
Abstract
Objective
Hyperlipidemia guidelines do not currently identify inflammatory arthritis (IA) as a cardiovascular disease (CVD) risk factor. We compared hyperlipidemia treatment of individuals with and without IA (rheumatoid arthritis, psoriatic arthritis, or ankylosing spondylitis) in a large national cohort.
Methods
Participants from the REasons for Geographic And Racial Differences in Stroke (REGARDS) study were classified as having IA (without diabetes or hypertension); diabetes (but no IA); hypertension (but no diabetes or IA); or no IA, diabetes, or hypertension. Multivariable logistic regression models examined the odds of medical treatment among those with hyperlipidemia.
Results
Thirty-nine participants had IA, 5423 had diabetes, 7534 had hypertension, and 5288 had no diabetes, hypertension, or IA. The fully adjusted odds of treatment were similar between participants with IA and those without IA, hypertension, or diabetes. Participants with diabetes and no IA and participants with hypertension and no IA were twice as likely to be treated for hyperlipidemia as those without IA, diabetes, or hypertension.
Conclusion
Despite their higher CVD risk, patients with IA were as likely to be treated for hyperlipidemia as those without diabetes, hypertension, or IA. Lipid guidelines should identify IA as a CVD risk factor to improve CVD risk optimization in IA.
Keywords
Introduction
The risk of cardiovascular disease (CVD) is increased among patients with inflammatory arthritis (IA) (including rheumatoid arthritis [RA], psoriatic arthritis [PsA], and ankylosing spondylitis [AS]).1,2 This increased risk is possibly related to accelerated atherosclerosis in the context of chronic inflammation.3,4 Several studies have shown a 50% to 60% higher risk of death from myocardial infarction and stroke in patients with RA than in the general non-RA population,5–7 with the standardized mortality ratio attributable to CVD ranging from 1.13 to 5.15.8,9 An increased risk of CVD has also been reported in patients with PsA and AS.10–12 Like patients with diabetes mellitus (DM), patients with RA have a two-fold higher risk of CVD compared with the general population.13,14 Evidence-based guidelines have been promoted to optimize the CVD risk in high-risk populations such as those with DM, resulting in higher awareness of the CVD risk in patients with DM among primary care physicians. However, these guidelines do not currently mention IA as a risk factor for CVD. Thus, CVD risk reduction in this high-risk population may not be strongly emphasized by these doctors. 15
Management of the risk factors for CVD, such as high cholesterol levels, can reduce the risk of CVD; however, such management may be suboptimal in patients with IA. 16 For example, a recent study reported that about 40% of patients with RA who had CVD risk factors were not screened for hyperlipidemia even after having experienced a CVD event. 17 However, few studies have examined hyperlipidemia treatment patterns in patients with IA among those with an elevated CVD risk. We used data from the national REasons for Geographic And Racial Differences in Stroke (REGARDS) cohort to compare hyperlipidemia treatment of participants with and without IA, controlling for individual-level factors that influence utilization of health services as conceptualized by Aday and Andersen. 18
Methods
Participants
List of medications for autoimmune disease used to identify participants with inflammatory arthritis within the REGARDS cohort.

Variables
The Aday and Andersen framework accounts for individual influences on access to healthcare including predisposing, enabling, and need factors. REGARDS collected detailed information regarding many variables within each construct of this framework. 18 These variables were collected at the time of the REGARDS baseline through telephone interviews, self-administered questionnaires, and in-home examinations. Information included the participants’ age, race, sex, region of residence, education, household income, cigarette smoking status, alcohol consumption, marital status, cognitive function, symptoms of depression, current antihypertensive medication use, use of pills or insulin for treatment of DM, and self-reports of a previous diagnosis of myocardial infarction, coronary revascularization, stroke, abdominal aortic aneurysm, or DM. During the in-home study visits, prescription and over-the-counter medications were documented through a pill bottle review. Participants underwent a physical examination including measurement of systolic blood pressure, which was estimated based on the average of two measurements after a seated 5-minute rest with both feet on the floor. Height and weight were also measured during this examination. Blood samples were collected, and cholesterol levels were assessed in a central laboratory at the University of Vermont.
Statistical analysis
We used descriptive statistics to characterize the cohort according to the four groups of interest: participants with IA only, without DM or hypertension; participants with DM with or without hypertension but no IA; participants with hypertension without IA or DM; and participants without IA, hypertension, or DM. Logistic regression models were used to examine the odds of treatment among the four groups of interest (comparing the first three groups to participants without IA, DM, or hypertension) after accounting for predisposing, enabling, and need factors guided by Aday and Andersen’s model of health services utilization. 18 Missing information was imputed by chained equations with m = 20 imputations and 10 iterations. 21 The analysis was conducted using SAS software (SAS Institute Inc., Cary, NC, USA).
Results
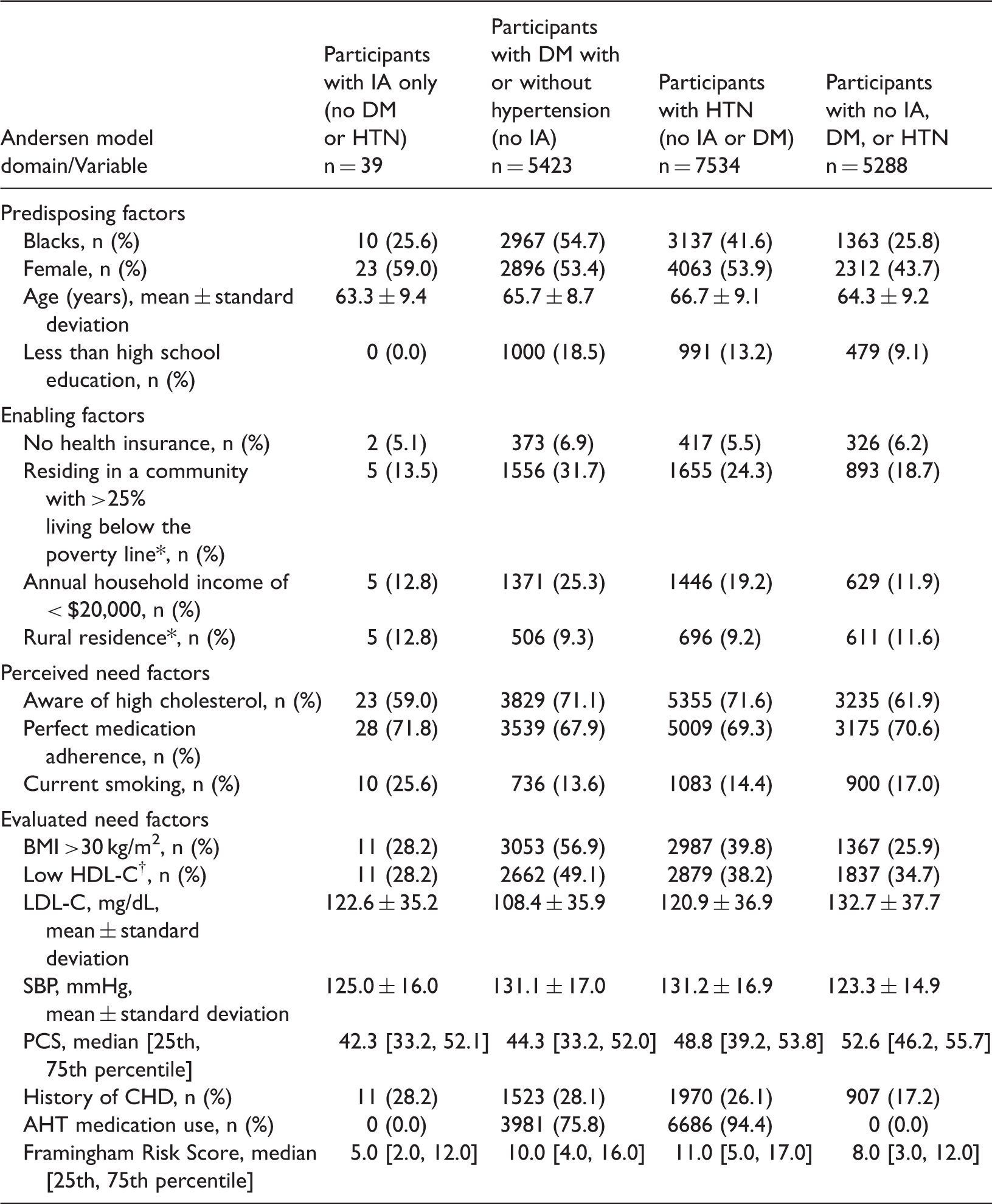
In total, 39 participants had only IA, 5423 had DM with or without hypertension but no IA, 7534 had hypertension but no IA or DM, and 5288 had no DM, hypertension, or IA. Proportionately fewer patients with than without IA were treated with lipid medications (Figure 1). Hyperlipidemic participants with IA were younger and predominately women, with lower Framingham risk scores and lower functional status (Table 2). The unadjusted model revealed that the likelihood of treatment with lipid medications was similar between individuals with IA and individuals without IA, DM, or hypertension. The fully adjusted odds of treatment for participants with IA were 27% lower than the odds for participants without IA, DM, or hypertension, or IA, although the difference was not statistically significant (Table 3). Participants with DM with or without hypertension but no IA and participants with hypertension and no IA or DM were twice as likely to be treated for hyperlipidemia than those without IA, DM, or hypertension.
Hyperlipidemia treatment among different populations. Characteristics of REGARDS participants with hyperlipidemia
#
at the time of enrollment. Data are presented as n (%), mean ± standard deviation, or median [25th, 75th percentile]. Abbreviations: AHT: antihypertensive, BMI: body mass index, CHD: coronary heart disease, DM: diabetes mellitus, HDL-C: high-density lipoprotein cholesterol, HTN: hypertension, IA: inflammatory arthritis, LDL-C: low-density lipoprotein cholesterol, PCS: physical component summary score, SBP: systolic blood pressure. See Supplement A for definition of hyperlipidemia. HDL-C: Men , <40 mg/dL; Women, <50 mg/dL. *Data based on census tracts. Results of multivariable adjusted analysis for odds of treatment for high cholesterol. Abbreviations: IA: inflammatory arthritis, DM: diabetes mellitus, HTN: hypertension. Hyperlipidemia treatment outcome included treatment with statins, fibrates, or niacin. Unadjusted model included only disease group. ‡Fully adjusted model included race, sex, education, region, health insurance status, neighborhood poverty, household income, rural residence, awareness of hyperlipidemia status, medication adherence, obesity, physical component summary score, history of coronary heart disease, and Adult Treatment Panel III Framingham Risk Score.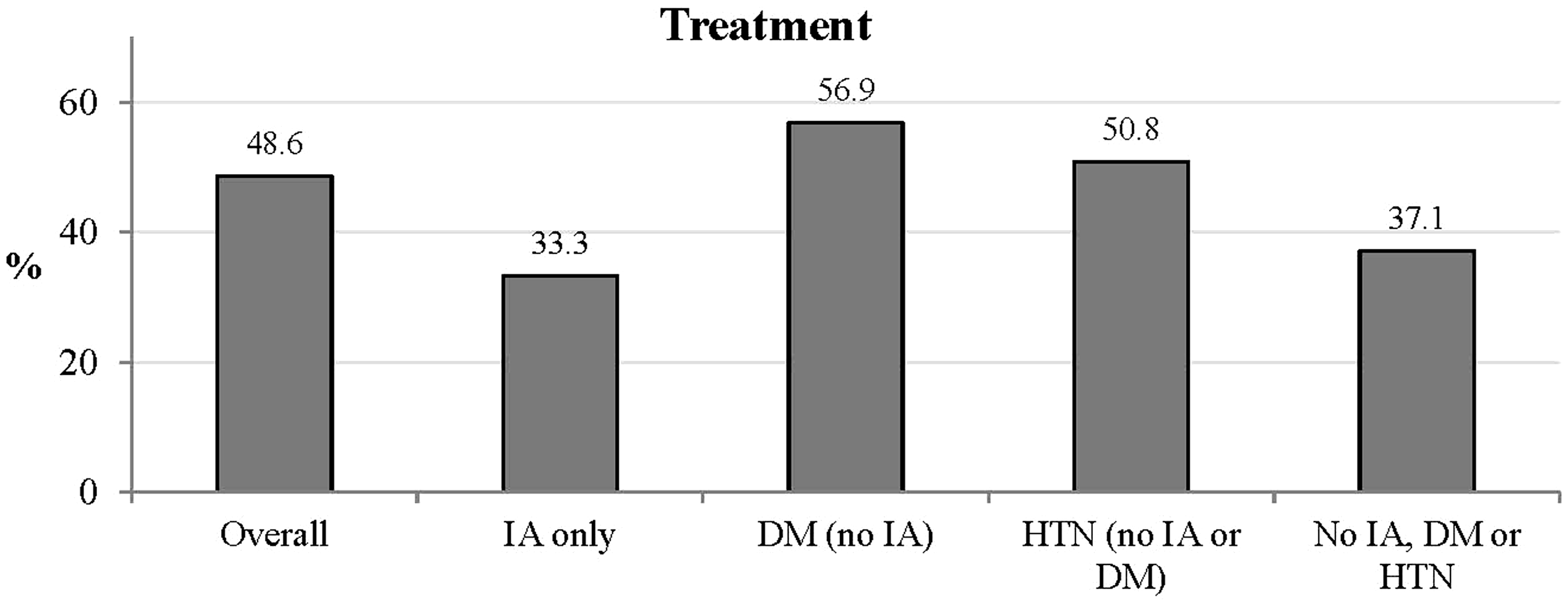

Discussion
In this study, hyperlipidemic participants with IA were less likely to be treated for hyperlipidemia than were participants with DM or hypertension, diseases well known to increase the risk of CVD, even after accounting for the CVD risk level. In fact, those with IA may have had lower odds of treatment than others with a similar CVD risk but without IA, DM, or hypertension, although the small number of participants with IA limited the power of this study. If confirmed in larger samples, these results reflect a potential gap in the management of hyperlipidemia for patients with IA. Because the multivariable models accounted for individual-level factors that influence the utilization of health services, other influences may be at play, such as suboptimal prescribing practices by physicians.
Our results identify a gap in the management of hyperlipidemia, reflecting the need for a multidisciplinary approach that includes rheumatologists and primary care physicians. 22 Clearly establishing which physician is taking the lead in the screening and management of CVD risk factors among patients with inflammatory joint disease is crucial for a successful approach to this comorbidity. Indeed, CVD risk factor management is not commonly within the scope of practice of rheumatologists, who may recognize that their patients with IA are at high risk but may not feel comfortable managing hyperlipidemia. Because clinical practice guidelines for the management of hyperlipidemia do not currently include patients with IA as a high-risk group, primary care physicians may not be as aware of this higher risk in patients with IA compared with those with DM, who are specifically recognized in the guidelines.
Inflammation plays a major role in the acceleration of atherosclerosis in patients with IA. There appears to be usefulness in biomarkers that can serve as a surrogate for endothelial damage, which can lead to accelerated atherosclerosis in these patients. One study identified dimethylarginines as a possible mediator of endothelial damage as well as a biomarker of CVD in patients with RA. 23 More recently, recommendations from the European League Against Rheumatism highlighted the importance of tight control of RA disease activity and inflammation to prevent CVD events. These guidelines emphasize the importance of screening and management of hyperlipidemia as well as other modifiable CVD risk factors not only among patients with RA but also among those with PsA and AS. 24 The benefits of aggressive CVD risk optimization have resulted in decreased CVD mortality among patients with DM. A similar approach may benefit patients with IA, but our results reflect a gap in the current treatment patterns. 25
Our study has several strengths, including the use of data from a prospective cohort that included African-Americans and Caucasians from rural and urban areas in 48 of the 50 United States. Our study has extensive patient-level data, including medications, health behaviors, and physiologic measures, allowing for control of multiple possible cofounders not previously reported. Several limitations should also be noted. IA was defined using medications specific for IA, which could have led to misclassification of some patients, although the specificity of the medications for IA lessens this concern. The small sample of patients with IA is another potential limitation, but the concern is lessened by the very narrow confidence intervals around the point estimates, suggesting little variability in the finding.
In conclusion, the treatment of hyperlipidemia in patients with IA in this sample was suboptimal compared with other conditions known to similarly increase the risk of CVD, such as hypertension and DM. Interventions to improve the treatment of hyperlipidemia in this recently recognized high-risk group may be needed.
Footnotes
Acknowledgements
This research project was supported by a cooperative agreement (U01 NS041588) from the National Institute of Neurological Disorders and Stroke, National Institutes of Health, and Department of Health and Human Service. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Neurological Disorders and Stroke or the National Institutes of Health. Representatives of the funding agency were involved in the review of the manuscript but not directly involved in the collection, management, analysis, or interpretation of the data. The authors thank the other investigators, the staff, and the participants of the REGARDS study for their valuable contributions. A full list of participating REGARDS investigators and institutions can be found at ![]() .
.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
INM was supported by the Rheumatology Research Foundation and by grant K12HS023009 from the Agency for Healthcare Research and Quality. MS and CG were supported by grants R01 HL080477 and K24 HL111154 from NHLBI. JC was supported by NIAMS (grant P60 AR064172). JC and MS received salary support from Amgen.