
Abstract
Cardiovascular disease (CVD) is the leading cause of maternal mortality in the United States. Two major hospital networks implemented a novel CVD risk assessment of pregnant and postpartum patients to standardize identification of patients with previously unknown CVD or at risk to develop CVD. This qualitative study explored the experience of being identified as at CVD risk in a purposive sample of 10 obstetric patients. Participants varied by age, race/ethnicity, language (English/Spanish), and comorbidities. Interviews focused on patients’ awareness, emotional responses, clinician-patient communication, and behavioral intentions. Thematic analysis using Atlas.ti 8 revealed a limited understanding of the association between CVD and pregnancy complications and lifetime CVD risk. Positive risk assessments triggered surprise and concern. Overall, patients evaluated the clinician-patient communication positively but found information too cursory and varied in strategies to find out more details. Several patients initiated immediate lifestyle changes, while others waited for guidance from clinicians. The study underscores the need to engage patients in the implementation of screening tests and to improve health literacy to facilitate follow up care and behavior change.
Plain Language Summary
Cardiovascular disease (CVD), or heart disease, is the main cause of death during pregnancy and after childbirth in the United States. Pregnancy is a stress test on the heart similar to being on a treadmill for nine months and hence heart disease is more likely to develop. As symptoms for heart disease can be confused with pregnancy symptoms, a standardized CVD risk assessment may help to identify pregnant and postpartum patients at risk of developing CVD. With this study, we aimed to explore pregnant and postpartum women's reactions to a positive risk assessment for CVD. We interviewed ten women who had been identified as risk-positive for CVD using a new risk assessment tool at two hospitals in California and New York. Women participated in online interviews, where we asked them about their awareness of CVD risk, how they reacted emotionally, their communication with doctors, and any changes in their health behavior. Our study found that most respondents did not know pregnancy could increase their risk for heart disease. Many respondents were surprised or concerned when they learned they were at high risk. Most respondents appreciated being monitored by their doctors frequently but they wanted more information and education about their condition. While some respondents immediately implemented changes in diet, physical activity, and self-care, others waited for guidance from their clinician. The study highlights that better communication and resources on heart health during pregnancy and postpartum can improve heart health and avoid problems throughout the life course. This research informs clinicians how to communicate with their patients about CVD risk and what additional resources would be helpful for patients.
Keywords
Introduction
Cardiovascular disease (CVD) is the leading cause of maternal death in the United States, 1 and will increase due to advanced maternal age and the growing number of CVD risk factors such as high blood pressure, obesity, and diabetes among reproductive-age women. 2 CVD remains the leading cause of morbidity and mortality for women throughout their lifetime with over 40% of women over the age of 20 years having some form of CVD.1,3
The increased amount of blood a heart needs to pump during pregnancy can lead to new or worsening heart problems in otherwise healthy birthing people. Furthermore, timely diagnosis of developing or previously undiagnosed CVD is often delayed or missed, because pregnancy may lead to signs and symptoms that are very similar to those of CVD. 4 Implementing standardized CVD risk assessments during the prenatal and postpartum periods may provide a key opportunity to improve identification and follow up of early symptoms and timely diagnosis. 5 Two major hospital networks implemented a standardized risk assessment to identify pregnant and postpartum patients with previously unknown CVD or at risk of CVD. 6
The effective implementation of the tool relies on patient engagement and health literacy as major drivers in quality care and health maintenance7-9 which states that personal health literacy is “the degree to which individuals have the ability to find, understand, and use information and services to inform health-related decisions and actions for themselves and others.” This approach respects an individual's decision on whether and when to modify risk behaviors and strives for patients’ self-advocacy as a goal. 8 Pregnant patients undergo a variety of screening tests during their prenatal care and after delivery but there was no information on how pregnant and postpartum patients would process information about being at risk for CVD. 10 Systematic reviews highlighted the limited research on patient knowledge of long-term CVD risks, such as hypertension and heart disease, among women who have experienced pregnancy complications like hypertensive disorders of pregnancy (HDP) and gestational diabetes (GDM).11,12 While some educational interventions showed slight improvements in women's awareness of CVD risks, many of the studies had small or non-significant findings, and there was no clear consensus on the best clinical tools for educating patients. This review also identified challenges in measuring knowledge and awareness of CVD risk due to varying patient health literacy and differences in assessment methods. 12 Patient counseling on CVD risk has not been standardized and a study on CVD risk counseling in the postpartum setting found a wide variability in the form of how clinicians talk to their patients about their CVD risk. 13
It has not been assessed how obstetric patients experience the notice that they may be at risk for CVD during a time where they at heightened awareness about their health and potential implications for their and their infant's health. It is also unknown whether patients distinguish and respond to the difference between “being at risk for CVD” and “having a CVD diagnosis after additional follow up tests” during a time where they at heightened awareness about their health and potential implications for their and their infant's health.
This study aimed to obtain insights on how pregnant and postpartum patients understand and react to being identified to be at risk for CVD. Our research questions explored patients’ knowledge about CVD risk during pregnancy and postpartum, their perception of the clinician communication about CVD risk, their emotional reaction and information need, and any intent to change behavioral risk factors such as diet or exercise now or after their pregnancy. These findings will inform how the clinician-patient communication about CVD risk should be framed and the type of health promotion that best complements the clinic encounter.
Methods
This was a qualitative study using participant interviews at two hospital networks in California and New York. Combined, they provide obstetric services at 23 sites ranging from hospital inpatient and outpatient clinics to community health centers and affiliated private medical offices. The CVD risk assessment tool was embedded into the electronic health record system. The risk assessment occurred at the first obstetric interaction at outpatient prenatal clinics, on labor and delivery, triage, antepartum and postpartum units. The risk assessment algorithm calculates a score based on symptoms, vital signs, demographic factors and comorbidities that determines whether patients should be referred for further testing such as EKG, echocardiogram and consultation with a cardiologist. This study was approved by the Institutional Review Board of the University of California, Irvine. Between July 2021 to December 2022, we identified 254 patients who had a positive CVD risk assessment.
We recruited a purposive sample of 10 patients. Patients were selected to represent different clinics (high risk, general obstetric, family medicine), age groups, race/ethnicity, preferred language, and presence or absence of comorbidities. We anticipated that with ten participants we would capture the diversity of experiences and perspectives related to CVD risk assessment, making a smaller sample size sufficient to reach saturation.
The clinician informed eligible patients about the study; if they agreed to be contacted, a member of the research team obtained verbal consent and conducted a zoom 30–40 min zoom interview. Interviews were audio-recorded and transcribed. Spanish interview transcripts were translated into English for analysis by a member of the research team. None of the interviewers provided clinical care to the participants. Interviewees received a $25 gift certificate.
The interviews were conducted by a female public health PhD scientist with extensive qualitative research experience who trained and guided a female maternal fetal medicine MD fellow, and a male master's in public health MPH intern. Two interviewers were bilingual in English and Spanish.
The research team developed an open-ended interview outline, based on the Health Belief model (HBM) and our research questions. According to the HBM, individuals with accurate knowledge of CVD and perceived susceptibility to and consequences of the disease, and awareness of the benefits of taking preventive measures, were more likely to make important lifestyle choices to prevent the disease's onset. 14 The interview outline was reviewed by a Technical Expert Panel that was comprised of Maternal Fetal Medicine specialists, cardiologists, social scientists, and patient representatives. The final version consisted of 21 open-ended questions (Supplemental Information). Participants were asked about their age, country of birth, primary language, insurance coverage, and race and ethnicity. The interview explored the following themes: (a) cardiovascular disease risk knowledge/awareness, (b) reactions to screening results, (c) effects on attitudes, beliefs, and intentions and (d) barriers to change, perceived Control. Emerging themes were added to the interview guide throughout the data collection process. Two members from the research team independently (KG, HTB) read and coded the interview transcripts, using ATLAS.ti v.8 software (Scientific Software Development GmbH, Berlin, Germany). Throughout the coding process, the team met regularly to ensure consistency and resolve any disagreements.15-17 This process allowed for synthesis of multiple researcher perspectives (clinical, public health) to gain a better understanding of the data. The research team (KG, DW, AH, HTB) discussed and sorted codes into broader themes through an iterative process. Relationships among themes were reported in our findings (Figure 1).

Relationships among identified themes.
Results
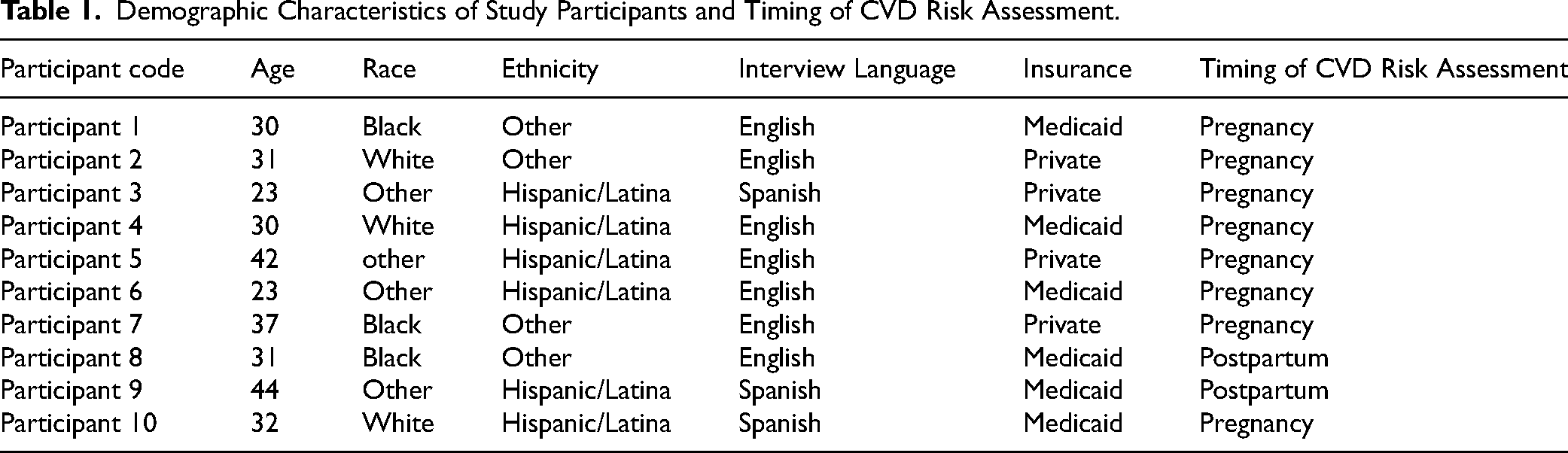
Of the ten patients selected and consented for the study, seven participants had the risk assessment during the pregnancy and three during the postpartum period [See Table 1] Age of interviewees ranged from 23 to 44, three participants identified as Black and six identified as Hispanic. All participants reported they receive regular prenatal care during their pregnancies.
Demographic Characteristics of Study Participants and Timing of CVD Risk Assessment.
Major Themes
CVD Risk During Pregnancy and Implications for Cardiovascular Health After Delivery are not Well Understood
Participants reported awareness of cardiovascular disease and its severity which was especially the case for participants who had a family history of CVD. However, among most participants, CVD was seen as a disease that occurs in an older individual and mainly in men. One participant remarked, “I didn’t know CVD was something that pregnant women would be at risk of.” (Participant 2). [See Table 2] While some participants were aware of CVD risk factors, they mostly associated them with general lifestyle choices, not pregnancy. There wasn’t any awareness that pregnancy would be a risk factor for developing heart disease. Even participants with pre-existing comorbidities were not aware of the relationship of their underlying medical condition to heart disease. On the contrary, concern about other medical conditions diverted attention from any focus on heart disease and heart disease risk. Patients with conditions like hypertension were aware of the immediate risks but unaware of the long-term cardiovascular implications. There was also little awareness among participants that pregnancy could increase future heart disease risks.
Summary of Patient Quotations by Theme.

Emotional Response to CVD Risk Assessment
Learning about the CVD risk triggered a strong emotional response among most participants. There was nearly uniform reporting of surprise when participants were informed that they were at risk for CVD. The positive CVD risk assessment also triggered concern among most participants, especially those with family histories of heart disease. One participant shared, “I was extremely worried because of what had happened to my dad. My dad died from [a heart attack]” (Participant 9). Clinicians played a key role in managing these emotional responses, with some patients appreciating the clear follow-up plan and close monitoring.
All Participants Wanted More Written and Digital Educational CVD Resources
While some participants felt they were given sufficient information regarding the positive risk assessment, others felt they were not properly informed about heart health and CVD risk. Respondents took the information about their CVD risk very seriously and reported an eagerness to learn about CVD in pregnancy. Six participants said they would have liked to learn more during the risk assessment (Participants 1, 3, 4, 5, 6, 9) and some wanted to have more information about their CVD risk and any impact for their baby. One respondent said, “The doctor gave no explanation, just said not to worry, and sent for follow-up. I would have liked more info and how it impacts the child” (Participant 6).
These participants suggested clinicians should provide access to comprehensive educational materials in hard copy or digital format. Overall, participants felt that they would have liked more information about the association between CVD risk during pregnancy and postpartum; they reported checking the internet themselves after the clinic visit, although they were aware of the potential for misinformation on social media. Even when knowing that information might be distorted, stories on blogs or chat groups could emotionally impact the patients. Clinicians were important in helping patients process these emotions. Respondents appreciated that CVD risk was identified. Furthermore, they felt reassured that clinicians conducted follow-up tests and monitored the patient closely. One participant could not remember the clinician's cognitive information about CVD risk but said she felt reassured that there was a “game plan” (Participant 2). Another participant who self-described herself as “not a type who wants to know all details” stated that her clinician provided a good explanation at a level that she could understand (Participant 8). A third participant stated she received good verbal explanation but noted that the provider did not follow up with written material (Participant 7).
Pregnancy Is a Motivator But Also a Temporary Barrier to Behavior Change
Some participants reported they were concerned about the impact of their CVD risk on the pregnancy's development and health. “We want to make the risks as small as possible, not just for myself, but for my baby, too. I would try anything that they recommend” (Participant 2). “I guess if I’m affected to a certain degree, then the baby would be affected” (Participant 7). Two respondents specifically stated that they would attempt CVD risk reduction behaviors to maintain a healthy pregnancy (Participants 3, 6). “I’m open to doctors’ guidance, I’m definitely willing to do whatever the doctors recommend for, my health and the health of my baby.” (Participant 6). For others, lifestyle changes were difficult to implement during pregnancy. “With the food it's just a struggle because of the nausea” (Participant 4). “I haven't been able to do much exercise because I haven't felt very energetic” (Participant 10). “I was going to start doing more exercising, but when I do too much, I start to lose my breath and the palpitations-…” (Participant 6). “I can maybe only stand for about 20–30 min and then I start not feeling well…” (Participant 2).
A few Participants Link Cardiovascular Health with Adverse Social Determinants of Health
Some participants brought up adverse social determinants of health as barriers that required changes at community level. Several comments mentioned the existence of food deserts. “It can be harder for some people to go to the store to get fresh produce because it can be expensive, and it is easier to go get fast food” (Participant 1).
A major barrier for physical activity and exercise is the lack of time due to work schedules and household chores. “It's just the timing, when my husband is here, he can help” (Participant 6); “If you don't plan yourself well, about time to exercise about time to go for therapy…then it could mess you up…” (Participant 1).
One participant mentioned several other structural impediments such as high cost of living “We're always working because even though legally you can take time off from work, the rents in California are horrendous…” (Participant 5). She also reported the struggles of living in a resource-limited neighborhood with few options for safe physical activity for herself and her children. “The public parks here in the West side are very bad. They're not taking care of them. There are swings that are missing…. The parks my daughter likes are on the East side of the city and those parks are so beautiful” (Participant 5).
Lack of insurance coverage was also an impediment for patients who need to use prescription drugs to lower blood pressure or cholesterol levels. “If it comes to some sort of medication or treatment that a doctor could recommend, right now what would be stopping me is that I’m having problems with my insurance” (Participant 5).
Discussion
In this study participants who underwent a novel screening for CVD risk during pregnancy or in the postpartum period brought to light challenges and issues with implementing this risk assessment. Overall, there is a lack of patient knowledge and awareness regarding CVD risk and pregnancy.
The surprise of being potentially at risk for CVD during and/or after pregnancy led a strong emotional response in some patients especially if they already had pre-existing issues with anxiety or family members with heart health problems. This brings to attention that the lack of awareness of CVD-related risks could impact women's health beyond the pregnancy and calls for a need for enhanced patient and community education.
Prior qualitative studies with postpartum people who have cardiovascular conditions revealed a knowledge gap of associated future health risks that improved significantly with health education and six months of remotely delivered lifestyle coaching. This led to increased recognition of CVD risk reducing strategies and a greater motivation to modify their health behavior. 18 One study of Australian women who developed hypertensive disorders during pregnancy (HDP) found that the structured postpartum follow-up and support not only improved knowledge of future risk with HDP but also motivated risk-reducing behavioral change. 19 Pregnancy undoubtedly is a window of opportunity to make life changes that improve cardiovascular health for the life course. Clinicians need to be aware of their patient's perceptions and values to guide counseling around CVD risk-reducing behavioral change.
The findings of the study illustrate that patient perceptions, emotions, and behavioral intent are crucial elements in exploring patients’ perspective on the purpose of CVD risk assessment in pregnancy and the knowledge of how they felt when they first received their risk assessment result is extremely valuable. Patients’ observations can reveal areas of potential improvement for delivering healthcare. 7 While clinicians may not have time to engage in detailed explanations about CVD and pregnancy during the clinic visit it would be helpful to provide internet links with accurate and reliable information in the after-visit instructions. Clinicians could also use visual aids to communicate the patient's individual risk level, its potential consequences, and list of next steps such as appointments with specialists and follow up tests [see Figure 2]. Follow-up appointments should also ensure that this information is revisited to confirm patient understanding. 20 While we aimed in this study to assess behavioral intent, several of our interview participants reported that they had already implemented lifestyle changes at the time of the interview, showing the potential of the risk assessment to help patients to use and apply health information for health promotion and disease prevention. This shows the potential of CVD risk assessments to increase CVD health literacy among pregnant patients and their communities.

Visual patient aid explaining CVD risk and follow up steps.
While this study focused on exploring modifiable individual-level perceptions and lifestyle changes, it is important to note that some of the barriers to cardiovascular health care system issues at the structural and policy level. Health care professionals should work synergistically with stakeholders and policy makers to advocate for better work conditions, better prescription drug coverage, better maintained public parks, safe neighborhoods, and elimination of food deserts. Clinic interventions, such as this CVD risk assessment tool, need to be complemented with community outreach and resources to ensure that patients can complete any medical evaluation or treatment required.
Future research with larger and more diverse samples, longitudinal follow-up, and broader geographical representation could further enhance our understanding of this important public health issue. Having a positive risk assessment for CVD and its effect on maternal and neonatal outcomes is currently under investigation.
Limitations
The qualitative approach allows for comprehensive data collection through participant interviews, enabling researchers to delve deeply into participants’ perceptions, experiences, and understanding of cardiovascular disease risk during pregnancy and postpartum periods. However, the study did not assess the actual behavior change or the sustained impact of being identified to be at risk for heart disease, which could provide valuable insights into the effectiveness of interventions over time. While our purposive sampling approach provided a diverse group of study participants by demographics and medical history and prenatal care setting, the small sample size may limit the representativeness of the findings and the results should be interpreted with caution due to the limited generalizability. A mixed method study with a larger sample that collects patient risk behavior and medical outcomes in addition to qualitative data, can provide insights into the effects of CVD risk assessment on maternal and neonatal outcomes. Furthermore, a longitudinal study that monitors behavior changes and heart health over time could provide deeper insights into the long-term effects of CVD risk assessment.
Conclusions
Obstetrical encounters are good opportunities to assess patients’ risk to be diagnosed with previously unknown risk CVD. However, the heightened focus on achieving a successful pregnancy outcome may lead to fear or anxiety when patients learn that they might be at risk of heart disease which needs to be addressed in the clinic encounter. These study findings highlight the need for empathetic, patient-centered communication during clinical encounters and for patient health literacy to assess, evaluate, and use health information and services for their health decisions and actions. Pregnancy serves as a significant motivator for encouraging women to adopt CVD risk-reducing behaviors. This life stage inspires them to embrace healthier habits for themselves and their families, make informed decisions, and seek comprehensive prenatal care. These proactive measures not only help reduce pregnancy complications but also lay a foundation for long-term health benefits. Moreover, clinic-based risk assessment interventions should be paired with efforts to enhance health literacy among individual patients and the broader community to achieve a lasting impact.
The findings from this study underscore the value of integrating CVD risk assessments into routine obstetrical care, paired with efforts to enhance individual and community health literacy. This dual approach is essential for empowering patients to engage in proactive, sustainable behavior changes. The interview process provided valuable insights into patients’ experiences with the screening tool, emphasizing its educational potential. Further research is needed to explore patient awareness of CVD risk and their willingness to modify lifestyle behaviors. Such studies will be instrumental in refining interventions to reduce the burden of CVD on maternal morbidity and mortality, ultimately advancing patient-centered care.
Footnotes
Acknowledgements
We would like to acknowledge the dedication and hard work of Tin Tran, MPH, for working on the literature review and interview development and administration, Julia Becerra, MPH, for administrative support, and the study participants for their time and insights.
Data Availability Statement
De-identified interview transcripts are available upon request.
Declaration of Conflicting Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
All subjects participated voluntarily and received a small compensation.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this original study is from NIH study #R21HD101783 and the Gordon and Betty Moore Foundation, Diagnostic Excellence Initiative #9055
Gordon and Betty Moore Foundation, National Institute of Child Health and Human Development, (grant number GBMF9055.01, #5R21HD101783).
Supplemental Material
Supplemental material for this article is available online.