
Abstract
Positive health (PH) offers a broader perspective on well-being, emphasizing the ability to self-manage social, physical, and emotional challenges. This study explores PH among cardiac patients by assessing their self-perceived health, personal goals, and what is needed to achieve these goals, aiming to guide healthcare improvements from a holistic perspective. A qualitative, phenomenological study was conducted with 10 Dutch-speaking cardiac patients at the Medisch Spectrum Twente cardiology outpatient clinic. Participants completed the My Positive Health tool online, followed by a semistructured interview conducted at the clinic. Thematic analysis revealed that participants rated their health as moderate. Participants reported physical limitations (fatigue and shortness of breath) and mental challenges (anxiety and difficulty accepting). Personal goals included improving physical health, reducing anxiety, enhancing daily functioning, and adopting healthier lifestyles. Participants identified professional support, self-care, tools (eg, diet apps and planners), and changes in medical practices as critical factors needed to achieve their goals. Cardiac patients face multidimensional challenges beyond physical symptoms. A personalized, holistic healthcare approach aligned with the PH concept can better address these needs, improving well-being and reducing disease burden.
Introduction
Healthcare systems worldwide face rising demands and costs, driven in part by an aging population and the growing prevalence of chronic conditions like cardiovascular diseases (CVDs).1–3 CVD remains a leading cause of mortality and disease burden worldwide. 4 In the Netherlands, where this study is conducted, CVD accounts for a significant proportion of hospital admissions. 5 This study focuses on the cardiac conditions of CVDs, like coronary artery disease, heart failure, myocardial infarction, and arrhythmias. The number of patients with cardiac diseases is expected to rise. 6 These conditions interact with physical, psychosocial, and lifestyle factors, which makes the broader perspective of positive health (PH) on well-being highly relevant in this context. For example, unhealthy lifestyles, along with conditions such as hypertension, obesity, and comorbidities like chronic obstructive pulmonary disease and diabetes, increase the likelihood of developing or worsening cardiovascular conditions. 7 In addition to the physical burden of CVD, mental health issues are prevalent, often exacerbating the condition and increasing hospital readmissions. 8 , 9
Despite this, healthcare systems have traditionally focused on diagnosis and treatment rather than prevention, health promotion, and well-being,10–13 calling for a shift to a more holistic approach. The concept of PH, developed by Huber et al, 14 can be utilized to understand and enhance a person's health and well-being. It is described as “the ability to adapt and self-manage in the face of social, physical, and emotional challenges.” PH encompasses 6 dimensions: bodily functions, mental well-being, quality of life, participation, daily functioning, and meaningfulness. The dialogue tool, My Positive Health (MPH tool), provides insights into how individuals perceive their health and set personal goals. 14 , 15
To the best of our knowledge, no studies have examined PH among cardiac patients. Existing research often focuses on particular aspects, such as self-perceived mental attitudes toward cardiac disease. 16 Currently, little is known about the self-perceived health of cardiac patients. This study aims to explore how cardiac patients experience PH, their personal goals, and what is needed to achieve them, with the goal of guiding healthcare to better align with patients’ needs from a holistic health perspective, improving well-being and reducing disease burden.
Method
Study Design and Setting
A phenomenological qualitative study was conducted to explore the lived experiences and perceptions of cardiac patients regarding their health and well-being, which was investigated through semistructured interviews held between April and May 2023 at the cardiology outpatient clinic of Medisch Spectrum Twente (MST), a tertiary hospital in the Netherlands.
Participants
The participants were 10 Dutch-speaking cardiac patients who were undergoing cardiac treatment at MST. The following inclusion criteria were applied: patients diagnosed with a cardiovascular condition, patients currently or previously treated at the cardiology outpatient clinic of MST, and patients over 18 years of age.
Data Collection
Participants were recruited through convenience sampling by physicians or nurses. After informed consent, they completed the MPH tool online before the interview, assessing health across 6 dimensions: bodily functions, mental well-being, quality of life, participation, daily functioning, and meaningfulness. The 44-item tool uses an 11-point Likert scale (0 = completely disagree; 10 = completely agree) with results visualized in a spiderweb diagram. 15 , 17 , 18 Interviews were conducted face-to-face at MST by a Health Sciences bachelor's student. The results, including the MPH spiderweb scores across the PH dimensions, were used to guide the discussion. Each interview lasted 45 to 60 min, and was audio-recorded, transcribed, and anonymized.
Data Analysis
Thematic analysis was employed, following established steps. 19 Initial phases involved reading transcripts and preliminary coding. Two researchers independently (MHG and IB) coded 2 interviews. The codes between the coders largely aligned, but were sometimes expressed in different terms, for which overarching terms were created. The coding was performed manually using the Word program. A codebook was created, categorizing codes into themes and subthemes, with MHG coding the remaining interviews and updating the codebook with the support of IB. Final themes were reviewed for coherence with the dataset, in collaboration with SHK and MHV. All interviews were recorded using the final codebook, and participant results were organized in a matrix following the Framework Method. 19 The SRQR guideline was followed for reporting this research. 20
Results
Ten participants, aged 34 to 66 years (median age 60.5), were predominantly male (n = 8), as shown in Table 1. Participants’ cardiac conditions were informally shared during interviews without systematic data collection or official diagnoses. Obviously, interviews revealed various cardiac conditions, including myocardial infarctions, cardiac arrests, blocked arteries, myocarditis, and arrhythmias. Eight participants mentioned having undergone surgical procedures.
Participant Characteristics.

Self-Perceived Health
Most participants rated their self-perceived health as moderate. Many noted the significant impact of cardiac disease on their self-perceived health.
Bodily Functions
While a few participants expressed partial satisfaction with their bodily functions, nearly all participants reported experiencing physical complaints due to cardiac problems. Commonly mentioned issues include reduced physical condition, fatigue, palpitations, and shortness of breath: “I have very little physical condition, I try to move as much as possible, but I get tired quickly” (P5). A few participants experienced pain, either from recent cardiac surgery or comorbid conditions. Almost all participants reported fatigue and some experienced sleep problems caused by shortness of breath. Physical complaints are limiting in daily activities: “I am unable to perform certain tasks without becoming fatigued” (P9).
Mental Well-Being
Mental health was a key theme in nearly all interviews. Anxiety was the most common challenge, often linked to fear of death or worsened by symptoms like shortness of breath. Sleep problems were frequently caused or intensified by anxiety: “I’m afraid I might die at night” (P2). Several participants also struggled to adjust to illness-related limitations and increased dependence, leading to feelings of guilt or uselessness: “I don’t want to accept that I have to rely on others … or that I’m dependent on a pacemaker” (P5). A few mentioned memory and concentration issues, though these were not seen as major obstacles. Despite these challenges, most participants remained generally positive about their mood and zest for life.
Lifestyle
Nearly all participants mentioned difficulties in maintaining a healthy lifestyle, particularly when it came to diet and physical activity. Fatigue and shortness of breath were major barriers to healthy habits: “Often, I’m so tired that I have no energy to eat and end up skipping meals” (P5). Anxiety also played a limiting role, especially in regaining the confidence to be physically active and to place more strain on the heart.
Daily Functioning
Many participants experienced limitations in daily functioning due to their cardiac condition. Several had to stop or reduce work and leisure activities: “I had to stop my business due to my cardiac problems” (P3). Some pushed their limits to maintain pleasure and autonomy, sometimes leading to serious consequences: “I pushed my limits too far, which led to arrhythmias and a hospital admission” (P5). Others learned to set boundaries, often accompanied by greater acceptance, enabling them to continue activities with adjustments. Support from loved ones was, and continues to be, essential in coping with daily challenges. Participants were satisfied with their personal situation (financial and housing).
Meaningfulness
Several participants noted a positive change in their outlook on life despite the challenges posed by cardiac disease. They have developed a more positive attitude and express gratitude: “After my cardiac surgery, I find more joy in the small things” (P8). Some expressed gratitude particularly for still being alive.
Medical Practices
Participants appreciated the positive impact of medical care, including support from motivating physicians and cardiac rehabilitation for both physical and mental recovery. Many also expressed gratitude for treatments and surgeries. However, nearly all noted shortcomings in medical practices, particularly the overwhelming nature of being a heart patient, especially with acute conditions. A common issue was the lack of clear, accessible information about symptoms and when to seek help: “At first, I linked every symptom to my heart and felt scared, not knowing some were normal” (P6). Additionally, some participants, especially those with anxiety, felt a lack of reassurance and support. They mentioned follow-up appointments being too spaced out and that mental health issues and sleep problems were sometimes overlooked: “I sometimes call the hospital when I suddenly feel short of breath because I’m scared. They tell me it's normal, but that doesn’t provide enough reassurance” (P3). A few also highlighted delays in starting cardiac rehabilitation and unpleasant medication side effects.
Personal Goals
Participants discussed personal goals for improving their self-perceived health, which are outlined in Table 2.
Participants Personal Goals.
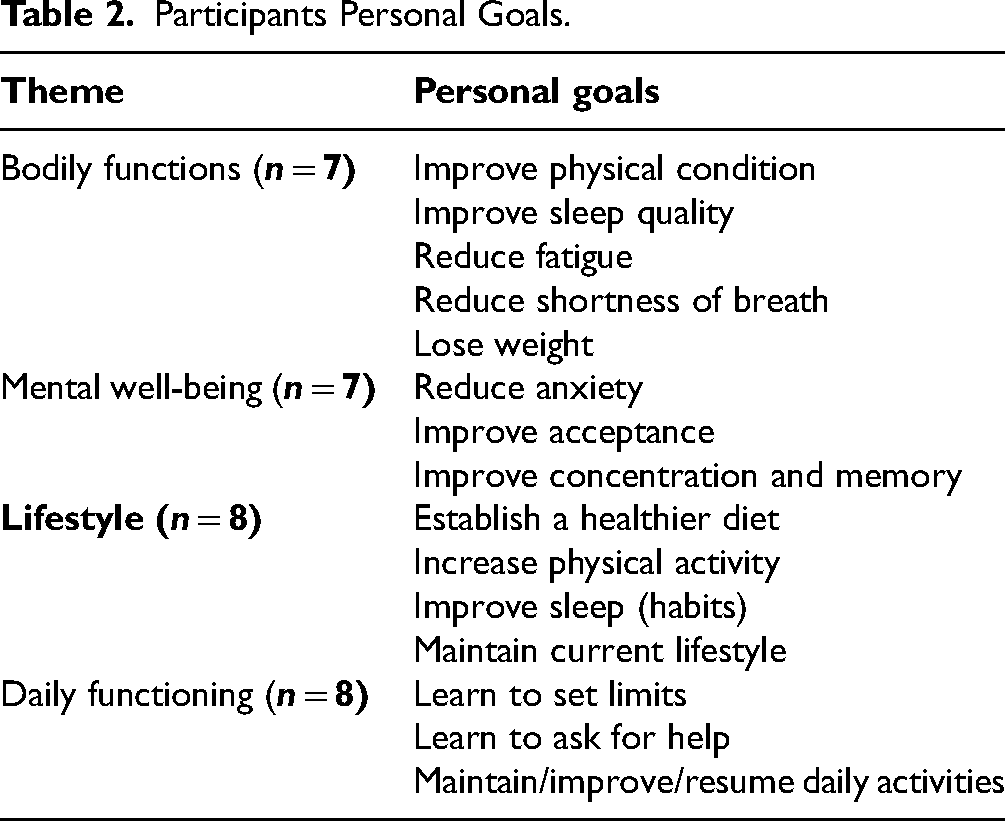
Bodily Functions and Mental Well-Being
Many participants aimed to enhance their physical condition and sleep quality. The majority sought to reduce anxiety, while a smaller group aimed to improve acceptance. A few wanted to improve their memory and concentration. These goals were interconnected: reducing anxiety can increase motivation for physical activity, and increased physical activity, in turn, improves physical condition. Conversely, more physical activity can boost confidence and reduce anxiety. A participant mentioned: “I want to improve my physical condition so I can walk short distances without shortness of breath. To feel better, I also need to accept my limitations and sleep without the fear of dying” (P3).
Lifestyle
Almost all participants expressed a personal goal for a healthier lifestyle to improve their overall health, focusing on improved exercise habits, dietary patterns, and sleep routines. Some mentioned the importance of daily structure as a stabilizing factor for both mental and physical health: “I want to improve my lifestyle by cycling and walking more and adding more structure to my meals and sleep” (P4).
Daily Functioning
Improving or maintaining daily functioning was a significant goal for nearly all participants. They emphasized the value of work, hobbies, and social activities for their overall well-being and quality of life. Importantly, these functional goals were often grounded in earlier-mentioned personal goals such as improving physical condition and reducing anxiety. Additionally, participants aimed to learn to ask for help and accept help, as well as to manage their physical limits, and mental challenges and to improve daily functioning: “The most important thing I want to learn is to accept and manage my physical limitations and set boundaries. Then I will feel much healthier” (P5).
What Is Needed to Achieve Personal Goals?
Participants identified key needs are shown in Table 3.
Participants Need for Achieving Personal Goals.

Professional Support
Over half of the participants expressed a need for professional support. They hope to address issues such as anxiety, acceptance, and management of their limits with the help of a psychologist: “Talking to a professional is different from talking to friends” (P1). Several participants expressed the need for help from a dietitian. A few participants mentioned needing physical therapy for exercise and confidence, while most had received or were receiving it as part of cardiac rehabilitation.
Tools
Some participants expressed interest in tools, including diet management apps, planners for memory aid, treadmills for exercise, and meditation and music to improve sleep.
Support From Others
Nearly all participants emphasized again the importance of maintaining or expanding support from others in achieving their personal goals. Continued communication with loved ones is crucial for mental support, and a strong bond with them aids in the recovery and acceptance process. Participants also expressed a need for more practical support, particularly in terms of doing activities together, such as cooking and exercising: “I find it helpful to have someone walk with me. It gives me a sense of safety” (P10). Additionally, some participants expressed the need to connect with other cardiac patients who have similar experiences.
Self-Care and Lifestyle
Almost all participants highlighted that taking good care of oneself and maintaining personal responsibility are crucial for achieving their personal goals. Especially in lifestyle. Many expressed the goal to take the responsibility for staying active: “I want to keep exercising once a week because I feel much healthier then” (P4). Regular walking was frequently mentioned, as was the responsibility to eat healthily and maintain good sleep habits. Also, as part of self-care half of the participants plan to manage their physical limits by dosing their activities, incorporating rest moments, and setting realistic goals for themselves.
Changes in Medical Practices
Almost all participants felt that changes in medical practices would support their personal goals. Over half expressed a need for a more personalized or holistic approach, such as addressing anxiety or customizing medication. There was also a strong demand for better information and education on cardiac disease, surgery, symptoms, and lifestyle, with some suggesting designated contact persons within the hospital or reliable resources. Participants favored more frequent follow-ups: “I would prefer to have appointments every three months instead of every six months. It provides more reassurance and control” (P6). They also emphasized the need for timely referral to cardiac rehabilitation, suggesting the implementation of automatic referrals.
Discussion
This study examined self-perceived health using the concept of PH, personal goals, and the needs of cardiac patients. Most participants rated their health as moderate, citing physical and mental complaints like reduced physical condition, fatigue, shortness of breath, anxiety, and difficulties with acceptance. Cardiac-related symptoms can significantly impair daily functioning, 21 , 22 a finding echoed by participants who reported limitations in daily activities and feelings of uselessness. Participants expressed a big challenge with anxiety, which can be classified as a stress factor. Both in this study and in the literature, sleep problems were common among cardiac patients, with anxiety being the leading cause. 23 Poor sleep, can negatively affect recovery and rehabilitation outcomes. 24 Participants emerged fatigue and anxiety as the most frequently mentioned barriers to maintaining a healthy lifestyle. This aligns with existing evidence linking fatigue to reduced self-care in heart failure patients 25 and showing that mental health issues can hinder lifestyle adherence. 26 Many participants struggled with accepting the consequences of their cardiac condition. A low level of illness acceptance is known to negatively impact quality of life, particularly in chronic cardiac diseases. 27 While depression and posttraumatic stress are common in this population, 28 , 29 depression was not observed in this study—possibly due to participants’ generally positive outlook, satisfaction with their social environment, or limitations in study design. Although participants generally reported strong social support, it is well established that inadequate support can adversely affect health outcomes. 30 Participants emphasized the importance of ongoing support—both emotional and practical. Social determinants such as access to transport, healthy food, and community resources were not major concerns in this study, likely due to the well-developed facilities in the Netherlands and participants’ general satisfaction with their personal circumstances, including finances and housing. To the best of our knowledge, no studies have examined the personal goals of cardiac patients in relation to PH. In this study, patients’ goals focused on reducing physical and mental symptoms, improving lifestyle, and maintaining daily functioning. Personal goals were interconnected. For many, the observed pattern was that the desire to reduce anxiety contributed to better sleep, which decreased fatigue and provided more energy to adopt a healthier lifestyle. Most participants preferred a more personalized, holistic medical approach, suggesting more frequent follow-ups and better information to reduce anxiety and improve acceptance. Professional support, especially from psychologists and dietitians, was seen as instrumental to achieving personal goals. Participants were familiar with physiotherapy. Tools like mobile apps could offer practical support. To ultimately achieve their goals, participants emphasized the importance of maintaining support from others and improving personal responsibility, including being open to accepting help and recognizing physical limits. Interviews revealed a diverse range of cardiac conditions. A notable finding was that nearly all participants reported experiencing anxiety and limitations in daily functioning. This suggests that a holistic and personalized approach is desirable for all cardiac patients. Addressing not only physical symptoms but also mental health, lifestyle, and daily functioning can lead to improved overall well-being. Evidence indicates that psychological interventions are beneficial for successful lifestyle changes among cardiac patients. 31 It is recommended that mental health issues be assessed during hospital admission following a cardiac event to prevent adverse outcomes. 32 These findings and the needs expressed in this study call for a shift in healthcare practices. More preventive and holistic care could potentially reduce costs and unnecessary healthcare services. Growing evidence supports tailored care approaches like patient-centered care, shared decision-making, and holistic nursing.22,33–35 This study and evidence have shown the concept of PH aligns with this approach. 36
Limitations
A limitation of this study is the narrow demographic profile, with mostly male participants over 50. While this reflects the higher CVD prevalence in older men in the Netherlands, 37 it limits generalizability to other groups. The lack of detailed socioeconomic data and specific information on participants’ cardiac conditions (eg, type and duration) further restricts applicability. This made it difficult to tailor personal goals to subgroups. At the same time, it underlines the need for a holistic approach for all individuals, regardless of their specific diagnosis.
Conclusion
The impact of cardiac disease on patients is significant and affects physical and psychosocial aspects. On average, cardiac patients perceive their health as moderate. In addition to physical symptoms, they experience issues with mental well-being and feel restricted in their lifestyle and daily functioning, with these factors mutually reinforcing each other. Cardiac patients have multifaceted personal goals and needs that requires a transition towards a holistic approach in healthcare. The concept of PH appears to be well-suited for addressing these needs.
Footnotes
Acknowledgments
We would like to thank the student for assisting with data collection and all participants in the study.
Authors’ Contributions
The researchers (MHV) and (SHK) were responsible for the overall management and execution of the research. The researchers SHK and MHV performed the final coding. All authors have given final approval for this article to be published and agreed to be accountable for all aspects.
Declaration of Conflicting of Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors (MHG, MHV, IB, and SKH), including the interviewees, were not involved in the development of the conceptual model of Positive Health and declared they have no conflict of interest.
Funding
This research received no specific grant from any funding agency. It is part of the L.INT lectorate Positive Health, which is partially funded by the Taskforce for Applied Research SIA.
Ethical Approval
Ethical approval to report this case was obtained from the Institutional Review Board of MST (protocol number K22-25).
ORCID iDs
Statement of Human and Animal Rights
All procedures performed in this study involving human participants were in accordance with the ethical standards of the Institutional Review Board of MST and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards (protocol number K22-25).
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.