
Abstract
Human cytomegalovirus (CMV) is a highly infectious virus that is prevalent among adults worldwide. In immunocompetent individuals, CMV infection rarely causes complications. Following initial infection, however, CMV remains latent in the body and can be reactivated especially in immunocompromised patients, such as those with autoimmune inflammatory rheumatic diseases (AIIRDs), leading to tissue-invasive, life-threatening diseases, such as colitis, vascular thrombosis, and pneumonitis. Although there are standard treatment recommendations for symptomatic CMV disease, there is paucity of consensus in the role of primary and secondary antiviral prophylaxis to prevent CMV reactivation, especially in AIIRDs patients undergoing immunosuppressive therapy. Therein, this review aimed to provide an overview of the prevalence, clinical disease, risk factors, and treatment for CMV infection, as well as on the role of primary and secondary antiviral prophylaxis in AIIRDs patients. The emerging novel techniques that measure CMV-specific T-cell immunity as a guide to initiate prophylaxis in high-risk patients were also discussed.
Keywords
Introduction
Human cytomegalovirus (CMV) is a member of the Herpesviridae family, which is a family of viruses that have double-stranded DNA genomes. CMV is a highly infectious virus that affects up to 60% of adults in developed countries and over 90% of adults from developing countries. 1 CMV is primarily transmitted through bodily fluids, namely saliva, blood, breast milk, urine, and vertical transmission from mother to fetus.
Fortunately, unlike other herpesviruses (i.e., herpes simplex virus), CMV usually causes few or no symptoms in immunocompetent patients,2,3 owing to the robust immune reaction to CMV and continuous immune surveillance suppressing any high viral loads, which is a prerequisite to cause serious manifestations in healthy individuals. 4 Possible symptoms of CMV infection include mild flu-like or mononucleosis-like syndrome symptoms, such as fever, myalgia, headache, and fatigue. Immunocompromised patients are susceptible to more severe CMV manifestations, including colitis, pneumonitis, encephalitis, vascular thrombosis, and retinitis. 2 Rarely, immunocompetent individuals may experience systemic syndrome with multiorgan involvement. 3
Following initial infection, similar to the other herpes viruses, CMV remains latent in myeloid progenitor cells for life, where it can be reactivated in later years. 5 During this latent period, CMV remains quiescent, resulting in suppressed viral loads, which remain undetectable during viral load test. Latent CMV infection remains asymptomatic in immunocompetent patients. 6 However, latent CMV may lead to an unspecified febrile, flu-like or mononucleosis-like syndrome and progress to severe and life-threatening infections in immunocompromised patients upon CMV reactivation. 7
Autoimmune inflammatory rheumatic diseases (AIIRDs) are characterized by immune disturbances that cause aberrant B cell and T cell reactivity to normal constituents of a host, leading to formation of autoantibodies, inflammation, and multiorgan dysfunction. 8 They include systemic lupus erythematosus (SLE), rheumatoid arthritis (RA), systemic sclerosis (SSc), vasculitis, and inflammatory myopathies, which are often associated with increased morbidity and mortality rates due to the disease process and infective complications.
The combination of a dysfunctional immune system and ongoing use of immunosuppressive therapy make AIIRDs patients easily susceptible to CMV reactivation and life-threatening complications with resultant increase in morbidity and mortality (9). Furthermore, CMV having immunomodulatory properties can also exacerbate or even trigger the onset of autoimmune diseases by means of molecular mimicry, increased autoantibody formation, inflammation, and nonspecific B-cell activation. 9 CMV-induced autoimmunity has been linked especially with SLE, SSc, and RA. 9
Hence, there is a potential role of antiviral prophylaxis to prevent CzV reactivation in AIIRDs patients undergoing immunosuppressive therapy. 10 Moreover, with the implementation of novel techniques to measure the status of CMV-specific T-cell immunity in patients, 11 it is possible to selectively administer prophylaxis to patients at risk. However, while there are recommendations for antiviral prophylaxis in hematopoietic stem cells and solid organ transplantation patients, there is no consensus regarding their use in AIIRDs patients. Herein, in this review, we aim to present an overview on the prevalence, risk factors and the clinical disease of CMV infection in AIIRDs patients, as well as possible treatment strategies to prevent CMV reactivation.
Methods
A comprehensive search was conducted using Google scholar and PubMed from February until June 2023 using the following keywords: “CMV”, “human cytomegalovirus”, “rheumatic disease”, “autoimmune disease” and “autoimmune inflammatory rheumatic disease”. Due to the limited available literature on CMV, research articles from 2005 onwards were included in this review, provided they were published in English and peer-reviewed.
Prevalence of CMV infection in AIIRDs patients
Studies on the prevalence of CMV in AIIRDs patients.
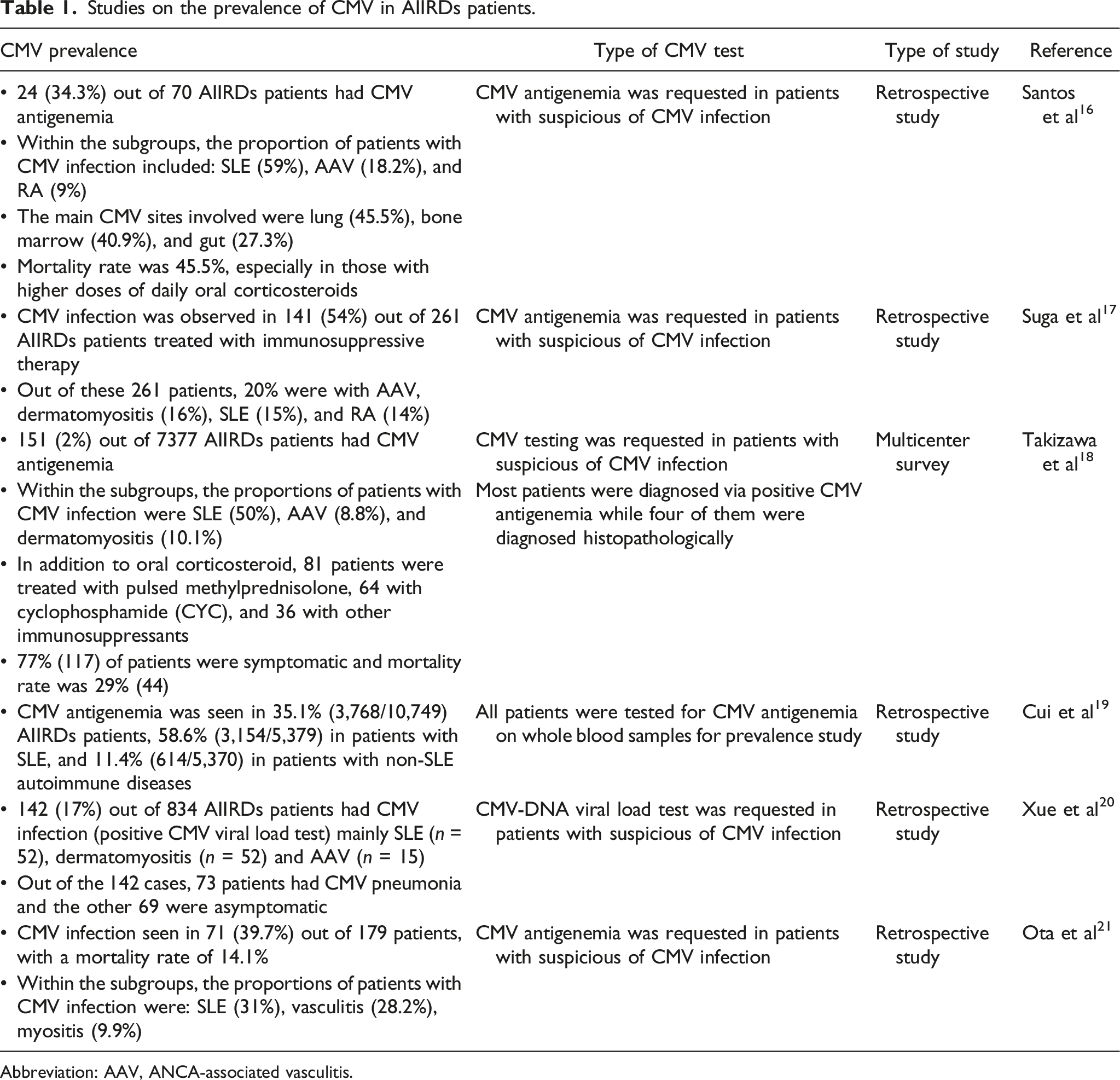
Abbreviation: AAV, ANCA-associated vasculitis.
Spectrum of CMV infection in AIIRDs patients
The spectrum of CMV infection in AIIRDs patients can range from asymptomatic infection to severe and life-threatening diseases. Similar clinical spectrum is also observed in pediatric AIIRDs patients with CMV infection.15,25 During immunosuppressive therapy, AIIRDs patients are known to have “viral blips”. The occurrence of blips, also known as “intermittent viremia”, refers to the transient phenomenon of increase in CMV viral load above the detection threshold in patients undergoing immunosuppressive therapy, and after which the viral load returns to below the lower limit of detection. 26 When CMV viral loads are detectable during this stage, the patients do not necessarily develop clinical disease but remain asymptomatic. However, blips have been associated with an increased risk of developing CMV-related diseases in high-risk transplant patients who undergo immunosuppressive treatment. 27 Hence, CMV viral load positivity in an otherwise asymptomatic patient needs to be interpreted within the clinical context to differentiate between transient viral blip from clinically significant disease and persistent viremia.
In mild cases of CMV infection, patients experience the typical viral syndrome characterized by fever, malaise, leukopenia, thrombocytopenia, and elevated hepatic enzymes. However, with ongoing immunosuppression, resultant high-level viremia predisposes patients to tissue-invasive end-organ disease. 28
For gastrointestinal CMV infection, its clinical manifestations include gastric ulcer, esophagitis, gastritis, duodenal ulcer, and colitis. 29 These patients often present with diarrhea, abdominal pain, hematochezia, hematemesis, dysphagia, fever, and weight loss. 30 Ideally, gastrointestinal diseases require the isolation of tissue biopsy for CMV detection, as it can occur without detectable CMV viremia (25).
Other clinical manifestations of CMV-related diseases are pneumonia,16,18 CNS-related inflammation (i.e., meningitis, encephalitis, and transverse myelitis), 3 bone marrow disorders (i.e., cytopenia), 16 liver conditions (i.e., hepatitis and cirrhosis), 3 and ocular inflammation (i.e., retinitis and uveitis).3,31 In some cases, CMV infection may lead to cutaneous and mucosal lesions from the oral cavity to the anal region. 30 In clinical practice, it may pose a challenge to differentiate organ dysfunction from CMV reactivation as opposed to AIIRDs pathogenesis or adverse medication effect.
CMV infection is also an important trigger of macrophage activation syndrome (MAS), especially in patients with systemic onset juvenile idiopathic arthritis and SLE.15,32 MAS, bearing similar clinical presentation to hemophagocytic lymphohistiocytosis (HLH), is a life-threatening condition caused by overly activated lymphocytes and macrophages, triggering a cytokine storm. 15
Risk factors of CMV reactivation in AIIRDs patients
Several risk factors associated with CMV reactivation have been identified in AIIRDs patients. The main risk factor would be the use of immunosuppressants and high dose glucocorticoids.4,33
In a retrospective study by Ogata et al., 4 looking at 249 AIIRDs patients, prednisolone dose of ≥0.45 mg/kg/day increased the odds of having CMV antigenemia (odds ratio, 16.25). The median time from the start of immunosuppressive therapy to the onset of CMV antigenemia was 30 days (range of 21–44 days), and 85.7% developed CMV antigenemia within 60 days.
Similar onset of CMV reactivation was also reported by Sekiguchi et al., 34 The retrospective study demonstrated that the mean number of days from the treatment initiation to CMV reactivation in dermatomyositis patients was 6.1 ± 0.5 weeks (mean ± standard deviation). While in another retrospective study, Yamashita et al. 35 reported 14 (40%) out of 35 AIIRDs patients receiving prednisolone more than 0.5 mg/kg/day detected CMV antigen positivity within 33.7 ± 15.3 (12–66) days (relative risk = 4.5, 95% confidence interval = 1.14–17.6).
Hence, high daily dose of glucocorticoids ranging 0.45–0.5 mg/kg/day within the first 1-2 months of treatment initiation is an important predictor of CMV reactivation,4,34,35 and patients should be monitored for signs and symptoms of reactivation during this period and perhaps represents a critical window of opportunity for antiviral prophylaxis.
In general, both high daily and cumulative glucocorticoid dose play an important part in CMV reactivation and clinical disease. For instance, Xue et al. 20 reported that a higher prednisolone dose was administered to 73 SLE patients with CMV pneumonia with a median dose of 32 mg/day (range of 4–100 mg/day) as compared to 69 asymptomatic patients with a median dose of 20 mg/day (range of 1–50 mg/day). Additionally, they also discovered that the total prednisolone dose in the preceding 3 months was also higher in the CMV pneumonia group. The risk of CMV infection is generally reduced after reducing the glucocorticoids dose, with or without additional immunosuppressants.
Similarly, a retrospective study by Tsai et al. 36 demonstrated that the mean dose of prednisolone (25.9 mg/day) administered to SLE patients with CMV infection was higher than asymptomatic patients (9.0 mg/day). Other immunosuppressants were also more common in the symptomatic CMV disease patients as compared to asymptomatic patients (79% vs 58%, p < .010). 20
Other risk factors for CMV reactivation include lymphopenia (especially CD4+ T-cells),17,37 hypoalbuminemia,33,37 elevated creatinine, 33 prolonged hospitalization with consequent increased risk of co-infections, 28 old age,17,33 especially those above 60 years old, 17 and oral candidiasis.17,37 The prevalence of CMV reactivation has also been reported to be higher in certain diseases, including SLE patients, especially those with moderate to severe disease activity, ANCA-associated vasculitis (AAV), and myositis. 20 Meanwhile, high CMV viral loads can also increase the risk of CMV disease in AIIRDs patients, 33 with a higher probability of having symptomatic disease when CMV-DNA load is more than 1.75 × 104 copies/ml. 20
Overview of treatment and prevention strategy for CMV infection in AIIRDs patients
The antiviral treatment for CMV infection in AIIRDs patients varies based on several factors, such as the severity of CMV disease, rheumatic disease, and discretion of clinicians.28,38 The two most commonly administered antiviral drugs to these patients are intravenous ganciclovir20,28,29,33 and oral valganciclovir, which is the prodrug of ganciclovir.28,29,33 These drugs are also used as prophylaxis. The associated molecular mechanism of these antiviral drugs is to suppress CMV replication by inhibiting DNA polymerase. The duration of antiviral treatment varies among CMV infection in AIIRDs patients, depending on the severity of CMV infection and patient’s response to the treatment. Generally, an antiviral treatment is given for a minimum of 2 weeks and is ceased when serial serum viral load becomes undetectable. 39
In AIIRDs patients, two main approaches to mitigate the risk of CMV reactivation are primary antiviral prophylaxis and pre-emptive therapy. Primary antiviral prophylaxis can be considered to be used in high-risk asymptomatic CMV IgG positive patients undergoing immunosuppressive therapy, which is in a similar manner used in hematopoietic stem cells and solid organ transplantation patients to prevent its reactivation and clinical disease.20,40 It can also be considered in high-risk seronegative patients undergoing immunosuppression to prevent them from contracting CMV. On the other hand, pre-emptive therapy is an alternative strategy that involves monitoring serial viral loads during immunosuppressive therapy, ensuring that the viral load is below detection rate and initiating antiviral treatment only when viral loads reach a predetermined threshold to prevent the onset of symptomatic CMV disease. 40 While primary prophylaxis may lower CMV disease incidence, it has been associated with increased antiviral drug-related toxicity, late-onset CMV disease, increased risk of drug resistance, and higher treatment cost as compared pre-emptive therapy. 41 To date, there is a lack of consensus with regards to antiviral prophylaxis in AIIRDs patients. 42
Conversely, the goal of secondary prophylaxis is to prevent further development of CMV disease, reactivated or recurrent CMV infection in patients who have already been infected with CMV. 43 Therefore, secondary prophylaxis is usually administered during ongoing immunosuppressive therapy in patients with a history of CMV reactivation or disease, which puts them at a high risk of developing life-threatening CMV disease complications, although the exact duration of secondary prophylaxis remains uncertain. 43 Apart from the commonly used intravenous or oral ganciclovir and oral valganciclovir, randomized trials in renal transplant patients demonstrated comparable efficacy of valacyclovir (2gm four times daily) for CMV prophylaxis.44–46 In another randomized controlled trial involving CMV seropositive patients with AAV, the use of valacyclovir prophylaxis for 6 months, suppressed subclinical CMV reactivation. 47 Kervan et al. 48 reported an alternative low dose valacyclovir prophylaxis of 1000 mg/day for 6 months in 68 orthotopic heart transplant patients on triple immunosuppressive therapy (i.e., ciclosporin, steroids, and mycophenolate mofetil). Only one CMV infection was noted during follow up at 17 months, suggesting that a lower dose regime may be feasible in resource limited setting.
In a retrospective study by Lim et al., 34 patients with glomerulonephritis and renal vasculitis undergoing immunosuppressive therapy were stratified according to the risk factors for CMV reactivation. 49 High-risk patients were defined as CMV seropositive patients with 3 or more risk factors: renal impairment with eGFR <15 mL/min/1.73 m2, use of methylprednisolone, cyclophosphamide, mycophenolate mofetil, rituximab or plasma exchange therapy. Among the 21 high-risk patients identified, 9 received antiviral prophylaxis and did not develop CMV disease during the 6 months of surveillance, while 1 patient developed CMV disease in the non-prophylaxis group (0% versus 1(8.3%), p = 1.00).
In a similar study by Tan et al., looking at a cohort of 119 glomerulonephritis patients including 49 patients with lupus nephritis and 19 with renal vasculitis, 28 patients were deemed to be at high risk for CMV reactivation (with 3 or more risk factors as defined by Lim et al. 49 ). 50 Among the 28 patients, 7 patients who received antiviral prophylaxis did not develop CMV disease while 3 patients developed CMV disease in the non-prophylaxis group (0% versus 3 (14.3%), p = .55).
Preventative strategies for CMV have also been considered in SLE patients with pulmonary hemorrhage, which has a high prevalence of CMV reactivation contributing to mortality 51 and MDA5 dermatomyositis patients who have a higher risk of CMV infection as compared to other types of inflammatory myopathies. 52 Furthermore, MDA5 dermatomyositis patients undergoing intensive immunosuppressive therapy have a significant risk for CMV reactivation ranging from 85% 53 to 100%. 54 Tseng et al. 55 reported improved 1 year survival in MDA5 dermatomyositis patients on tofacitinib who were also given valganciclovir (p = .003) as primary CMV prophylaxis as compared to those who were not given prophylaxis. Tsuji et al. 53 employed pre-emptive therapy by monitoring serial CMV antigenemia in MDA5 dermatomyositis patients receiving combination therapy of glucocorticoids, cyclophosphamide, ciclosporin, and early antiviral drugs if patients were positive for CMV antigenemia.
To date, there is no published guidelines on the use of prophylaxis to prevent CMV infection in AIIRDs patients due to the lack of robust data.56,57 Ergo, the decision to use primary or secondary prophylaxis is at the discretion of clinicians based on individual patient’s profile. 56
The duration of prophylaxis varies according to the patient’s CMV viral load, risk factors, length of intensive immunosuppression, and type of antiviral drug administered. 19 As various induction immunosuppressive regimes tend to span from 3 to 6 months representing the peak period of immunosuppression, perhaps a minimum duration of 3–6 months of antiviral prophylaxis would seem a reasonable approach taking into account patient profile, cost, and tolerability. Additionally, prophylaxis should be initiated instantly to achieve optimal prophylactic effect and reduce the risk of CMV disease. 20 Nevertheless, there is no guidelines or studies on the optimum duration of antiviral prophylaxis.
Given the clinical significance of CMV reactivation in AIIRDs patients contributing to morbidity and mortality, one possible strategy would be to perform baseline CMV screening in patients planned for immunosuppressive therapy to stratify their risk of developing CMV disease. Determination of CMV IgG seropositivity as an initial step can help to identify patients with potential risk of reactivation (20,35). Serial CMV viral load monitoring during immunosuppressive therapy can also be used to guide antiviral prophylaxis therapy (20,35).
Common techniques used to monitor CMV viral load are antigenemia and quantitative nucleic acid amplification (QNAT) testing, namely real time-polymerase chain reaction (RT-PCR) test. 58 The antigenemia test is an immunofluorescence assay based on the detection of CMV viral antigen, such as phosphoprotein 65 (pp65), in the peripheral blood leukocytes using monoclonal antibodies. 59 Although this test is relatively easy to perform and does not require expensive equipment, it is labor intensive, requires immediate sample processing, and inconsistent in terms of assay protocol and result interpretation. 41 In contrast, RT-PCR, the gold standard of CMV detection, has a quicker turnaround time and higher throughput and accuracy, despite requiring expensive equipment and reagents. 41 RT-PCR quantifies CMV DNA levels in whole blood or plasma by amplifying viral DNA found in the specimen using PCR method and fluorescence. 60
Another emerging technique to stratify risk of CMV reactivation is by measuring the adequacy of CMV-specific T-cell immunity in individuals. 11 A positive test result suggests that the patient has adequate CMV-specific-T-cells to fight off CMV infection, while a negative result implies low CMV immunity with a consequent higher risk of reactivation. In a prospective study by Bruminhent et al., 55 active SLE patients were monitored for clinically significant CMV infection (defined as plasma CMV DNA loads >3 log10 IU/mL) before and after intensive immunosuppression therapy. 61 CMV-specific T-cell immunity was determined using QuantiFERON-CMV assay. At 1-month post-immunosuppression, CMV infection was higher in QuantiFERON negative patients compared to QuantiFERON positive patients (44.4% vs 11.8%; p = .03; adjusted hazard ratio, 4.97; 95% CI, 1.07–23.10; p = .04). Hence, antiviral prophylaxis can be considered in patients who lack CMV-specific-T-cells. 62 This can also be beneficial in determining the duration of secondary prophylaxis following CMV disease, where antiviral prophylaxis can potentially be continued until the return of adequate CMV-specific-T cells. This strategy has an advantage by avoiding universal prophylaxis for all patients and instead selecting only high-risk patients for therapy, thus avoiding drug adverse events, risk of drug resistance, and financial burden.11,40
The tests developed for measuring CMV-specific T-cell immunity include QuantiFERON-CMV assay,63,64 CMV-(enzyme-linked immunospot) ELISPOT assay, 62 and CMV T-Cell Immunity Panel (CMV-TCIP). 11 The QuantiFERON-CMV assay, a commercially available predictive test for CMV, works on the principle of enzyme-linked immunosorbent assay (ELISA)-based type II interferon (IFN-γ) release assay, which detects the level of CMV-specific CD8 + cells following multiple peptide stimulations.41,65,66 This assay was proven to be predictive of CMV immunity in solid-organ transplant patients and aids in serostatus-based risk stratification. 67 The predictive values of this assay were 0.90 (95% CI, 0.74–0.98) for positive results and 0.27 (95% CI, 0.18–0.37) for negative results. However, some studies have shown that QuantiFERON-CMV has limited incremental predictive value and require further development.64,68 The CMV-ELISPOT assay, which is also an IFN-γ release assay, measures the immune activity of CMV-specific CD4+ and CD8 + T cells in the blood specimen through the release of cytokines when stimulated with CMV-specific antigens like pp65 or immediate early 1 (IE-1). 63 The CMV-ELISPOT assay performed comparatively well in predicting CMV infection in renal and kidney transplant recipients in contrast to QuantiFERON-CMV assay.63,68 Similar to the CMV-ELISPOT assay, the CMV-TCIP assay can measure both CMV-specific CD4+ and CD8 + T-cell responses toward CMV separately after stimulation of blood specimens with CMV-specific peptides and lysates. 11 However, CMV-TCIP should not be used as a sole indicator to start or discontinue prophylaxis, and it is important to consider patient’s individual conditions when monitoring patients for CMV. 69 There is also a possibility of getting different diagnostic outcomes due to the variations in target peptides. 65 For instance, QuantiFERON-CMV assay detects CD8 + T cells through multiple peptide stimulations while CMV-ELISPOT assay detects CD4+ and CD8 + T cells through the stimulations of viral proteins. Moreover, although these tests are able to predict viremia, their ability to predict CMV disease is yet to be established. 63 These novel tests require further validation, especially in clinical settings involving AIIRDs patients, as most of the outcomes of these tests were observed in transplant recipients.
Conclusion
There is a high prevalence of CMV in AIIRDs patients, especially in those undergoing immunosuppressive therapy, with potential risk of developing tissue invasive and life-threatening CMV-related diseases. At the present moment, no standardized recommendation can be made with regards to antiviral prophylaxis in AIIRDs patients. However, in high-risk patients, antiviral prophylaxis should be considered to subdue virus replication after considering the risk of drug-related toxicity, resistance, and higher treatment cost. It is also important to continuously monitor for CMV reactivation and disease in such patients and initiate early antivirals based on predetermined viral load threshold. Secondary antiviral prophylaxis should also be considered following CMV-related diseases until the patient’s immune system status, in particular T-cell mediated immunity, is at a satisfactory level. Presently, there is an emerging technique that measures CMV-specific T-cell immunity which can reflect patients’ ability to fight off CMV, allowing clinicians to selectively administer prophylaxis to patients who require medication to control CMV viral loads. While this novel laboratory test requires further validation and cannot be used as a sole indicator to start or discontinue prophylaxis, it is one step closer to lessening CMV-related morbidity and mortality in AIIRDs patients.
Footnotes
Author contributions
BB was the lead author involved in drafting of the manuscript and literature review. AM was involved in the article conceptualization and writing of the manuscript. WYS was involved in the concept, design, editing of the manuscript. All authors reviewed and approved the final version of the manuscript .
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets generated and/or analysed during the current study are available from the corresponding author.