
Abstract
When the consultation is predominantly verbal, existing research in clinician–patient communication indicates that many patients struggle to understand and recall medical consultations or may not understand the extent of their illness or the purpose of their treatment plan. When the clinician–patient discussion centers around the risk of a repeated cardiovascular disease (CVD) related event, qualitatively assessing what factors affect the communication of this risk may guide the creation of effective communication solutions. Semi-structured interviews were conducted with 17 clinicians treating patients at stages along the cardiac rehabilitation patients’ journey. Thematic analysis identified factors that prevent patients from understanding the risk they face of experiencing a repeated cardiac event. Results indicate a clearer understanding of the cardiac rehabilitation patient journey by means of a patient journey map; an overview of how CVD risk is currently communicated; and the factors that affect communication of these risks in the form of themes and sub-themes. Findings shape the proposal of an evidence informed model of opportunities for enhanced digital media supported communication in cardiac rehabilitation.
Keywords
Introduction
Of all human illnesses, cardiovascular disease (CVD) is the number one cause of death globally, taking an estimated 17.9 million lives each year (representing 32% of all global deaths). One-third of these deaths occur prematurely in people under 70 years of age. 1 However, identifying those at highest risk for future CVDs and ensuring they receive appropriate treatment can prevent most deaths from this disease. This early detection of, and intervention in treating people either with established CVD or who are at high risk for developing CVD, is the core focus of a clinician–patient risk discussion (CPRD). The CPRD is defined as “a dialogue between the clinician and patient about potential for atherosclerotic cardiovascular disease risk reduction benefits” 2 ,(p1361) specifically as relates potential lifestyle or therapeutic interventions under consideration.
However, we know that many patients struggle to understand and recall medical consultations3–8 and the extent of their illness or the purpose of their treatment plan,9–11 with resultant healthcare and economic costs. 12 “In developed countries, adherence among patients suffering from chronic diseases averages only 50%, and it is even lower in developing countries” 13 (p1) leading to more hospitalizations, increased medical costs, higher social impact and more premature deaths, which the Organisation for Economic Co-operation and Development (OECD) has estimated at 200 000 patients per year. 14 Studies estimating the lack of medication adherence to cost European governments €125 billion per year (hospitalization, primary care services, rehabilitation costs, etc) and in the United States 15 reveal that this lack of patient understanding and patient adherence may be associated with approximately 125 000 deaths, and at least 10% of hospitalisations 16 accounting for one in 10 patients in their hospitals at any one time, contributing to increases in morbidity and mortality. 17
To better understand ways in which the CPRD could improve adherence, this study aimed to identify (1) what the patient journey looks like for cardiac rehabilitation patients; (2) how risk is currently communicated to patients; (3) what inhibits successful communication of this risk; and (4) where digital media might best support or enhance communication of risk along this patient journey.
Methods
Patients with cardiac diseases or cardiac-related problems in Ireland are typically given a 75-page booklet 18 showing the following 4 phases of cardiac rehabilitation: (1) In Hospital; (2) Going Home; (3) Exercise and Education Programme; and (4) Community or Home Based Programme. This study includes interviews with clinicians from these phases in order to assist in fully understanding the patient's journey along the cardiac rehabilitation process in Irish public hospitals.
The Study Context
The study was conducted in 2 Irish public hospitals. Following a cardiac event, a patient is referred to relevant healthcare clinicians for rehabilitation.
These interactions typically take place immediately after their medical event (Phase 1), and in subsequent scheduled visits (Phase 2 to 4). Over 12 months, this study was conducted with clinicians and patients in 2020/2021.
Theoretical Framework
This research used a qualitative approach, using Braun and Clarke's thematic analysis (TA),19,20 allowing for the systematic analysis and subsequent interpretation of the experiences of doctors with cardiac patients. This presented a pragmatic approach to qualitative analysis that involves searching for patterns or themes from transcribed textual interview data through the use of codes. These identified patterns in code detection allow for the extraction of themes that highlight important information relating to the communication between patients and other healthcare professionals throughout their post-cardiac event journey.
Sampling Strategy
A total of 17 clinicians were interviewed as part of this study, totaling a duration of approximately 6 and a half hours of interview time across all participants. The size of this study was determined by purposeful sampling. All necessary ethics committee approvals were received, and details are provided in the Ethical Approval section of this paper. Inclusion criteria for research participants consisted of participants needing to be healthcare professionals working with cardiac rehab patients in the hospitals selected for this research.
Data Collection
This method involved interviewing clinicians, ranging from consultant cardiologists to clinical nurse specialists and other allied health professionals in selected Irish public hospitals. Participants were interviewed individually in person as well as over video calls between September and December 2021. Each of these interviews were recorded.
Data Analysis
This study used a TA approach to identify factors from the lived experiences of clinicians in their cardiac patient communication. Thus, having transcribed the interviews, the data were then analyzed using TA, which enabled identification, analysis, and reporting of themes within the data. Findings stemming from this TA are outlined in the results section.
Results
Reporting of the results of the analysis is divided into 3 categories: (1) a clearer understanding of the cardiac rehabilitation patient journey in Ireland; (2) an overview of how risk is currently communicated; and (3) the factors that affect communication of risk. Each of these are discussed below.
The Cardiac Patient Journey
The 17 semi-structured interviews with various clinicians were audio-recorded and transcribed to reduce the occurrence of errors or misinterpretations. By coupling the data analysis from the interviews with the 4 phases of cardiac rehabilitation in Ireland, the following schematic (Figure 1) was devised in order to provide a more detailed schematic of the patient journey.

Cardiac patient journey.
Its additions include: clinical appointments before and after the cardiac event; approximations of the days, weeks, and months of each stage; durations of each clinician encounter; alternative pathways to phases 1 and to outpatients via referrals; as well (in many cases) the need for an annual check-up with outpatients.
An Overview of How Risk is Communicated
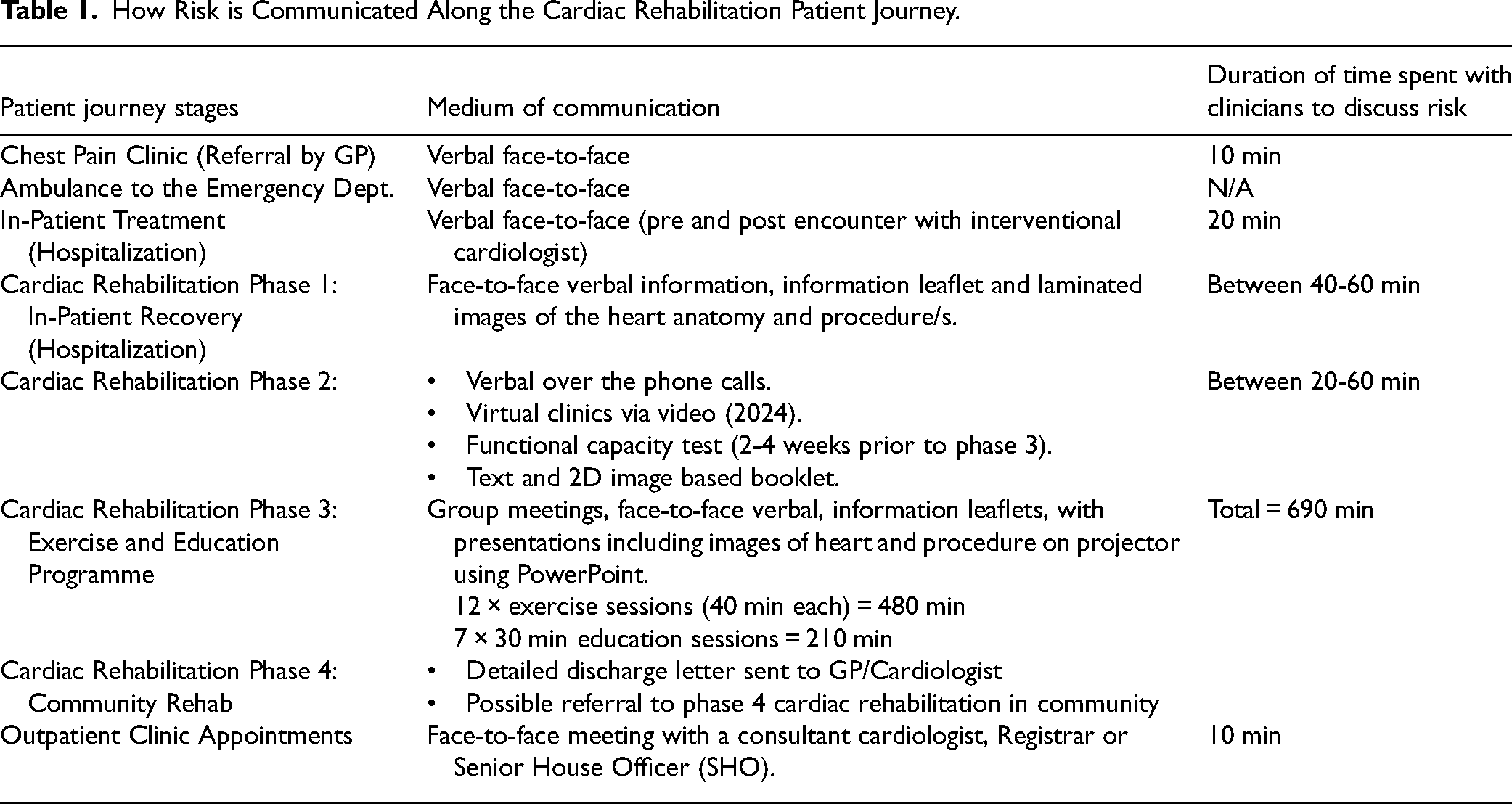
Table 1 outlines each of the patient journey stages, along with the corresponding medium of communication of risk with their clinician, and the duration of each appointment.
Factors That Affect Communication of Risk
The 6 steps of the Braun & Clarke TA model are outlined in this section.
Phase 1: Data Familiarization and Writing Familiarization Notes
After transcribing the interviews into text, the first step was to become familiar with the data by reading it in its entirety before delving into specific items.
Phase 2: Systematic Data Coding
This involved the coding of the data. “Coding” refers to highlighting sections of the text within the primary data. Each code can be a single word, phrase, sentence, or paragraph, and the code used is very much like a shorthand label (or “code”) to describe their meaning, or intent.
Phase 3: Generating Initial Themes From Coded and Collated Data
Next, themes were created from the codes identified. This was achieved by reviewing the bank of codes created, identifying patterns within these codes, and generating the first iteration of (potential) themes within the data.
Phase 4: Developing and Reviewing Themes
In phase 4, it was necessary to compare themes to the data set and combine several themes where relevant. For example, Covid, acceptance and denial, time constraints and more were combined to form an overarching theme entitled “Being a patient is challenging” (later refined as “Complexities of the Patient Journey”).
Phase 5: Refining, Defining, and Naming Themes
In phase 5, this method of combining low-level (sub-) themes into refined, overarching, themes continued, with each of these themes now having a clear, succinct name and definition. This phase ultimately resulted in 4 primary themes, with sub-themes, as outlined in Table 2.
The Themes and Sub-Themes Identified by This Study.

Phase 6: Writing the Report
Finally, phase 6 refers to the “writing-up” step. In analyzing the factors that affect the communication of risk, our study identified 4 primary themes, and related sub-themes, from the interviews with clinicians, listed in Table 2.
Discussion
In summary, there are 4 main objectives of the study: to identify (1) what the patient journey looks like for cardiac rehabilitation patients; (2) how risk is currently communicated to patients; (3) what inhibits successful communication of this risk; and (4) where digital media might best support or enhance communication of risk along this patient journey. These first 3 research objectives have already been identified in the results section. In this section, the significance of these findings will be discussed, along with their role in exploring the fourth objective.
Several previous studies regarding the mapping of patient journeys have helped shape this study. These examine before and after hospitalisation, 21 heart failure congestion symptoms, 22 and opportunities for care and improve information delivery.23–26
What the Patient Journey Looks Like
Figure 1 outlines a more accurate depiction of the patient journey than the 4 arbitrary phase headings explained to patients. This is significant for patients in that it acts as a map, with signposts, durations of visits, and approximate timelines from once they enter the cardiac rehabilitation system.
An Overview of How Risk is Communicated
Table 1 outlines each of the patient journey stages, along with their corresponding medium of communication of risk with their clinician, and the duration of each appointment. This is significant as the table identifies (1) additional hospital visits; (2) the variety of means of communication at each stage; and (3) the variance in time spent between clinician–patient at each stage (from less than 10 min to 720 min).
How Risk is Communicated Along the Cardiac Rehabilitation Patient Journey.
The Factors That Affect Communication of Risk (as Themes)
When the consultation is predominantly verbal, existing research in the field of clinician–patient communication indicates that many patients struggle to understand and recall medical consultations,3–8 or may not understand the extent of their illness or the purpose of their treatment plan.9,27 However, findings indicate that there is a wide range of communication methods used at various stages along the patient journey. Theme 1 (Table 2) findings, echoing related research findings,28,29 also indicate that clinicians are open to, and in some cases are already using digital communication tools to assist in communicating risk and acknowledge that their patients are also open to the use of digital tools, including software applications, for the purposes of learning and understanding risk.
Although many of the participants espouse a desire to incorporate other more visual media (pamphlets, sketches, apps, images, charts, and videos) into the consultation process as a means of improving the patient experience, research literature argues that this cannot take place in isolation of the literacy and numeracy skills of the patient.30,31
Equally, the choice of media used to convey this risk to patients poses challenges. 32 Patients’ perceptions of the severity of their CVD and treatment preferences “are influenced by the tool used for risk communication, and risk perception influences a patient's willingness to consider therapy.” 33 ,(p1192)
Existing research suggests that “individual characteristics such as age, education, and numeracy, may affect not only risk comprehension but also the qualitative interpretation of risk.” 34 ,(p7) In this study, it was clear that patients’ age, gender, and location (rural or urban), as well as access to internet and smartphone technologies also play key roles in patients being able (or not) to access information about their disease, and, as a result, their ability to participate in the fulfilment of their treatment.
Theme 3 (Table 2) findings indicate that clinicians are also aware of clinician challenges that affect optimal communication of risk to patients. One such challenge is the importance of having suitably interoperable health IT systems in place to effectively carry out their roles. Specifically, in relation to the CPRD, 35 this call for more appropriate health systems is echoed in other research literature. 36
Tying together the first 3 themes, and ever-present throughout, is the fourth theme of time. “Dedicating sufficient time to high-quality CPRD offers an opportunity to strengthen clinician–patient relationships, patient engagement, and medication adherence.” 2 However, findings from our research show that along the patient journey map, there are stages where time is limited and where there will never be sufficient time to communicate risk to patients at these bottleneck stages. Communication of risk does not have to be focused exclusively on these pressurized areas, and perhaps there are other opportunities for communication of risk that exist elsewhere along the patient journey other than the tight (<10 min) consultation windows.
Opportunities for Digital Media Supported Communication
The findings from research objectives 1, 2, and 3, confirm, complement, and contribute to existing literature. They have enabled the researchers to identify opportunities for digital media supported communication—the fourth purpose of this study.
By plotting the stages of the journey, quantifying the time spent with clinicians at each stage, and cognizant of the factors affecting the communication of risk (as outlined in the themes), a clearer picture—or concept map—emerges. This is an evidence informed model of opportunities for enhanced digital media supported communication in cardiac rehabilitation (Figure 2).

Evidence informed model of opportunities for enhanced digital media supported communication in cardiac rehabilitation.
Informed by the TA findings of objective 3 (Table 2), this conceptual map (Figure 2) plots the findings from research objective 1 (Figure 1) and objective 2 (Table 1) in the form of an encounter duration graph. Along this encounter duration graph are the potential areas for use of tailored digital media interventions to assist in clinician–patient communication of risk. These are illustrated by the grey circles—the greater the circle, the greater the opportunity for media supported communication of risk. In particular, for phases 1, 3, 4, and cardiology outpatients appointments, there are potential windows of time to receive clinician-led multimedia related learning content to assist in the communication of risk.
Strengths and Limitations
This study involved interviewing doctors, nurses, and allied healthcare professionals along the cardiac rehabilitation patient journey. Researching healthcare professionals’ perspectives provides an alternative to interviewing patients, and is arguably more reliable, objective, and gathered from a more experienced source in understanding the patient journey.
Studies have shown that patients are not always reliable narrators of their health, 37 due to ambiguity and contradiction in their accounts. 38 Patients may not be willing to voice their dissatisfaction with their doctors for various reasons. 39 They are also potentially once-off users of this cardiac rehabilitation system, whereas clinicians have experience in diagnosing and treating thousands of patients, and, as a result, are arguably more attuned to trends, challenges, and opportunities within this dynamic working environment.
The sample size of 17 participants in this study is small, but it yielded 6.5 h of recorded interviews with a broad range of healthcare professionals interacting with cardiac patients along their patient journey in Irish public hospitals. By varying the disciplines of the healthcare professionals (consultants, interns, nurses, occupational therapists), this approach contributed to a deeper understanding of communication of risk along the patient journey.
One limitation of the patient journey map is that it does not include GP visits or appointments with other healthcare professionals outside of cardiology.
Conclusion
The following 4 research objectives were achieved: To identify (1) what the patient journey looks like for cardiac rehabilitation patients; (2) how risk is currently communicated to patients; (3) what inhibits successful communication of this risk; and (4) where digital media might best support or enhance communication of risk along this patient journey.
The findings in relation to each of these research objectives complement existing research literature in the field of clinician–patient communication while also contributing to new learning in the field of cardiac rehabilitation in the form of a more accurate understanding of this patient journey, which has the potential to increase basic understanding of the timelines and events facing the patient 12-months post cardiac event; a structured taxonomy of the communication of risk challenges and considerations within the cardiac rehabilitation patient journey (themes and sub-themes); and an evidence informed model of opportunities for enhanced digital media supported communication of risk along this patient journey in cardiac rehabilitation. Through these contributions this study's findings can impact future research and future cardiac rehabilitation care.
Future Research
For other researchers in this field, these findings, in the form of a structured patient journey and taxonomy of communication of risk challenges, may inform future research and development studies into the design of appropriate clinician–patient communication aids.
The evidence informed model of opportunities for enhanced digital media supported communication in cardiac rehabilitation has potential to influence software designers and developers when considering multimedia interventions along this patient journey within cardiac rehabilitation. As part of a wider research project, the learnings from these findings serve as a basis to design and develop appropriate multimedia interventions aimed at enhancing this communication process along each of the stages within the patient journey in cardiac rehabilitation.
Future Care
For clinicians, informed by the findings of the data analysis, as well as learnings from pertinent research literature, this study reinforces the idea that any interventions to assist in the communication of risk should go beyond mere information provision. They should also include strategies for managing other concerns such as digital literacy, numeracy, willingness and ability to access content, as well as a range of socio-cultural, behavioral, and emotional factors.
In conclusion, this study contributes valuable insights into the patient experience in cardiac rehabilitation and the complexities of clinician–patient communication. The analysis of this complex inter-relationship between patient and healthcare professional yields significant results and highlights the need for further research into patient experience design in the field of cardiac rehabilitation.
Footnotes
Acknowledgments
The authors sincerely thank all the participants in this research.
Authors Contributions
Mark Campbell: conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, validation, visualization, writing—original draft, writing—review & editing. John William McEvoy: conceptualization, supervision, resources, writing—review & editing. Gavin Calpin: project administration, resources, writing—review & editing. Fiona Concannon: conceptualization, funding acquisition, supervision, methodology, writing—review & editing. Sam Redfern: conceptualization, funding acquisition, supervision, methodology, writing—review & editing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Irish Research Council (grant number EBPPG/2019/8).
Ethical Approval
Ethical approval to report this case was obtained from both the Clinical Research Ethics Committee (CREC) in the Galway Hospital Group (Reference: C.A.2814) and the University of Galway Research Ethics Committee (Reference: 2020.08.003).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Clinical Research Ethics Committee's (CREC) in the Galway Hospital Group (Reference: C.A.2814) and the University of Galway Research Ethics Committee's (Reference: 2020.08.003) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the healthcare professional(s) for their anonymized information to be published in this article.