
Abstract
Systemic autoimmune rheumatic diseases (SARDs), like rheumatoid arthritis and systemic lupus erythematosus, impose significant burdens on patients. This cross-sectional survey explores knowledge sources about SARDs, emotional and practical support from family and peers, and willingness to disclose their condition publicly, particularly through social media, among a Middle Eastern population. A descriptive, cross-sectional study was conducted at the University Hospital (Abha), the University Hospital (Makkah), and Alhabib Private Hospital (Jeddah), involving 301 adults aged 18 to 50 with SARDs. A structured questionnaire assessed sociodemographic data, clinical information, support systems, and disclosure practices. Data were analyzed using SPSS v25.0 (P < .05). In total, 84.7% of participants received disease information from their treating physicians, while 50.2% turned to social media. Over half (55.1%) felt supported by families, and 49.5% noted workplace cooperation. However, 32.2% cited fear of stigma, and 14.6% felt like a burden as barriers to disclosure. Enhancing patient education, expanding support groups, and raising awareness about autoimmune diseases are vital for improving social support and encouraging disclosure without stigma.
Keywords
Introduction
Systemic autoimmune rheumatic diseases (SARDs) encompass a spectrum of chronic inflammatory conditions affecting the musculoskeletal system and connective tissues. 1 These inflammatory conditions include rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and psoriatic arthritis (PsA). These conditions are often manifested as persistent joint pain, stiffness, and fatigue that substantially reduce patients’ mobility and quality of life. 1 Beyond their physical impact, SARDs pose considerable psychological challenges, including depression and anxiety, which stem from prolonged pain, limited daily functioning, associated fibromyalgia, and concerns about disease progression. The prevalence of anxiety and depression in RA patients reached 18.6% and 9.4%, respectively, which is above the baseline of anxiety and depression that accounts for 6.3% and 4.92%, respectively. 2 In Saudi Arabia, the reported prevalence of SARDs is approximately 8.7%, with RA comprising 40% of the diagnosed cases. Despite the relatively increased incidence in the last decade, public acquaintance and understanding of SARDs are still deficient, resulting in misconceptions and stigma. 3 Patients frequently struggle with whether and how to expose their medical illness to the surrounding community, ranging from close relatives to colleagues at the workplace, weighing the potential benefits of open communications, such as increased support and understanding, against the risks of negative stereotyping or discrimination. 4 Personal and cultural factors, including perceived disease aspects, anticipated reactions from others, and family burden, strongly influence the open discussion. In Middle Eastern societies, where family bonds and collective identity hold particular importance, discussing chronic illnesses can be especially delicate, prompting many individuals to opt for selective disclosure to avoid social repercussions. 4 Although treatment strategies for SARDs have improved, the psychosocial aspects, particularly around breaking the diagnosis and the long-term management, remain underexplored in Saudi Arabia, and patients who fear stigmatization or receive inadequate support may delay seeking specialized care, worsening long-term outcomes. 3 Patients seek other sources due to the limited time in the clinical visits, and more importantly, the limited global acknowledgment about SARDs. A patient might consult someone with a similar disease or symptoms, search medical articles, or browse lay websites and social networks. All will shape their beliefs about the disease and influence coping strategies.3,5 Therefore, we should be more cautious about the educational gaps and references that our patients seek. This study aims to highlight what Saudi patients navigate to nourish their understanding of SARDs and whether their relatives and colleagues are providing adequate help through supportive societies, enlightening the solidity of the support received from the surroundings, and to what extent Saudi patients with SARDs are liberated to share their condition with others. Although these factors are discussed in the existing literature, limited research discusses them in the Saudi population. This cross-sectional study builds on previous studies by addressing the gaps in the existing literature that discusses sources of knowledge, family and peer support that Saudi patients with SARDs receive, and their willingness to disclose their medical status on social media platforms.
Methodology
Study Design and Setting
This is a descriptive, cross-sectional study conducted in Saudi Arabia at the University Hospital (Abha), the University Hospital (Makkah), and Alhabib Private Hospital (Jeddah). The study was conducted using a survey-based approach. The survey was conducted among adult patients with autoimmune rheumatic disease between November 2024 and December 2024.
Inclusion Criteria
We included adult patients aged between 18 and 50 years who are diagnosed with 1 or more of the following SARDs: RA, SLE, Sjögren's syndrome, Behçet's disease, PsA, ankylosing spondylitis (AS), systemic sclerosis, inflammatory myositis, vasculitis, and antiphospholipid syndrome.
Exclusion Criteria
We excluded patients who were unwilling to give informed consent or patients older than 50 years, as patients above this age are not active users of these platforms and are unlikely to utilize social media to seek medical information or peer support. 6 Patients diagnosed with non-SARD musculoskeletal conditions, such as osteoarthritis, crystal-induced arthropathy, and fibromyalgia, were also excluded.
Sample Size
A total of 385 participants were included, ensuring a 95% confidence level with a 5% margin of error. The sample size was determined using the following formula: n = z2 × p(1 − p)d2, where z = 1.96 (for 95% confidence), p = 0.50 (to account for maximum variability), and d = 0.05 (margin of error).
Questionnaire Development and Pretesting
In this survey, we did not use a specific index to measure the patient's support domain. The questionnaire combined a literature review and insights from 3 rheumatologists with over 5 years of experience. Support levels were categorized into an ordinal scale (enough support, somewhat, and no support). Initially drafted in English, it was translated into Arabic for native speakers. The translation was done by a professional translator familiar with medical terms. The questions covered 5 domains: demographics disease characteristics, sources of information, support level, disclosure behavior with barriers, and the role of supportive social groups. The survey included nominal and ordinal items, with some open-ended questions, such as other sources or other reasons.
Pretesting and Validation
A pilot test with 15 patients diagnosed with SARDs evaluated the questionnaire's clarity, relevance, and comprehensibility. Their feedback refined the question wording, format, and structure. Internal consistency was assessed using Cronbach's alpha, which resulted in a strong reliability value of .85. These refinements ensured the questionnaire effectively captured patients’ experiences regarding disease disclosure, knowledge sources, and support systems, aligning with best practices in qualitative research on workplace disclosure and chronic illness management. 4
The questionnaire comprised 5 sections that were based on a literature review and verified by 3 rheumatologists with over 5 years of experience. The first gathered sociodemographic data, including age, gender, marital status, education, and employment. The second focused on clinical details like SARD diagnosis, disease duration, treatment history, and information sources. The third assessed perceived emotional and practical support from family, friends, colleagues, and healthcare providers. The fourth explored disclosure behaviors and barriers, such as willingness to discuss the diagnosis, fears of stigma, concerns about burdening others, and anticipated negative reactions. The final section examined participants’ perceptions of sharing their disease journey on social media to gauge engagement with the broader community.
Survey Administration
The survey was conducted in 2 formats: a digital version via a Google Forms link distributed through WhatsApp groups, which included unique tracking to prevent duplicates while ensuring anonymity, and a paper version provided to about 20 patients at the University Hospital in Abha, with assistance available, whereas the other 2 hospitals only received digital forms for convenience. The paper surveys were only given to hospital participants, maintaining confidentiality.
Data Collection Process
Data collection lasted 1 month, with participants completing surveys during clinic visits or at home. Completed paper surveys were securely stored and later integrated with digital results by the statistician. The majority of participants were WhatsApp survey respondents, and the survey was not restricted to participants from a certain hospital. The rheumatologists in this study were usually referring their patients to the support group coordinators; however, several participants had been transferred to or from another rheumatologist, were missing follow-up, or were newly diagnosed. Therefore, it was difficult to identify the characteristics of the participants who rejected or accepted engaging in the support groups.
Bias
This study acknowledges potential bias resulting from recruiting participants only from a hospital-based setting, which may limit generalizability. Additionally, the exclusion of SARD patients over 50 years old because they are less likely to use social media for peer support or for obtaining medical information may have caused age-related selection bias. Therefore, efforts to minimize bias included using paper formats and online survey formats across 3 hospitals in 3 different cities to increase diversity among the represented population in the study.
Statistical Analysis
Frequencies and percentages characterized categorical data, while means and standard deviations (SD) were calculated for continuous variables. Chi-square tests assessed correlations between support levels and disease characteristics, with significance at P < .05. Data analysis was performed using SPSS version 25.0.
Results
Sociodemographic Characteristics
This study included a total of 301 participants. The mean age was 36.7 years, with females constituting 89% of the sample. About 52.8% were married versus 47.2% unmarried (42.9% single, 2.3% widowed, and 2% divorced). The majority have a higher education level (68.4%), followed by those who had a high school education level (21.9%), and only 2% were illiterate. The majority of the participants were housewives (46.2%); 32.9% were employees; 13% were still students; and the minority were unemployed (Table 1).
Sociodemographic Characteristics and Sources of Knowledge About Autoimmune Rheumatic Diseases Among Participants (n = 301).
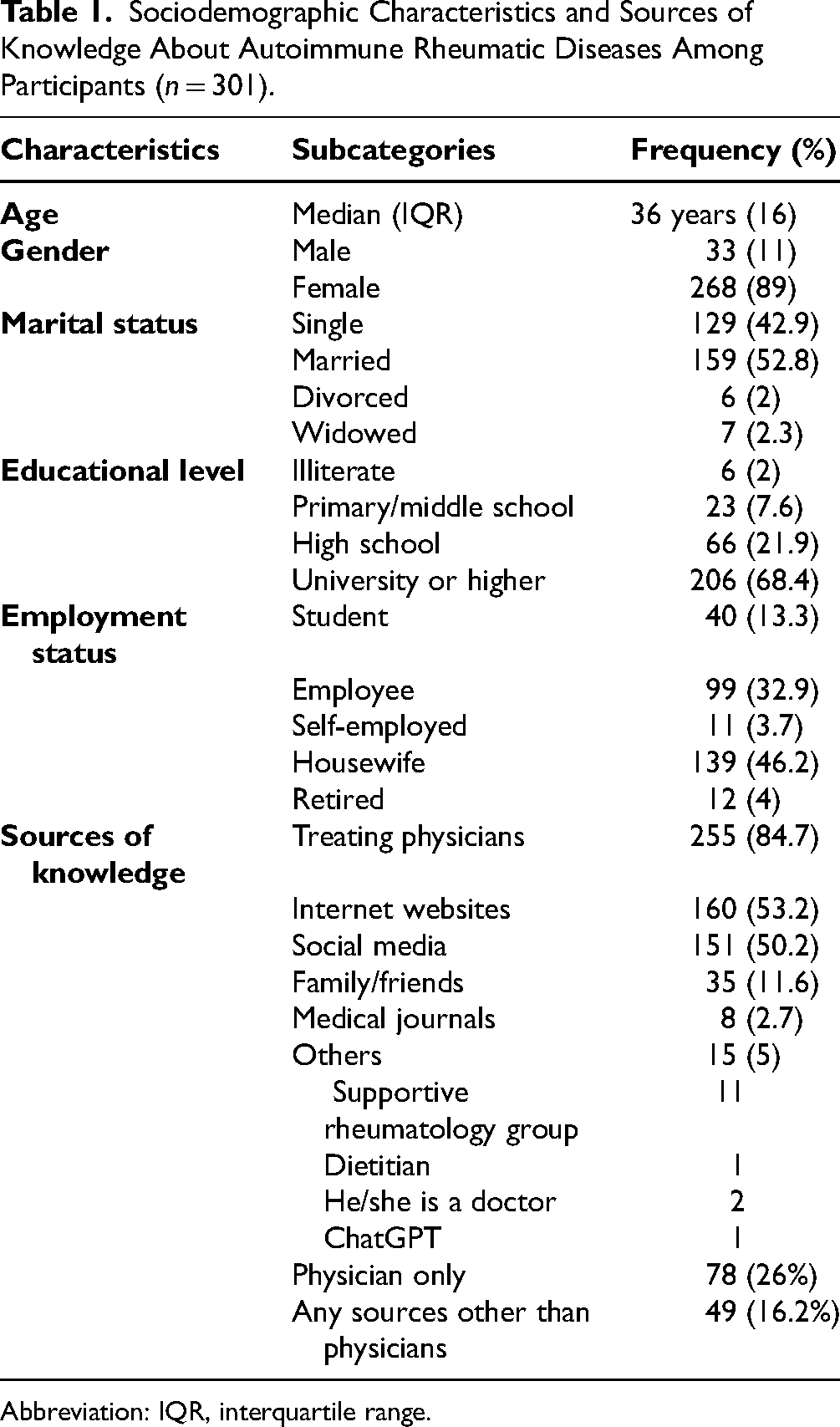
Abbreviation: IQR, interquartile range.
The SARD Characteristics
RA was the most prevalent autoimmune rheumatic disease among the participants (42.9%), followed by lupus (27.9%) and scleroderma (9%). The least common were inflammatory myositis and vasculitis (1.7%) and antiphospholipid syndrome (0.3%) (Figure 1a). The majority of disease courses were between 1 and 5 years (46.9%), and less than 10% were diagnosed in less than a year. The majority of the participants (84.7%) chose physicians and medical staff as their source of knowledge regarding autoimmune rheumatic diseases, and 26% of them relied solely on their physician's discussion. More than two-thirds (74%) were seeking other sources, most commonly internet websites and social media platforms, such as Twitter, Instagram, and Snapchat (53.2% and 50.2%, respectively) (Table 1).

(a) Proportion of different autoimmune rheumatic diseases among participants. (b) The percentage of patients who share their autoimmune disease story with people through social media, such as Twitter, Snapchat, Instagram, TikTok, and Facebook. (c)The percentage of participants who joined a supportive group, such as the Saudi Society of Rheumatic Diseases.
Disease Disclosure and Receiving Support from the Surroundings
More than half of the participants reported receiving adequate support from their families and spouses (55.1% and 53.6%, respectively), while a minority indicated no support from family and spouse (7.9% and 11.3%, respectively). Only a third were satisfied with their friends’ support (31.2%). About half (49.5%) experienced satisfactory cooperation with workplace staff, while 15.9% worked in an uncooperative environment (Table 2).
Social Support, Disclosure, Perceptions, and Barriers to Joining Supportive Groups.

Most participants (52.8%) felt comfortable discussing their condition with family. However, they were less open with social gatherings (22.6%) or colleagues in the work/study place, and 42.2% and 55.5%, respectively, preferred to be selective (Table 3). The most reported barrier to disclosure was fear of being labeled sick (32.2%), followed by concerns about being a burden (14.6%), and anxiety about discussing their condition (12%), in addition to other participant-identified reasons (Table 2).
Factors Associated With Family Support.

Abbreviations: OR, odds ratio; CI, confidence interval; RA, rheumatoid arthritis; AS, ankylosing spondylitis; PsA, psoriatic arthritis.
*Significant association.
Sharing Disease Experience and Knowledge Through Social Media Platforms
The majority of participants (68.2%) did not share their experience through social media platforms, whereas only 31.9% of participants did (Figure 1b). Among those who responded with No, 32.6% believed that sharing their problem with others with similar conditions would help them accept and understand it better, and 29.6% wanted to share for educational purposes, as they felt it would make other people understand and nourish their knowledge about autoimmune diseases. On the other hand, 25.9% saw no advantage in sharing their experience (Table 2).
Participation in Supportive Groups for Rheumatology Patients
Only 18.9% joined one of the supportive societies or groups, and the majority (81.1%) did not (Figure 1c). The most reported reasons were being group Naive (52.8%) and lack of time (14.6%) (Table 2).
Correlation Between Family Support and Disease Characteristics
The chi-square analysis depicts that the overall educational level was the only factor that showed association with receiving family support (P < .05), and there was no significant association between receiving family support and gender, SARD subtype, disease duration, and marital status (Table 3).
In the logistic regression model (Table 3), participants with postsecondary education had significantly higher odds of receiving less support than other subgroups (odds ratio [OR] 2.7, 95% confidence interval [CI]: 1.03-7.2). Additionally, individuals over 30 years received less support than younger age groups (OR 9.3, 95% CI: 1.2-75).
Discussion
The emotional and physical wellness of patients with chronic conditions is shaped by their social connections, including spouses, family members, and friends. 7 Social constraints and lack of optimum support may have a drastic effect on the overall well-being of these individuals, especially from family members and spouses.7,8 This cross-sectional study addressed issues among patients with rheumatic diseases in the Saudi population. Among 301 patients with autoimmune diseases, over two-thirds completed university-level education, which may correlate with better health literacy and the ability to seek information. However, older patients reported less support from their surroundings. RA was the most common disease, followed by lupus and scleroderma, with the latter being more prevalent in this study due to recruitment from specialized clinics. Most participants received information from their physicians, but a quarter relied solely on the internet, possibly due to their higher education levels. However, these findings contrast with the results of a previous study conducted by Garneau et al 9 among RA patients, in which the internet was the most utilized source of information. Another study conducted by Barahona-Correa et al 10 evaluated the quality of YouTube videos for patients with RA and found that 67% were considered useful according to metrics such as view count, time online, and video duration. The results of this study confirm the results of the Garneau et al study and contrast with the results of our study. In line with these results, Erdogan et al 11 surveyed 399 rheumatic diseased (RD) patients; 74% of them agreed that social media platforms provided them with effective health information. 11 However, the abundance of unreliable information available online contributes to relatively low and harmful value, and in some cases, affects medical decisions and is life-threatening. 12 We are expecting more expansion of ChatGPT utilization for diagnostic and management purposes in the foreseeable future.
Strong familial bonds and understanding are crucial when it comes to coping with any medical condition, which is consistent with psychological theories on the role of support. 13 In our study, we found that 55.1% and 53.6% of patients expressed satisfaction with the support and attention they received from their families and spouses, respectively. Conversely, the remaining participants reported either moderate satisfaction (37.2% and 35.1%, respectively) or a complete absence of perceived support (7.9% and 11.3%, respectively). These findings surpassed our expectations concerning the emotional well-being of our patient population. In alignment with our findings, 2 studies conducted on patients diagnosed with SARDs demonstrated that elevated levels of spousal support are positively correlated with enhanced psychological adjustment to the patients’ condition. This improved psychological well-being, in turn, is associated with greater adherence to treatment regimens and increased overall life satisfaction.14,15 Nearly half of the participants reported that their managers and colleagues in the workplace were cooperative and understood that their medical condition could sometimes interfere with their performance, while a minority reported never receiving any cooperation. These findings are higher when compared to a previous study conducted by Jetha et al, 16 where more than half of the participants (53%) reported they did not receive the needed support from their work supervisors. The significance of this issue is particularly pronounced for young patients who often perceive their condition as an impediment to securing stable employment, maintaining productivity, and achieving professional advancement. When it comes to transparency regarding their rheumatic conditions, these individuals tend to adopt a more reserved approach in conversations with coworkers or during social gatherings, exercising caution in their discussions about their illness. This reticence can lead to a bidirectional impact; negative interactions with relatives and friends may increase stress levels, thereby exacerbating depressive symptoms. It is essential to understand the implications of this dynamic not only for the well-being of these patients but also for their social and professional integration.17,18 Ostuzzi et al 19 conducted a study that challenges previous findings, involving a sample of 250 working patients with RA. Their research revealed that a significant 81.2% of participants disclosed their condition to coworkers. This disclosure was found to be correlated with both the patients’ perceptions of their illness and the duration of the disease. These results suggest that personal and contextual factors may play a critical role in the decision to share one's health status in the workplace. Similar positive results found that interacting with colleagues helps patients with SARDs to get distracted from daily fluctuating symptoms and redirects them toward better adherence to medications.20,21 From our perspective, this situation poses potential risks, as patients may experience insecurity when confronted with more detailed inquiries regarding their condition. This apprehension can be attributed to the currently low level of societal acceptance of SARDs, as previously discussed. The predominant concerns expressed by patients in our survey included feelings of being labeled as “sick,” perceived as a burden, and heightened anxiety. These findings highlight the pervasive stigma associated with autoimmune diseases and reflect broader societal attitudes toward health and illness, which in turn obstruct open communication and honest disclosure.
Moreover, while the majority of our patients have refrained from sharing disease-related content on their social media accounts, social barriers continue to prevent approximately one-third of participants from engaging with these platforms. This proportion is noteworthy, especially against the backdrop of existing conservative cultural norms, indicating that the reluctance to disclose personal health experiences is influenced by more than just individual choice. A similar proportion of participants posting about their disease was found in the survey conducted by Cline and Haynes. 12 Social media serves as an effective platform for discussing medical conditions and disseminating information about advancements in treatment options.22,23 Additionally, it provides a feasible and cost-efficient means for patients to share their health experiences and receive constructive insights and feedback on the challenges they face. 24 Notably, patients living with SARDs often offer valuable and practical strategies to address functional disabilities, thereby enhancing overall quality of life. 25 Venuturupalli et al 26 used Twitter as a channel to obtain data on patient-reported outcomes among lupus patients, highlighting the value of social media in capturing clinically relevant data directly from patients’ perspectives.
The findings of this study indicate that a significant proportion of participants has not engaged with supportive groups for rheumatology patients, primarily due to a lack of awareness regarding their existence. Existing literature suggests that peer support plays a crucial role in the recovery process, as it cultivates a sense of community and belonging, particularly among those who may perceive themselves as burdens to their caregivers.27,28
Future Recommendations and Policy Implications
The results of this study entail several recommendations that can be made to improve the quality of life of Saudi patients with SARDs. For instance, it is imperative to educate patients about the availability of these groups during the counseling process, particularly for individuals who may feel hesitant or ashamed to disclose their condition to peers. Physicians and rheumatologists can play an essential role in educating their patients about the existence of support groups and their benefits for their well-being. National health authorities should establish associations and collaborations to provide support groups either online or offline for SARD patients to ensure that they receive both support and trusted medical information. Additionally, several campaigns should be made to increase awareness among the population regarding SARD symptoms and their physical and psychological effects on the patients, which will result in the encouragement of patients to disclose their medical status and avoid the stigma.
Strengths and Limitations
To our knowledge, there have been no comparable studies conducted in Saudi Arabia or the Middle East concerning this topic; thus, this research serves as a foundational contribution to the existing body of evidence. The survey was administered to a diverse cohort of patients across multiple healthcare centers within various regions of the Kingdom, which enhances the robustness and generalizability of the findings. Nonetheless, it is essential to acknowledge the potential for selection bias, given that participants were primarily recruited from scleroderma clinics and that the study was limited to a specific age group. Furthermore, as this research employed a cross-sectional design, it is not feasible to draw causal inferences from the data. Future prospective studies are warranted to further elucidate the dynamics of social support and disclosure over time and their subsequent impact on disease trajectories.
Conclusion
Patients diagnosed with SARDs require enhanced support and care from their families, friends, and spouses to promote their overall well-being in the context of their ongoing struggle with the disease. Research has demonstrated that emotional and social support from loved ones can significantly alleviate symptoms and bolster psychological health in these individuals. Therefore, there is a pressing need to facilitate patient-centered public webinars and symposiums that focus on SARDs. Additionally, increasing public awareness through social media and various broadcasting channels is essential to educate the community about the complexities of SARDs and their profound impact on patients’ quality of life.
Footnotes
Author Contributions
HA: writing the methodology, the statistical analysis and the reviewed/edited the manuscript. KA and WH: writing the discussion. AA, MA, MA, AA and AA: survey distributions and data collection.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent
Ethical approval for the study was obtained from the Institutional Review Board at King Khalid University Hospital, under approval number ECM#2024-2203. Additionally, written informed consent was secured from all participants, with materials provided in Arabic to ensure comprehension and compliance.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.