
Abstract
Employee turnover is a key metric and performance indicator when evaluating the fiscal and operational effectiveness of any health-care facility. This article outlines a turnover analysis and onboarding program performance improvement initiative used by a 187-bed community hospital in the Washington DC metropolitan area to reduce staff turnover. Using an evidence-based approach, we evaluated facility staffing statistics, exit survey data, research literature, and industry exemplars. We identified presence of severe turnover for hospital and nursing staff employed less than one year (new hires), with 2009–2012 annual new-hire losses ranging from 28.8% to 49.6%. Exit survey data identified only 50% to 62% of new employees who felt that: hospital orientation provided necessary information for successful employment; they had people to go to with concerns; and they had a realistic understanding of their job. Therefore, a 10-element program intervention was designed to strengthen and standardize the new employee onboarding process. Program elements focused heavily on retooled onboarding communications, including frequent new-hire interactions with managers and regular support from assigned high-performing colleagues. Post program implementation, overall annual hospital turnover decreased from 18.2% to 11.9% and new-hire turnover losses decreased from 39.1% to 18.4.%, which was statistically significant between measurement periods (Wilcoxon signed ranks test, Z = −2.06, p = .04). Implementing a standardized onboarding format that was specifically tailored to support new-hire employees allowed our hospital to rapidly reverse unsustainable turnover increases. The successful reduction in hospital and nurse turnover we achieved was rooted in multidisciplinary engagement of institutional stakeholders, managerial collaboration across departments, and strong support from executive hospital leadership.
Keywords
Introduction
Employee retention is one of the primary measures to determine the overall and fiscal health of an organization (Griffeth & Hom, 2001). Workplace dynamics that drive employee turnover, or voluntary employment termination, are often modifiable (Kovner, Brewer, Fatehi, & Jun, 2014). Hospital employers that fail to assess severity of their employee turnover are neglecting a key organizational resource impacting their financial interests, nursing care processes, patient outcomes, and the overall perception of a positive healing environment for patients (Collini, Guidroz, & Perez, 2015; Hayes et al., 2012). For example, hospital staffing turnover is estimated to account for up to 5% to 5.8% of total hospital annual operating budget and is largely driven by the loss and necessary replacement of qualified nurses (Waldman, Arora, & Smith, 2004).
Comprehensive turnover costs are challenging for health-care organizations to calculate. This is due to changing external market forces and regulatory controls, the inability to directly link revenues to staffing costs, and the variability in how institutional turnover is defined as an operational construct (Waldman et al., 2004). As such, cost estimates cited for hospital nursing turnover range considerably—from $10,098 to $88,000—and are due to variability in the research methodology used to obtain them, largely during cost categorization and conceptualization processes (Li & Jones, 2013). The Li and Jones (2013) estimate is based on a 20-year literature review (1990–2010) comprising 10 seminal studies, with turnover measures varying greatly across research efforts as to how investigators defined and calculated institutional turnover. For example, some facility metrics included nursing assistants and licensed practical nursing staff in addition to registered nurses (RNs), others included just full-time nurses, others incorporated all staffing categories (i.e., full-time, part-time plus others), while still others defined turnover as voluntary only, or both voluntary and involuntary.
Variable measure calculation and research methodology design appears to be typical in health-care turnover research. For example, the 2009 Retaining Experienced Nurses Research Initiative sponsored by the Robert Wood Johnson Foundation reported that RN replacement costs for 13 grantee hospitals ranged from $14,225 to $60,102, with the average cost of replacing a full-time equivalent RN being $36,657 (Lewin Group, Inc., 2009). In contrast, a Consumer Price Index cost assessment technique obtained an average cost of replacing an experienced RN at $62,000 to $67,000, with a correlated total nurse turnover cost of $5.9 to $6.4 million, and after inflation adjustment, these values rose higher—to $82,000 to $88,000 and $7.9 to 8.5 million (Jones, 2008). Regardless of the variability in turnover calculation technique employed by facilities and investigators, cumulative research findings indicate that hospital nurse turnover can be costly for organizations to ignore.
The priority designated to reduction of staff turnover by hospital executives, and in particular nursing turnover, is not always as high as it could be. Competing demands, expanding professional responsibilities, a rapidly changing health-care policy landscape, and the reality that some degree of turnover is ever-present, means nurse turnover can become a lower level priority in administrative settings. For example, a national survey of 240 U.S. hospital executives prioritized nursing and physician workforce issues behind government reimbursement, clinical quality, government regulations, commercial reimbursement, and uncompensated care (Pricewaterhouse Coopers’ Health Research Institute, 2007). Often high nursing turnover is not detected until it is a severe problem, at which point it is challenging for organizations to ameliorate.
Published reports indicate creating a supportive work environment, especially between managers and employees, creates a strong deterrent to nurses leaving an organization by improving perception of organizational support, employee engagement, team cohesion, and connection to the mission of the health-care setting (Cline, Reilly, & Moore, 2003; Collini et al., 2015; Homburg, Van Der Heijden, & Valkenburg, 2013; Nei, Anderson Snyder, & Littwiller, 2015; O’Brien-Pallas, Duffield, & Hayes, 2006; Ritter, 2011; Tomey, 2009). Skilled managers with executive support can deliver the right work environment and nurture worker relations; however, numerous variables must be adequately addressed including: staffing, job satisfaction, nurse attitudes such as intent to stay, competitive compensation and benefits, professional autonomy, advancement opportunities, positive physician relationships, and presence of social support, among others (Aiken, Clarke, Sloane, Lake, & Cheney, 2008; Aiken, Clarke, Sloane, Schalski, & Silber, 2002; Brewer, Kovner, Greene, Tukov-Shuser, & Djukic, 2012; Buffington, Zwink, Fink, Devine, & Sanders, 2012; Larrabee et al., 2003; Unruh & Zhang, 2014). Determining and quantifying factors responsible for increased turnover can help hospitals to create a positive work environment and impact hospital and nurse staffing, and patient and financial measures at various levels of the organization.
A critical component to retaining qualified staff is ensuring that new employees are successfully assimilated into an organization’s culture at the time of hire (Trossman, 2016). A 2007 study by the Wyndhurst Group (as cited in Maurer, 2015) reported that new-hire employees were 58% more likely to remain employed at 3 years’ post-hire if they participated in a structured onboarding process (Maurer, 2015). When newly hires are placed into intense acute care practice environments without a structured orientation process, employees can become quickly discouraged and disconnected from their work and colleagues (Goldschmidt, Rust, Torowicz, & Kolb, 2011). Organizations that can acculture new employees to required professional skills and expected normative group behaviors can create a robust competitive advantage by retaining highly qualified individuals over long-term employment periods (Baldwin, 2016). New nurses are particularly susceptible to rapid turnover losses if not professionally and socially sustained through a structured format of employer support, commonly in the form of nurse residency programs (Bontrager, Hart, & Mareno, 2016; Bratt & Felzer, 2011).
Our medium-sized (187-bed), hospital network-affiliated, community hospital in the DC metropolitan area is engaged in transforming its clinical and nursing practice environment. In December 2012, following several years of significant hospital staff turnover, nurse leaders and executive personnel identified a total hospital staff voluntary turnover rate of 18.2%, nursing staff voluntary turnover of rate of 12.5%, and a nurse vacancy rate of 7.4%. In comparison, 2012 national benchmarks were 14.3% for median hospital turnover, 13.2% for median nursing turnover, and a median bedside staff nurse vacancy rate of 4.4% (The Advisory Board Company, 2012). Using our corporate “Cost of Turnover Analysis” instrument, we estimated financial losses from hospital and nursing staff turnover at $12,350 per termination (total of n = 157), yielding a total financial loss of $1,938,950 to our facility for Fiscal Year 2012. We identified a concerning trend of increasingly severe new-hire turnover losses of 29.8% to 47.5% (staff employed less than one year) with corresponding exit survey data from the same periods indicating outgoing staff did not feel informed or supported at the time of hire. This article summarizes the evidence-based performance improvement process we used to reverse escalating levels of hospital and nurse staff turnover, and the notable outcomes achieved after implementation of a 10-element onboarding program intervention.
Methods
Following consultation with hospital and nursing staff leaders in January 2013, a Human Resources Committee (HRC) was charged with reversing a trend of escalating severity in hospital and nursing staff turnover. As this was an internal performance improvement initiative based on administrative process data and no human subject risks were present beyond institutional standard of care, institutional review board approval was not obtained. We used an evidenced-based turnover analysis approach that included: (a) compilation and analysis of 2009–2012 facility staffing and turnover statistics, (b) analysis of standardized exit survey data, (c) literature review, and (d) review of industry practice exemplars in health-care and private sectors.
Turnover Terms and Definitions.

The 10-Element Onboarding Program for Hospital and Nursing Staff Turnover Reduction.

We aimed to reduce the total turnover below 14% and the new-hire turnover below 20% by December 2013. The HRC created a proposal for the initiative and the Vice President Human Resources (VPHR) presented it to our hospital’s executive leadership (Chief Executive Officer [CEO], Chief Operating Officer, Chief Financial Officer, and Chief Nursing Officer), who endorsed the adoption of the onboarding program facility-wide. Following additional hospital stakeholder approvals from department directors and staff, our 10-element turnover reduction intervention was initiated in April 2013.
30-, 60-, and 90-Day Structured Interview Content.

Pre- and postintervention staffing and turnover data were imported into IBM SPSS Statistics version 20 and analyzed for statistical significance using the nonparametric Wilcoxon signed ranks test (Wilcoxon matched pairs signed ranks test).
Results
Annual Turnover and Demographic Data for Hospital and Nursing Staff.
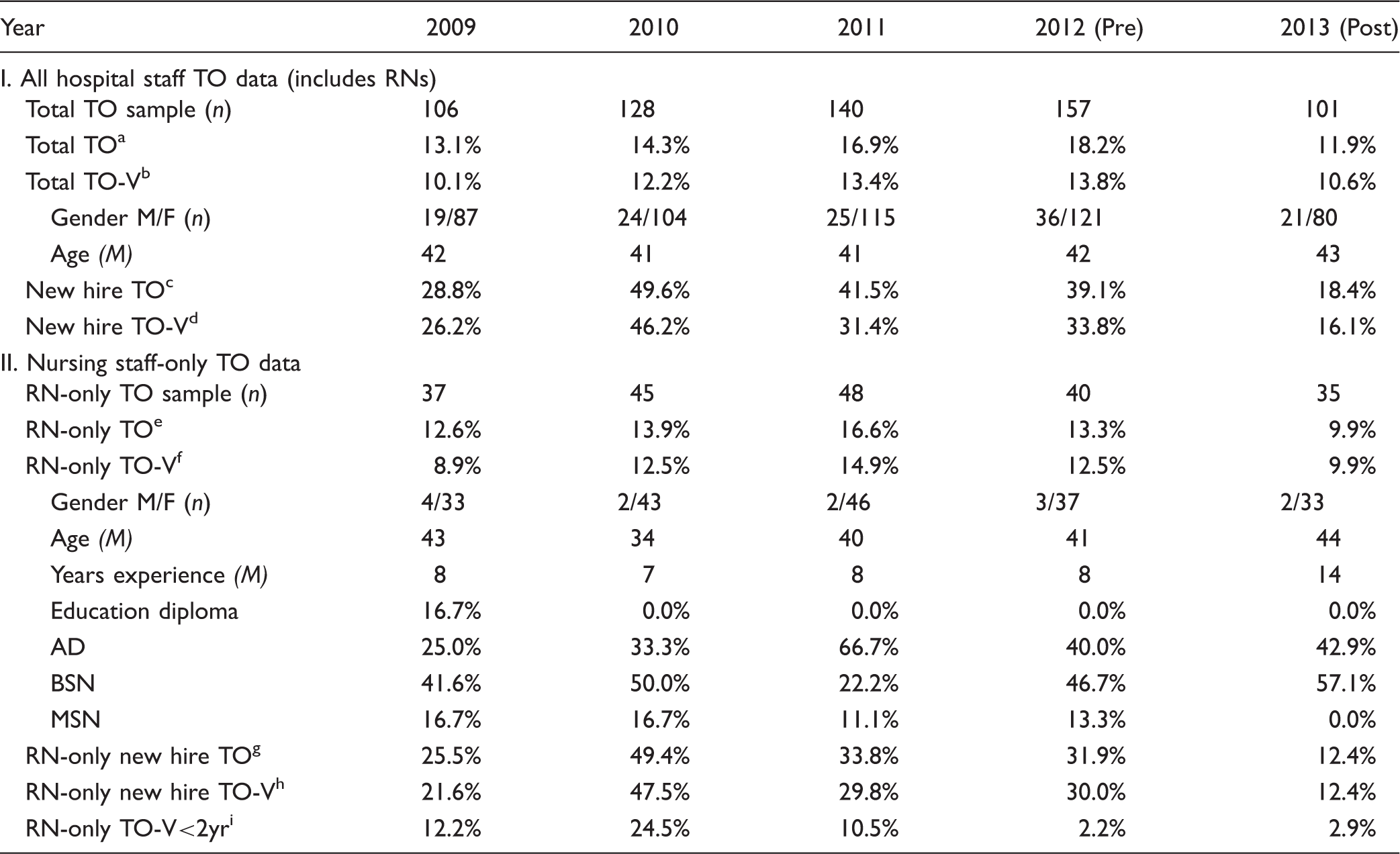
Note. Preintervention annual turnover data are summarized for 2009–2012 and postintervention data in 2013. The denominator for all Table 1’s percentage data are the total TO sample n.
Total TO: total involuntary and voluntary turnover.
Total TO-V: total voluntary turnover.
New Hire TO: % of total involuntary and voluntary turnover comprised of individuals employed <12 months.
New Hire TO-V: % of total voluntary turnover comprised of individuals employed <12 months.
RN-Only TO: total nursing involuntary and nursing voluntary turnover.
RN-Only TO-V: total nursing voluntary turnover.
RN-Only New Hire TO: % of total involuntary and voluntary turnover for RNs employed <12 months.
RN-Only New Hire TO-V: % of total voluntary turnover for RNs employed <12 months.
RN-Only TO-V <2yr: % of total voluntary turnover for RNs with <2 years’ experience.
Demographic trends for outgoing hospital and nursing staff from 2009 to 2013 appeared relatively stable and did not contribute to the intervention program design process. The average age of departing staff ranged from 41 to 43 years for hospital staff and 34 to 44 years for nursing staff, and was predominantly female across all categories. Outgoing nursing staff were primarily baccalaureate prepared and had an average of 7 to 14 years of clinical experience. Similar to the overall trend of increased new-hire hospital staff turnover, there was increased new-hire loss of RNs, which ranged between 29.8% and 47.5% in 2010–2012. RNs with less than 2 years of clinical experience comprised a small amount of nurse turnover for most years (2.2%–12.2%), except in 2010 (24.5%).
Figure 1 presents 2012 data on five key measures from standardized exit surveys collected by a third-party vendor. Results confirmed need for administrative retooling of our hospital orientation and onboarding programs, and provided additional insight to why our new-hire losses were occurring. Three of the five measures received special focus: only 50% of departing employees agreed that orientation provided information key to successful employment; only 57% agreed they had someone to go to for questions and concerns; and just over half (62%) agreed they had a realistic understanding of the job prior to their employment.
2012 Selected Onboarding Exit Survey Elements.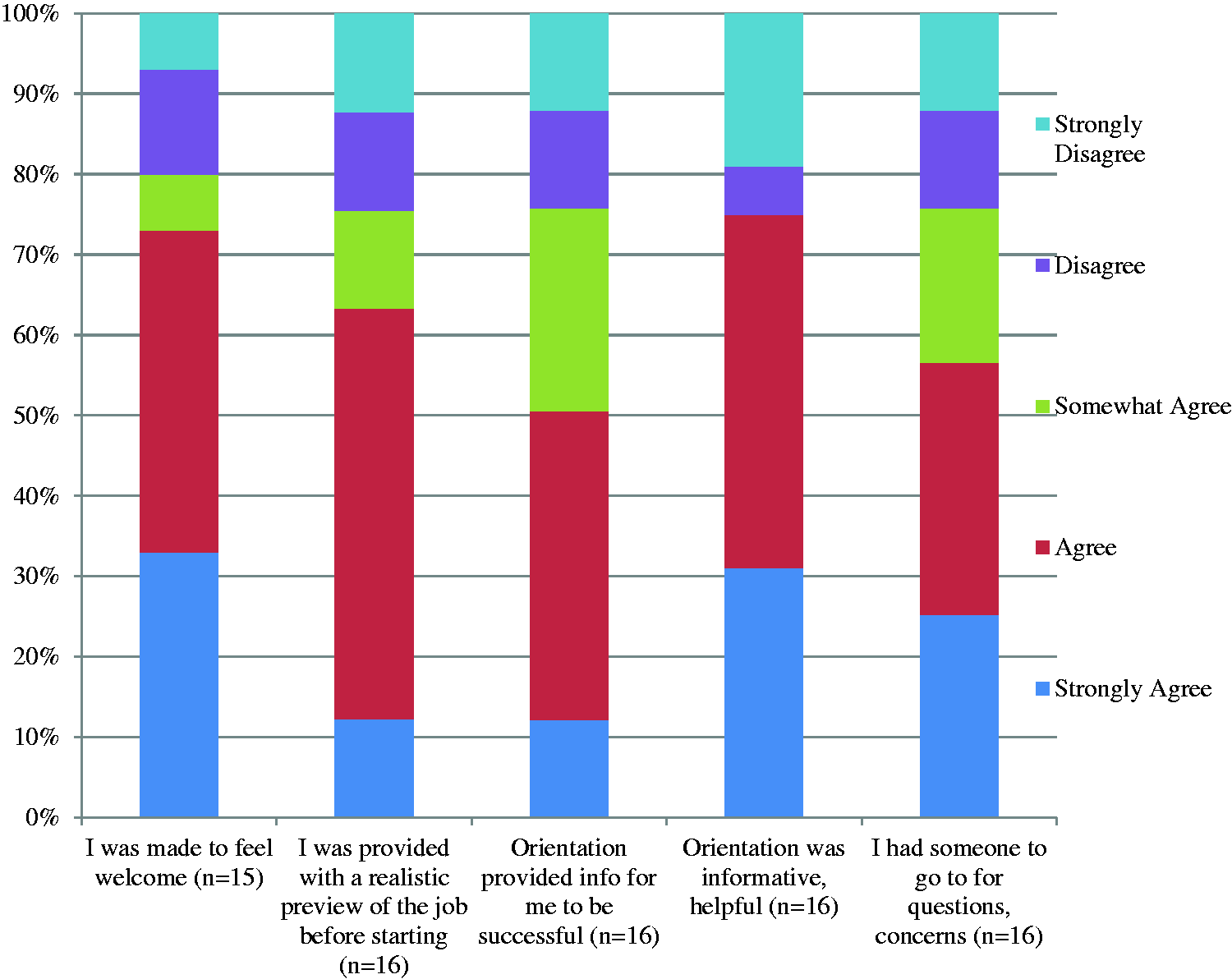
Participants who completed the program felt regularly scheduled interviews created a structured process to get to know their managers. Additionally, the seriousness with which their managers sought and recorded their feedback, and reported it to administrative leadership, allowed new-hire employees to feel they meaningfully contributed to the onboarding process and hospital’s practices. Participants felt managers really cared about what they thought and were seriously considering their input on how to improve things in their department. The use of specific interview questions ensured managers demonstrated caring concern during the 30-, 60-, and 90-day interviews when asking new-hire employees for their input. Managerial follow-through when acting on that input led to the overall perception of a highly individualized and supportive approach. All documented 30-, 60-, and 90-day information by the manager was turned into the Human Resources department, who created a database and monitored new-hire responses for problems and trends.
Hospital and Nursing Department Pre- and Post-Intervention New-Hire Turnover.

Note. Hospital and nursing department new hire turnover (FT, PT employees employed <12mths) before and after implementation of a 10-element pilot program; 0% change data not shown (n = 37). Telemetry, MRI, and Plant department staff are small (between 1 and 3 staff), producing > 100% TO changes and indicated by (–).
Discussion
We identified unusually high new-hire turnover, need for a new onboarding program to better support our new-hire employees, and also need for improved collaboration with hospital/unit directors and supervisors to improve the new-hire experience. We created and implemented a 10-element program intervention focusing heavily on the support of new-hire employees to reduce annual hospital and RN staff turnover. We achieved a statistically significant reduction in staff departures and met our stated goals of total turnover < 14% and new-hire turnover < 20% by December 2013.
While some degree of employee turnover is expected and healthy, increased turnover rates in a hospital environment can threaten the core primary function of providing safe, quality-driven patient care (Nowak, Holmes, & Murrow, 2010). There is strong consensus that turnover damages overall fiscal health and is often driven by the loss of qualified nursing staff (Kovner, Brewer, Greene, & Fairchild, 2009). While turnover was a problem at our facility, we found that it was primarily driven by new-hire losses and included both hospital staff and RN terminations. Replacement of qualified nurses is especially costly, and this was a category for which we experienced significant loss. Its impact is likely underestimated by our corporate calculation of $12,350 per termination. For example—replacement of qualified RNs is cited at $48,000 for a medical-surgical nurse, $64,000 for a critical care nurse, and can even extend up to 125% of the nurse’s annual salary (Beecroft, Kunzman, & Krozek, 2001; Cline et al., 2003). These amounts are associated with the direct costs of supplanting staff (i.e., human resources department time and resources, hospital manager time, accrued paid time off, and temporary coverage costs) and the indirect costs of orienting new staff (i.e., mentoring time, productivity decreases, morale decreases, training equipment, and materials). Additionally, new-hire losses are especially serious and produce a greater effect than losing tenured employees. New-hire losses result in exponential increases in per capita hiring, produce intense workloads for remaining staff that are constantly onboarding new hires, and can drive departures and early retirements of tenured staff (The Advisory Board Company, 2015). Frequent orientation of new staff, working with staff that may not be as skilled, working short when staff replacements are not found collectively impact morale, attendance, patient and staff satisfaction, and further affects the hospital’s bottom line.
During our turnover analysis, exit survey response data were used to assist in the design of the turnover reduction program initiative. While there is little scientific evidence from empiric research concerning their effectiveness, numerous reports affirm exit interview utility in gaining detailed work setting information to assist managers and executives in the design of turnover reduction initiatives (Brooks, 2007; Hawkins, O’Connor, & Potter, 2003; Leahey & Henderson, 1991; Flint & Webster, 2014; Whitis & Whitis, 1983). A primary criticism of exit interviews or surveys is decreased validity when departing employees do not want to share negative information about their reasons for leaving (i.e., negative feedback about a manager). Use of neutral, trained interviewers or a structured interview format, emphasizing confidentiality, using information gained to make positive changes that include managers, and cross-checking exit interview, survey results with other data sources are recommended techniques for enhancing their validity and gaining accurate data (Allen, 2008). We used a third-party vendor to administer a standardized assessment, cross-referenced our results with detailed drill-down analyses, and also worked with nursing and nonnursing unit managers and department directors to facilitate positive changes identified from our literature search.
One of the most striking successes we experienced came from providing our managers and supervisors with a standardized onboarding format to use for supporting new hires. There were several hospital and nursing units where losses were especially significant. Creating a buddy system with high-performing employee leaders, posting new-hire profiles for other employees to learn about the new hire, requiring manager communications at frequent intervals, and implementing 30-, 60-, and 90-day structured interviews allowed challenged departments and units to address problems early. Improved coworker relationships and employee–manager professional dialogue during the new hire’s first 3 months promoted an improved work environment and promoted staff retention. The standardized process positively influenced our workplace culture by ensuring that the employee had at least three sessions of designated one-on-one time with their manager in the first 90 days of employment, where three formal “stay interviews” were completed along with an essentials checklist (Table 3). During these sessions, the manager reviewed the department Mission, Values, and Service Excellence Goals as well as unit norms, safety plans, and structure standards. Because the stay interviews were designed to gather information about the new employee as well as provide information, managers sometimes found that the new employee’s fresh perspective led to unit improvements. Designation of a Unit Champion provided new employees with one-on-one assistance whenever needed, helped facilitate coworker networking, provided an accurate source of hospital and unit-specific information, and promoted acclimation (Johns Hopkins University, 2012; as cited in Barbazette, 1994). All these onboarding steps led to improved new employee engagement and improved unit culture.
Also key to obtaining a successful outcome was that hospital administrators and leaders ensured our departmental managers viewed the initiative as a priority. For example, when the VPHR initially presented the onboarding program to all administrators and department managers, our CEO made it clear he was in favor of the program and managerial compliance was expected. The CEO received quarterly updates from VPHR on how effectively the managers were completing the 30-, 60-, 90-day interviews in addition to any pertinent trends or concerns. The VPHR then presented summary turnover data by department at monthly department manager meetings where hospital administrators were in attendance. Department managers who were not following through were required to develop a corrective action plan and present it to an administrator to ensure compliance was achieved. Finally, potential compliance barriers for hiring managers were identified and addressed as much as possible before starting the program. To alleviate the burden of adding a new initiative to their all-encompassing roles, department managers were provided as many supportive resources as possible up front. Upon offer acceptance, the recruiter would prepare an onboarding packet for the hiring manager which contained all the necessary checklists and documents needed for their new hire.
Strengths and Limitations
This project presents the implementation of a well-researched hospital staff turnover reduction initiative at a medium-sized community hospital facility. The initiative was designed after extensive review of the human resources literature, industry exemplar practices, and by conducting detailed drill-down analyses of hospital turnover data. The initiative was supported by executive leaders and received interdisciplinary support from hospital supervisors and nursing managers in implementing a comprehensive 10-point plan specifically targeted to retain new-hire employees.
While we were able to drive down our hospital and nurse turnover in 2013 and 2014, especially that of new-hire employees, we were not able to sustain low turnover rates on a longer term basis. In November 2015, follow-up turnover metric outcomes identified a 57% increase in our voluntary turnover losses where staff left their positions for a better career opportunity (n = 20 in 2014 and n = 33 through November 2015). During that same time, we also observed a 20% increase in voluntary turnover due to relocation. November 2015 drill-down analyses identified that while our voluntary new-hire losses (<1 year employment) continued to be stable, voluntary turnover of staff with 1 to 4 years’ of service climbed to 43%. The 1- to 4-year turnover trend was not reflective of our program or its implementation, but rather represented newly emerging issues in our facility’s workforce and the surrounding regional labor market.
Although our initiative was sustained for a period of time, the program’s focus developed into completing the required tasks rather than nurturing longer term, lasting relationships with new staff. As with many new initiatives, the meaningfulness of the tasks can become overshadowed by other priorities. We are currently retooling our peer interview process with the addition of a validated assessment tool. Earlier this year, we rolled out purposive employee rounding, where department directors meet with their direct reports on a monthly basis and ask many of the questions asked of new hires. Long-term sustainability of the program would benefit from reducing the unit Directors’ and supervisors’ workload in administering the program. For example, some units can onboard 2 to 10 new-hire employees at once depending on the department and time of year. Possible ideas to consider include enlisting the help of charge nurses, senior nurses aiming to complete clinical ladder requirements, and new-hire champions to perform some of the program’s interview and documentation requirements.
We did not formally include organizational outcome measures suspected to be impacted by turnover for our pre- and postintervention statistical analysis (i.e., such as adverse events, national nursing quality indicators, and Hospital Consumer Assessment of Healthcare Providers and Systems scores). However, we noted anecdotal improvements on a number of relevant quality and safety indicators that were possibly impacted by our intervention. At the conclusion of 2013, Catheter-Associated Urinary Tract Infections decreased by 28%, Surgical Site infections decreased by 40%, and staff injury rates were 8% lower than the corporate and state rates for the year. There were a number of patient satisfaction score improvements as well.
Labor and Nursing Implications
As with any turnover analysis information, the labor and nursing implications of a hospital’s turnover metrics should be interpreted in the larger context of national and regional workforce trends. While our hospital must now turn and address an emerging challenge of retaining staff at 1 to 4 years’ of service, we identified that some of our internal turnover dynamics are being impacted by external factors. For example, in 2012, our hospital began a $40 million expansion including the addition of 180,000 square feet of medical offices, a new pediatric emergency room, and expanded inpatient and outpatient surgical service infrastructure and resources. Additionally, our parent company expanded into a neighboring county with a new 124 bed hospital, which opened in December 2015. Thus, any hospital aiming to develop and implement a turnover reduction plan should appreciate the broader labor, staffing, and environmental contexts that will influence their initiative design efforts.
As the economy has grown since the Great Recession in 2008, so does turnover—national health-care turnover is currently estimated at 17.1% and has increased annually from 13.5% since 2013 (NSI Nursing Solutions, Inc., 2015). This means that as economic health improves, employees feel more secure and are willing to assume risks associated with relocation and seek improved employment conditions. Our facility is situated in Northern Virginia and is part of metropolitan Washington DC’s health-care market. Northern Virginia has experienced a sustained rate of significant population growth, demonstrates extraordinary racial and ethnic diversity, is comprised of a high percentage of workers >55 years old, is highly educated, and is susceptible to intense competition for qualified workers (Billingsley, 2011). Turnover was low during the Great Recession for all health-care occupations in Northern Virginia through 2008–2011, and nurses in particular postponed retirement (Altstadt, 2014).
The Washington DC metropolitan health-care market is complex and characterized by multiple, overlapping hospital submarkets, with most hospitals belonging to several systems, including: Inova, MedStar, Hospital Corporation of America, Sentara Healthcare, Johns Hopkins Health System, Trinity Health, and Universal Health Services. Hospitals in the region are experiencing significant uncertainty associated with the value-based payment transitions, are experiencing increased geographic competition, and are rapidly expanding their ambulatory care networks into broader overlapping areas (Koskinas & Giovanis, 2014). These market realities translate into competing employment opportunities for needed health-care workers and nurses to staff health-care operations. For example, in 2012, 78.2% of employers in Northern Virginia seeking RNs desired an experience level of 1 to 4 years (Altstadt, 2014).
Hospitals often use a mixture of short- and long-term strategies to retain health care and nursing staff, such as: temporary staffing, bonuses and other financial incentives, training opportunities (i.e., clinical ladders), clinical and nursing school partnerships, flexible scheduling, shared governance, Magnet credential application, care delivery changes, and communication model improvements (May, Bazzoli, & Gerland, 2006). However, hospitals focusing on modifiable factors that promote employee autonomy and supportive work environments over a long-term period are best situated to increase staff retention (Han, Trinkoff, & Gurses, 2015).
While regional demographic and health-care market factors impacting our hospital are complex and rapidly shifting, our current action plan is to first maintain the progress we made on new-hire turnover losses (<1 year employment). Second, we must replicate our 2013 turnover reduction intervention process with a specific focus on professional development tactics for employee staff retention with 1 to 4 years of service using a mix of the strategies presented herein. Our next turnover reduction plan will incorporate a longer term focus and include strategies to navigate the region’s competitive market realities. Since we have a proven road map from a well-researched effort to attain these aims, we are confident that consistent follow-up with departmental managers on proper use of targeted initiative elements will improve our recent 1- to 4-year turnover increases.
Conclusion
In 2012, our medium-sized metropolitan community hospital was experiencing increasing and unsustainable levels of hospital and nursing turnover. Because employee turnover is a key performance indicator that directly impacts a number of critical operational variables, a well-researched and collaboratively designed turnover reduction initiative, such as outlined here, including the contributions of human resources staff, hospital executives, and department/unit management, can serve as a valuable support system and resource. Our hospital’s 10-element onboarding program intervention to reduce annual hospital and nursing turnover is one such initiative, and like any successful plan—needs executive oversight, sustained management accountability, and continuous reevaluation in the context of national and regional policy and workforce trends to continually ensure long-term success.
Footnotes
Acknowledgements
We gratefully acknowledge members of the Human Resources Turnover Committee for their assistance with research, program design and training, template development, and program implementation. We thank our facility's Executive Administration Team for their kind support of this work. We thank Strategic Programs, Inc. for exit survey data collection assistance. Thanks to Ms. Gillian Zeile, BSN, RN, Case Western Reserve University Master's student for manuscript preparation assistance. We also thank Resources, Inc. personnel for their research literature retrieval service support: Dr. Roberta Miller, EdD, MALS, President; Mr. Markus Compton, Chief Operations Officer; and Ms. Agnes Fortune, Northern Virginia Medical and Legal Retrieval Services.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.