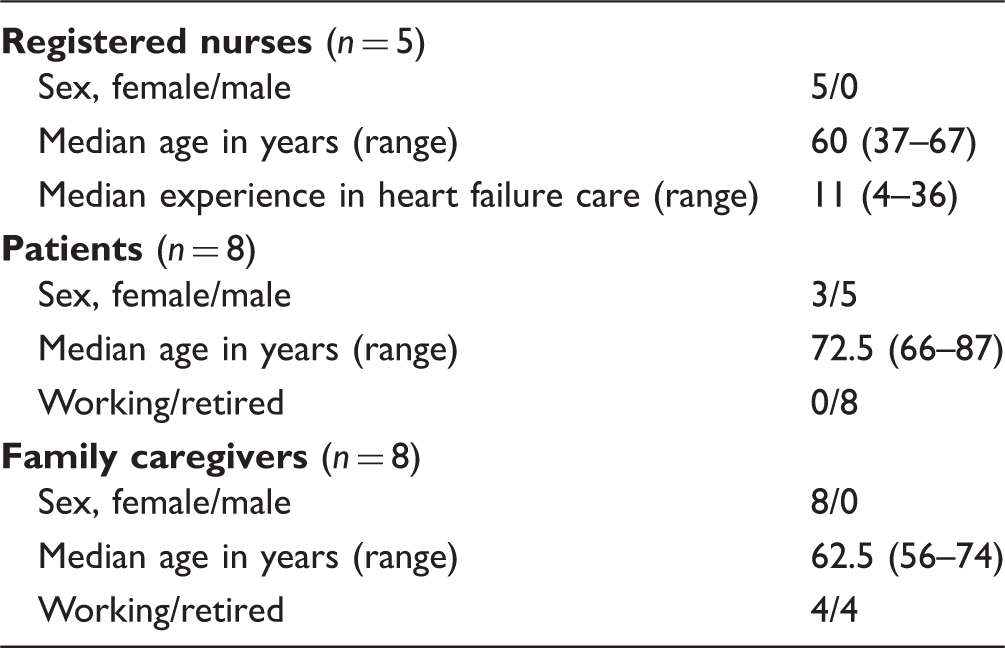
Demographic Data of the Participants.
Recruitment Procedure
In total, six RNs worked in the aforementioned clinics. They were all informed about the study background and purpose and asked to participate in the study, and five agreed. One RN was in the process of retirement and did not participate. During a period of 2 months, RNs consecutively informed the eligible patients about the study background and purpose before inviting them to participate. The goal was that each RN should recruit two patients and their family caregiver. Out of 30 invited patients, 22 declined participation. The reasons for declining were impaired hearing, considering the FamHCs and the study obligations to be too burdensome, or feeling too frail. Thus, eight patients and eight family caregivers participated after signing individual written informed consents. At the end of the last FamHC with each family, the RNs asked if the family was willing to take part in a joint interview with the first author about their experiences. Out of eight families, three declined. The reasons for declining were practical difficulties to meet face-to-face as the family caregivers lived far away. After receiving individual written informed consents, the first author contacted each family and organized the interview.
Intervention
The five RNs participated in a half-day intensive course held by the first author who was trained in conducting FamHCs. The course covered the theoretical underpinnings of family-centered nursing, the core components of the practice of FamHCs (Benzein et al., 2008, 2012; Östlund, Bäckström, Lindh, Sundin, & Saveman, 2015), and role-play in conducting FamHCs. The RNs conducted three FamHCs with each family, with an average duration of 45 minutes (range 30–60 minutes) for every 2 weeks using a telephone with speakerphone capability; in total 24 FamHCs.
The FamHCs’ focus was on the interplay and the relationships between family members rather than on the individual family members as it was assumed that “the problem” resides in the dialog between individuals rather than within the individuals. The family has the preferential right to decide what to talk about (Benzein et al., 2008, 2012) and the RN was a collaborator in an interactive process and acknowledges the family’s unique perspective. Differing perceptions can arise among family members, and the RN’s role was to embrace them all without partiality (Benzein et al., 2008, 2012; Östlund et al., 2015). The RN focused on the family’s strengths and invites narratives and reflections through asking reflective questions (Andersen, 2011; Benzein et al., 2008; Wright & Bell, 2009; Wright & Leahey, 2013). These questions focus on relationships and are “appropriately unusual,” that is, they open up new directions of thinking as they are slightly different from the family’s own beliefs and reflections (Andersen, 2011). During the FamHCs, the RNs’ silence was sometimes deliberately used to give time for reflection and allow for new thoughts and ideas to emerge and be voiced (Benzein et al., 2008, 2012).
The FamHCs in the present intervention differed from the conventional FamHCs in family-centered nursing, which are conducted by two RNs who meet face-to-face with the family and send a closing letter to the family 2 to 3 weeks later (Benzein et al., 2008, 2012).
To assess and ensure RNs’ adherence to the core components of FamHCs (Östlund et al., 2015), the first author listened to the first and last FamHC with each family. The families were informed about the first author’s presence in the room and the reason for it, and gave their verbal consent. Immediately after the first FamHC, the RN and the first author discussed the adherence to the core components of the FamHC. The RN was then provided with guidance in order to be appropriately prepared for the next FamHC with the same family.
RNs initiated the first FamHC by asking the family members about their expectations of the conversations. They were then invited to describe their beliefs about their current situation and were encouraged to listen to, and reflect upon each other’s narratives. The RNs listened carefully and tried to discern the essential parts of each narrative. Then, together with the family, the RNs decided the issues that were necessary to discuss. In the second FamHC, the RNs probed deeper into the family’s situation and the beliefs identified in the first FamHC. In the third and last FamHC, the focus was on the family’s thoughts about the future, and the RN and the family summarized and reflected on the eventual process of change that the family had undergone. At the end of each FamHC, the RNs offered their own reflections to the family, which confirmed the family’s narratives. The RNs also stated explicitly that the FamHCs were not focused on finding solutions but on the family’s ability to develop their own tools to improve their well-being. The problematic situation might persist after the FamHCs, but the family may have found new strategies to manage their situation.
Data Collection
Interviews
Interview Guide in Interviews With Families and RNs.

Note. Text in bold refer to the predefined categories, which correspond to the anticipated results of Family Health Conversations (FamHCs). RN = registered nurse.
Joint interviews were performed with five families, 4 to 6 weeks after their last FamHC. By definition, a joint interview is conducted by one researcher with two persons who have a prior relationship (Polak & Green, 2016) and presents a unique opportunity to support a dynamic communication between informants (Morgan, Ataie, Carder, & Hoffman, 2013). The interviews were performed in the families’ homes and lasted 45 to 70 minutes.
One individual and two joint interviews were performed with the five RNs, after completion of the FamHC series, in the RNs’ workplaces and lasted 20 to 30 minutes.
All interviews were performed, digitally recorded, and transcribed verbatim by the first author.
Questionnaires
Questionnaires were used to explore family caregivers’ experiences of caregiver burden, families’ experiences of RNs’ support, and of the communication within the family. Upon receiving individual written informed consent from the patients and the family caregivers, the first author posted the questionnaires to each person with a postage-paid return envelope included. The first author received the completed questionnaires 2 to 3 weeks before the first FamHC.
Heart Failure Caregiver Questionnaire®. Heart Failure Caregiver Questionnaire® (HF-CQ®) is a translated and reliability- and validity-tested questionnaire, which has the aim to assess the subjective caregiver burden of family caregivers to patients with HF (Strömberg et al., 2017). HF-CQ® consists of 21 questions, divided into three domains: Physical well-being (5 questions), Emotional well-being (11 questions), and Lifestyle (5 questions). Alternatives are rated on a 5-point Likert scale ranging from Not at all (1), to Very much (5). Higher scores reflect a higher subjective burden associated with caregiving. The total score for the entire scale is 105 points (Physical well-being, 25 points; Emotional well-being, 55 points; and Lifestyle, 25 points). The questionnaire was answered by family caregivers using a recall period of the past 4 weeks.
Iceland-Family Perceived Support Questionnaire (Swe). Iceland-Family Perceived Support Questionnaire (Swe) (ICE-FPSQ [Swe]) is a translated and reliability- and validity-tested questionnaire (Bruce et al., 2016) of the Icelandic ICE-FPSQ questionnaire (Sveinbjarnardottir, Svavarsdottir, & Hrafnkelsson, 2012), which has the aim to assess perceptions of cognitive and emotional support from RNs. ICE-FPSQ (Swe) consists of 14 items, divided into two subscales: Cognitive support (five items) and Emotional support (nine items). Alternatives are rated on a 5-point Likert scale ranging from Almost never (1) to Almost always (5). Higher scores reflect a perception of consistent family support offered by the RNs. The total score for the entire scale is 70 points (Cognitive support, 25 points; and Emotional support, 45 points). The questionnaire was answered by patients and family caregivers separately.
Statements Assessing Communication Within the Family.

Data Analyses
Because a model and theory existed prior to collecting data, a deductive approach (Elo & Kyngäs, 2008; Hsieh & Shannon, 2005) was used for the manifest qualitative content analysis. The intention was to explore the model of FamHC in a different context; conducted by telephone instead of face-to-face contact (Hsieh & Shannon, 2005). The data were searched for specific issues or categories related to the model and the theory. The coding framework consisted of predefined categories corresponding to the questions in the interview guide (see Table 3). First, the transcripts of the interviews were read through to get a sense of the text as a whole, and the sections with the families’ and RNs’ experiences of FamHCs were highlighted. The highlighted text was then coded and placed into the predefined categories of the coding framework. Data that could not be coded within the predefined categories were sorted into new categories (Hsieh & Shannon, 2005). Each step of the analysis was discussed by the authors until consensus was achieved. Quantitative data were analyzed with descriptive statistics using IBM SPSS Statistics, version 22.0 for Windows.
Ethical Considerations
The study was approved by the Regional Ethical Review Board in Uppsala [Dno. 2016/007] and conforms to the principles outlined in the Declaration of Helsinki (World Medical Association, 2013) and the International Committee of Medical Journal Editors (2017) Recommendations for the Protection of Research Participants. After the interviews, the families were assured that, if needed, a counselor would be available to support.
Results
Interviews
Families’ and RNs’ experiences of FamHCs described in the interviews are presented in accordance with the predefined categories and one new category.
FamHCs’ contribution to change in the families, and FamHCs’ impact on relationships and communication within the families (families’ experiences)
The reversed opening of the FamHCs, compared with “regular” conversations where the RNs decide what to talk about, was described by some of the families as unfamiliar and slightly uncomfortable. Yet, family members spoke about their worry for one another, and differences related to the knowledge and beliefs about HF symptoms and self-care surfaced, which would otherwise have remained hidden.
The FamHCs were experienced as an opportunity for the families to become more open with their thoughts and feelings, even after the FamHC series had ended. Family caregivers stated that the “permission” to talk about one’s own irritation and worry with a third person listening was a relieving and even liberating experience. Patients described that they felt affirmed and supported by the RN regarding their frequent need for rest because of HF symptoms. Likewise, family caregivers felt affirmed and supported by the RN about their need for the patients to discuss their symptoms more openly. Both parties were more explicit when describing their own thoughts and feelings and listened more patiently to each another than usual. After the FamHCs, they found it easier to complement each other’s narratives, and to discuss new issues that they had hesitated to bring up before.
FamHCs offered opportunities for the family caregivers to establish a contact with an RN in the nurse-led HF clinic. For the family members, this highlighted the need to have an RN as a permanent health-care contact; a need not all had reflected upon prior to the FamHCs.
FamHCs’ contribution to change in RNs’ work, and FamHCs’ impact on RNs’ relationships and communication with the families (RNs’ experiences)
When the agenda for the FamHCs was decided upon by the family members, it became evident for the RNs that the families needed to speak about issues beyond self-care and monitoring of symptoms. Some RNs found it slightly awkward to speak openly about relational matters with the families.
The RNs also initially struggled with the reflective “appropriately unusual” questions. Eventually, the RNs found them to be useful as they led to a more straightforward and truthful conversation, and presented a more complete picture of the family situation. The RNs intended to continue to use the reflective questions in their daily work.
The RNs described how their previous awkwardness with silence had subsided. Silence was found to be a powerful tool to give time for new thoughts and ideas to emerge, and RNs intended to continue using silence in future contacts with patients and family caregivers. I have worked with myself when it comes to silence, to dare to be silent, it’s really powerful, and it’s a strength to be able to stay silent. There is so much coming from that, from the family, when I give them more space to reflect on what has been said and I kind of invite them through silence to tell their story. I have really practiced that in these conversations. (RN)
New knowledge and understanding gained through FamHCs (families’ and RNs’ experiences)
The FamHCs led to better understanding of the necessity to be open and discuss differences in the knowledge and beliefs about HF symptoms. Before FamHCs, the patients could trivialize, or camouflage, symptoms while the family caregivers observed the deterioration but were unable to discuss this with the patient. I come from one of those families where you would never complain and “Ah, it will sort itself out, if not today then tomorrow” so why go to the doctor and why keep moaning about it. So, therefore I get a bit quiet sometimes. (Patient in a spousal relationship)
Generally, the family members did not want to worry each other by talking about their own worries about the consequences of HF, which had resulted in silence in the relationship. However, the family caregivers found it valuable to speak and reflect on their worries in the presence of an RN who specialized in HF nursing care, as the professional presence temporarily unburdened them of their medical responsibility. After the FamHCs, family caregivers were conscious of their own potential negative patterns of worry and tried to break them.
It was sometimes challenging for the RNs to retain a collaborative, nonhierarchical relationship between themselves and the families. Most challenging was to grant equal value to all family members’ views about self-care when these were in sharp contrast to the RNs’ medical knowledge or when the patient was considered to be in denial. However, the RNs still adhered to the FamHC model’s core components and acknowledged its benefits, despite the RNs’ challenged professional opinions.
Freedom of choice about when to conduct FamHCs (families’ and RNs’ experiences)
An additional category emerged, beyond the predetermined categories. Both families and RNs discussed the importance of having the freedom to choose when to conduct FamHCs. Families stated that there was no need for FamHCs when the health status of the patient was relatively stable, and tranquility in the relationship was enjoyed. FamHCs were instead more useful and supportive after an exacerbation or deterioration of HF. Families also suggested that RNs’ routine checkups conducted by telephone could be in the form of FamHCs. Families and RNs were unanimous in stating that FamHCs should be offered to families soon after HF diagnosis to detect relational incongruence early, and as a suitable complement to RNs’ routine follow-up in education on HF and self-care.
Feasibility of FamHCs conducted by telephone (families’ and RNs’ experiences)
An overall satisfaction with FamHCs conducted by telephone was found. For families, the positive aspects included the comfort of remaining in one’s home and the possibility for family caregivers who lived far away, or who were short of time or working, to participate in FamHCs. The negative aspects were mostly of a technical nature and included occasional telephone line disturbances. Families also experienced a certain tension when there was a prolonged silence and mistook it for a disconnected telephone line. Thus, the relaxed atmosphere and recurring silence, characteristics of FamHCs, were somewhat compromised when conducted by telephone. Also, the advantages of having face-to-face conversations such as verbal nuances, facial expressions, and body language were lost in FamHCs conducted by telephone. In the event of strong emotional reactions in the conversations, the appropriateness of conducting them by telephone was questioned by both families and RNs. Nevertheless, FamHCs conducted by telephone were experienced by families as “good enough,” with the improved opportunities to involve family caregivers and establish nurse–family relationships as their main advantages.
The RNs preferred meeting face-to-face with the families. Over the telephone, important nonverbal communication between the patient and the family caregivers could be missed, which could lead RNs to misinterpret the situation and relations within the family. Also, the inability of RNs to see bodily reactions and to look into the eyes of the family members created insecurity for the RNs. Therefore, it was important for the RNs to have an established relationship with the family caregivers prior to the FamHCs. On the other hand, when RNs felt secure, they spoke about sensitive issues with ease as the distance created by telephone had a buffering influence. Moreover, when using the telephone, the focus was entirely on the conversation, without the disturbance from visual inputs or illness-related routine checks.
RNs considered three FamHCs to be one too many. As core issues had already been discussed in the first and second FamHCs, the third FamHC was experienced as repetitive. The stipulated minimum time of 30 minutes per FamHC was a reasonable time to allow for more in-depth conversation, except in the third FamHC when it was considered as too long. The feasibility of conducting FamHCs in RNs’ daily work was questioned because of the length and number of FamHCs. Nevertheless, the RNs saw several advantages of FamHCs conducted by telephone. They enabled RNs to make contact with family caregivers who ordinarily did not have the opportunity to come in person, and with families in which the patient or the family caregiver were too weak or ill to come to the nurse-led HF clinic.
Questionnaires
Family caregivers’ experiences of caregiver burden
Family caregivers’ (n = 8) experiences of caregiver burden.
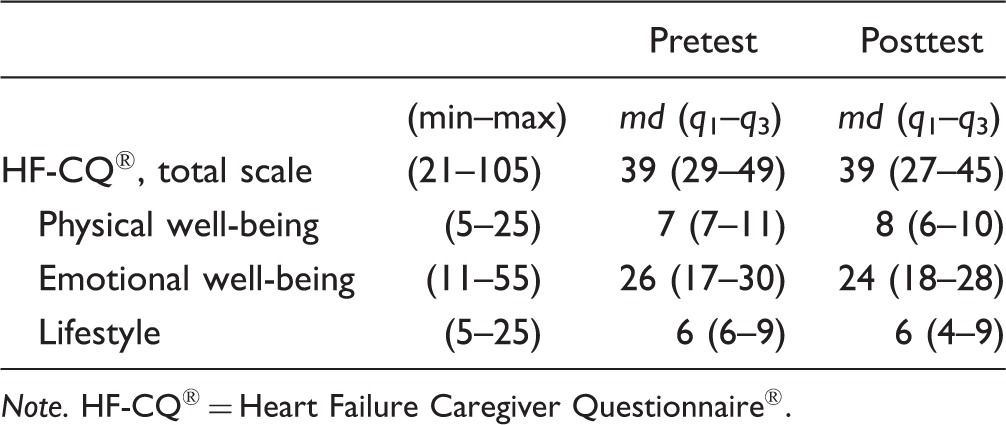
Note. HF-CQ® = Heart Failure Caregiver Questionnaire®.
Families’ experiences of RNs’ support and of communication within the family
Families’ Experiences of Registered Nurses’ Support.

Note. ICE-FPSQ (Swe) = Iceland-Family Perceived Support Questionnaire (Swe).
Families’ Experiences of Communication Within the Family.

Discussion
Overall, participation in FamHCs was described as facilitating communication within the family and initiated and strengthened the nurse–family relationships. FamHCs conducted by telephone were also considered to be feasible, but needed modification in length and number in order to better suit RNs’ daily work.
Families’ and RNs’ experiences of FamHCs
Worry and relational incongruence were key issues discussed in the FamHCs and family caregivers reported reduced worry after they had participated in the FamHCs. The persistent worry and uncertainty that are recurring themes in the literature on HF and family caregiving (Dionne-Odom et al., 2017; Gusdal et al., 2016; Hooker, Grigsby, Riegel, & Bekelman, 2015), seemed to be mitigated by FamHCs in the current study.
To narrate one’s own story in the FamHCs was also an opportunity for the families to become aware of their own beliefs and gain a new understanding of themselves as individuals and as a family. This can be compared with a study by Bülow (2004) who found that through sharing narratives, the participants jointly created experiential knowledge. In the current study, the family caregivers reflected, through narration, on their need to constrain their worry in order to limit HF’s influence on their daily life. This new understanding was related to listening to their own stories, as observed by Benzein and Saveman (2008) who discussed how individuals construct stories while narrating them, using their reflections.
Although the responses in the questionnaires are based on few respondents, the posttest responses showed a tendency for families, in particular the patients, to experience increased support from RNs. Presumably this was because of the trusting environment that FamHCs provided, as previously found by Dorell, Bäckström, et al. (2016) and Sundin et al. (2016). For some family caregivers, it was the first time they had been included in a conversation with the RN in the HF clinic and given the chance to talk about their caregiving situation. The families also said that they after the FamHCs more easily complemented each other’s narratives and discussed new issues that they had previously been hesitant to bring up, which was also found by Persson and Benzein (2014). The new awareness of one’s burden and the need for an RN as a permanent health-care contact were described in the joint interviews and are in line with previous results that suggest that FamHCs is a way for families to unburden “a load they were not aware of carrying” (Benzein and Saveman, 2008, p. 442).
Families living with a chronic illness can create the unhelpful belief of illness as a threat to life as opposed to “illness as a part of life” (Walsh, 2016). If the family primarily lives within the present moment, even while experiencing a serious illness, and accepts “what is now” rather than focusing on the past or future, the suffering is likely to decrease (Wright, 2015). Using the Illness Belief Model in FamHCs is one way to ease the family’s suffering since it acknowledges and strengthens the family’s facilitating illness beliefs, and explores and challenges the family’s constraining beliefs (L. Årestedt, Benzein, & Persson, 2015; Östlund et al., 2016). The findings in the current study suggest that FamHCs conducted by telephone, can support a shift in illness beliefs as the families became aware of some of their constraining beliefs and spoke openly about them.
It is not only families that hold facilitating or constraining beliefs about illness and health, so do health-care professionals (Bell, 2013). In the FamHCs, RNs became aware of their own constraining beliefs about granting equal value to all family members’ narratives and beliefs, as some of these challenged the RNs’ medical knowledge. Instead of correcting family members’ misconceptions about self-care or monitoring of symptoms, the RNs tried to develop an atmosphere of trust with the families by exploring their experiences and beliefs without interrupting, questioning, or judging them. Bell (2013) describes how the relationships between families and RNs are shaped by the beliefs of the RNs. If they believe that they have more education and expertise (and thus are likely to be more “right”) they may be less inclined to value the families’ views or enter into collaborative relationships with them. To hold the belief that “I have no time to involve families” constrains the relationships and conversations with families. If RNs instead believe “I have confidence in my knowledge and skills about how to talk to families,” they will become more confident in welcoming, including, and acknowledging families as partners (Bell, 2013).
Families’ and RNs’ Experiences of the Feasibility of FamHCs Conducted by Telephone
FamHCs conducted by telephone was an attempt to bypass families’ difficulties in leaving their homes, a dilemma characteristic of patients with HF. Previous support and coaching programs for family caregivers conducted by telephone have shown positive effects (Piamjariyakul et al., 2013, 2015; Piette et al., 2015); however, these interventions primarily concerned self-care, and not beliefs and family relationships. Outcomes of a relationship-focused intervention, as conducted in the current study, can be expected to depend upon health-care professionals meeting families face-to-face. Therefore, it is encouraging that Chiang et al. (2012) found a significant improvement of family functioning after a relationship-focused tele-health-care intervention. In the current study, the advantages of FamHCs conducted by telephone seemed to outweigh the disadvantages for both families and RNs. To avoid misinterpreting the situation because of being unable to see each other, video telephony can be used, or other online devices as shown in a study by Lindh et al. (2013).
Feasibility of FamHCs Conducted by Telephone in HF Nursing Care
It is important to identify the prerequisites for successfully introducing and sustaining family nursing interventions in the clinical setting. Interventions may be successful while the studies are ongoing, but the needs and demands of RNs and their workplaces have to be considered in order to integrate family nursing interventions that are feasible for RNs on a long-term basis. In the current study, RNs preferred to conduct fewer and shorter FamHCs: two FamHCs with a maximum length of 30 minutes. Bell (2012) highlights the 15-Minute Family Interview as an attractive and feasible practice model in the clinical setting. Four hours of teaching sessions and training sufficed to adequately prepare RNs for integrating the 15-Minute Family Interview into their daily clinical practice (Braun & Foster, 2011; Martinez, D’Artois, & Rennick, 2007; Svavarsdottir, 2008; Svavarsdottir, Tryggvadottir, & Sigurdardottir, 2012). Leahey and Wright (2016) state that the majority of young and inexperienced RNs feel insecure about meeting with families and will mask their apprehensions by stating shortage of time in their everyday practice. However, once RNs embrace the belief that “illness is a family affair” (Wright & Bell, 2009) and understand that they can make a profound difference in only 15 minutes or less, they challenge their constraining belief of not having enough time.
The difficulties of implementing family nursing interventions have previously been described as multifactorial on both organizational and individual levels. Challenges on an organizational level include poor managerial support and whether health-care personnel adopt a shared approach toward families in their workplace (Duhamel, 2010; Duhamel, Dupuis, Turcotte, Martinez, & Goudreau, 2015; Saveman, 2010; Voltelen et al., 2016; Wright & Leahey, 2013). The major challenges on an individual level are the absence of role models and lack of coaching in family nursing in the workplace, together with RNs’ low level of confidence in their competence to work with families. Challenges also include RNs’ young age, gender, short nursing experience, level of education, and their attitudes toward family involvement (Bell, 2013; Benzein et al., 2008; Duhamel et al., 2007; Gusdal, Josefsson, Thors Adolfsson, & Martin, 2017; Saveman, 2010; Voltelen et al., 2016; Wright & Bell, 2009; Wright & Leahey, 2013). Gusdal et al. (2017) found that to work in primary health-care centers or in nurse-led HF clinics, and to have a district nurse specialization or education in cardiac or HF nursing care predicted RNs’ most supportive attitudes toward family involvement in HF nursing care. These RNs can act as role models and mentors for their younger and less experienced colleagues.
It should be noted that disagreement exists in the literature on whether family nursing should be limited to RNs with specialist education (Braun & Foster, 2011). Duhamel et al. (2007) and Voltelen et al. (2016) underscore in their studies that in addition to being an experienced RN who feels secure in their own professional capacity, it is important for RNs to acquire expert knowledge in HF nursing care and nursing skills in family nursing in order to work successfully with families.
Limitations and Strengths
There are several limitations in the study. Out of 30 families, 22 declined to participate. Three reasons were given for nonparticipation: considering the FamHCs and the study obligation of questionnaires to be too burdensome, feeling too frail, and having hearing problems. Thus, the study may have excluded the families most in need of support. Because of the small sample, the quantitative data can only point toward tendencies and, therefore, no inferential statistics were used. Another limitation is the choice of technology. Video telephony is currently available and video conversation is a standard procedure in many contexts. Thus, missing nonverbal communication between the family members because of lack of visual input can easily be resolved by modern technology.
However, this study is the first of its kind and even though the results might not be transferable, it can inspire others in the field of family nursing or HF nursing care to conduct similar interventions by the use of video telephony, using the reliability- and validity-tested questionnaires HF-CQ® and ICE-FPSQ (Swe).
Conclusions
Families and RNs experienced that FamHCs conducted by telephone facilitated the communication within the family, and initiated and strengthened the nurse–family relationships. The FamHC can thus be a way for RNs to support and involve families in HF nursing care. FamHCs conducted by telephone were found to be feasible for both families and RNs, although fewer and shorter FamHCs were preferred by RNs. The advantages seemed to outweigh the disadvantages for both families and RNs, but to avoid misinterpretation caused by lack of visual contact was requested, the use of video telephony may be a better alternative. Also, a shorter version of the tested FamHC could be implemented in all encounters with families struggling with HF, whether they take place in a nurse-led HF clinic, a hospital ward, in a regular follow-up in the primary health-care center, in home health care, or in a routine follow-up conducted by telephone.
Footnotes
Acknowledgments
The authors wish to express their sincere gratitude to all the patients, family caregivers and RNs who shared their time, experiences and thoughts so generously with them.
Declaration of Conflicting Interests
The author(s) declared no potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.