
Abstract
Our objective was to understand how empathy and self-awareness content, alongside traditional deescalation training, might impact ambulatory clinic staff responses to patient and family escalation events. Verbal and physical workplace violence is escalating across healthcare organizations, including ambulatory clinics. Deescalation content is often developed with acute care, psychiatric, or emergency care in mind. There is a need for relevant and empathic deescalation training for ambulatory clinic staff to address their specific needs. We developed empathic and self-reflective deescalation training which was interactive and relevant to ambulatory clinic staff. Staff were trained using both in-person and virtual modalities. Participant self-reflection pre- and postintervention questionnaires indicated increases in understanding and application of deescalation methodologies. Multiple ambulatory clinics where staff participated saw a decrease in patient complaints and grievances. Participating ambulatory clinics also saw an improvement in the likelihood to recommend practice. However, participating ambulatory clinics did not see a reduction in reported patient-involved workplace violence events. Ensuring both empathy and self-awareness content in deescalation training, along with relevant ambulatory clinic scenarios, support ambulatory staff to respond effectively and appropriately to escalation events, helps reduce patient complaints, and improves patient satisfaction.
Keywords
Introduction
Verbal and physical workplace violence is escalating across healthcare organizations. Patient-facing healthcare workers continue to navigate the impact of social unrest, pandemic policy enforcement, and evolving patient expectations with limited resources and a reduction of staff. Eighty percent of violent incidents reported in healthcare settings were caused by interactions with patients, 21% of registered nurses and nursing students reported being physically assaulted and over 50% verbally abused over a 12-month period, 12% of emergency department nurses experienced physical violence, and 59% experienced verbal abuse over a 7-day period. 1 During the COVID-19 pandemic, the APA reported that 8 out of 10 Americans stated the pandemic has created significant stress in their life. 2 Healthcare employees are often bearing the brunt of that stress as seen in little patience or tolerance and short fuses, with patients taking their frustrations out on the very people trying to care for them. Meanwhile, healthcare staffing shortages and limited resources continue to put strain on current employees. 3 A recent survey reported that 93% of healthcare workers were experiencing stress, 86% reported experiencing anxiety, 77% reported frustration, 76% reported exhaustion and burnout, and 75% said they were overwhelmed. 2 Many industries are facing increases in consumer outbursts and violence, including food service, aviation, and retail. 4 Burnout is a significant problem, particularly among U.S. nurses, who are leaving their jobs or considering leaving their jobs. 5
The Joint Commission defines deescalation as a combination of strategies, techniques, and methods intended to reduce a patient's agitation and aggression, but there is little research about deescalation training efficacy or guidance for what is considered the gold-standard. 6 Deescalation training educates healthcare workers in situational awareness, early escalation recognition, and escalation mitigation strategies. 7 Deescalation training content is often developed with acute care, psychiatric, or emergency care in mind. Deescalation training content often includes elements of environmental safety, behavior recognition, and personal protection coupled with relevant scenarios.6,8,9 But each healthcare worker is affected by and ultimately responds to patient escalation events uniquely because of their values and past experiences. Personal awareness and understanding, often missing from deescalation training, is crucial to developing the confidence to execute common mitigation strategies and avoid further escalation. Because of increased escalation events, key stakeholders led by the patient experience team in a large academic medical center physician group practice, created and released a comprehensive deescalation training for patient-facing employees across 200+ clinics. Interactive trainings were held in-person and virtually. Participant self-reflection pre- and postintervention questionnaires were conducted showing improvement in participant understanding and confidence post training. Patient complaints were monitored before and after the intervention, seeing decreases after training among participating clinics. Patient-involved workplace violence events were monitored before and after intervention; however, decreases in cases were not observed. Patient satisfaction ratings were also monitored before and after the intervention, seeing an increase among participating clinics.
Background
There are indications of deficits within more standardized deescalation training and limited research within the ambulatory clinic setting. In a qualitative study of the perceptions of primary care staff, workers indicated the need for supervised, practical deescalation training methodologies, mandated attendance expectations, empathic communication training, and personal emotional awareness and management. 3 Similar needs arose within a qualitative study of nurses who indicated empathic communication and personal emotional awareness and management were key to effective patient deescalation. 10 Empathic communication training helps staff understand that each patient and family member “has a history, is part of a family, and lives in a community full of beliefs, values, social roles and legacies.” 11 This training includes behaviors such as active listening and recognizing the unique context patient escalation behaviors occur. 11 Ambulatory clinics face unique environmental, staffing, and patient concerns compared to traditional hospital settings. In another qualitative study of the perceptions of primary care staff, workers expressed the differences of deescalation training needs between administrative and clinical primary care employees. 12
The intersection of empathy and self-awareness could be moral imagination. Moral imagination is sustained attention on others through their concerns and drawing upon personal narratives and metaphors to respond appropriately. 13 Moral imagination is “shaped by the narratives individuals have lived by and lived through.” 13 We found that through intentional self-reflection on personal values and past experiences, healthcare employees will be better equipped to manage their emotions, practice empathy, and effectively execute deescalation strategies.
Methods
Self-awareness training included the ABC Technique of Irrational Beliefs, a keystone of cognitive therapy 14 developed by Psychologist Albert Ellis. 15 He suggests that each of us holds a unique set of beliefs about ourselves and our world that guide us through life and determine our reactions to situations we encounter. Unfortunately, some people’s beliefs are largely irrational, guiding them to act and react in inappropriate ways. The ABC model includes the Activating Event which can be a word, gesture, experience, action, or event that touches off an immediate emotional reaction in us. The Consequence is our reaction such as raging, attacking, retaliating, breaking into tears, fleeing, fighting, or freezing. The Belief is our worldview, history, and values that can be exaggerated or irrational, through which we filter the Activating Event. Ellis believed that it is not the Activating Event that causes negative emotional and behavioral consequences, but rather that a person interprets these events unrealistically through their belief system that causes the consequences. The Activating Event is often easily recognizable or seen; as is the Consequence. But the Belief is unseen and often goes unnoticed. By reflecting on our Beliefs, we gain understanding that influences our reactions. A better reaction can help improve our physical safety, emotional well-being, and patient communication. The framework of Ellis’ ABC model, applied to healthcare activating or “trigger” events, helped participants better understand the unique beliefs, values, and past experiences through which they filter escalation events. Self-awareness training reviewed preconscious physiological responses to activating events, and the impact our sympathetic and parasympathetic nervous systems have on vocalization, posture, and body language. Attendees practiced common breath control exercises to combat physiological stress responses that may hinder deescalation. Empathy training included value listening during escalation events. Value listening looks past the patient's escalated emotional expression (words, tone, volume, gestures) to identify what the patient values most in that moment, what's most important to them. Value listening combines active listening techniques with the five whys, a common root cause analysis exercise. The Five Whys Technique, developed by Sakichi Toyoda in the 1930s, is used for troubleshooting and quality improvement by asking why up to five times. Thinking deeper about why a patient is aggravated up to five times can help staff respond with greater understanding and compassion. Value listening helps the deescalator respond empathically to what's most important and not risk further escalation (ie “I see through this experience we have not valued your time” vs “I’m sorry you're so upset”). Finally, attendees learned the four expressions of anger to understand how they express anger when stressed to more appropriately apply deescalation techniques. The Four Expressions of Anger include passive, passive-aggressive, aggressive, and assertive responses. This unique content, coupled with group activities and interactive scenarios, amplified common deescalation training content for better overall outcomes.
Deescalation training was offered to all ambulatory clinic employees but focused on patient-facing, nonphysician staff. The training was approximately 2 h in length, in-person or virtual. Each course was led by a member of the ambulatory clinic patient experience team. Individual participation was tracked and aggregated by clinical specialty. Participants were sent a preintervention and postintervention questionnaire to gather a self-assessment of the course content and their perception of the presenters, resources, and course value. Pre- and posttime periods were established for clinical divisions based on the percentage of nonphysician staff trained. Patient satisfaction survey results, complaint and grievance case counts, and workplace violence case counts were monitored for each clinical specialty. Statistical analysis was applied to patient satisfaction survey results and participant questionnaire results.
Results
De-escalation training was offered to non-physician staff in four ambulatory clinical specialties: otolaryngology, gynecology/obstetrics, general internal medicine, and medical specialties (i.e. rheumatology, gastroenterology, pulmonary, etc.). 49 employees (72%) completed training in otolaryngology. 140 employees (62%) completed training in gynecology/obstetrics. 80 employees (23%) completed training in general internal medicine. 63 employees (31%) completed training in medical specialties. Participants were sent a preintervention and postintervention questionnaire to gather a self-assessment of the course content and their perception of the presenters, resources, and course value. Seven questions regarding de-escalation practices, empathy and self-awareness principles, and self-care were asked and participants rated their confidence 0.61 higher on average after the course. (Table 1). N size, standard deviations, and p values can be found in Table 1. The greatest improvement in confidence ratings pre to post included: I can identify three ways to practice self-care after a trigger event (+0.92),·I can appropriately respond to a patient/family member who is verbally abusive or demanding (+0.71), I understand what a trigger event might be in a healthcare setting (+0.65), I can confidently redirect an angry or upset patient/family member (+0.61).
Pre/Postintervention Participant Questionnaire.

Note. 5-point Likert Scale: strongly disagree–strongly agree.
The postintervention survey also asked eight additional questions measuring the participant’s perspective of the course, teaching methodologies, and its overall value. On average, participants rated these questions 4.47 out of 5 (Table 2). Highest-rated questions included: I enjoyed how my instructor taught the skills lab (4.58), The teaching methods used in this skills lab were motivating and helped me to learn (4.53), My instructors used helpful resources to teach the skills lab (4.49), The teaching methods used in this skills lab were helpful and effective (4.47). Positive feedback from the post-intervention survey included: “I was assaulted by a patient in 2015. He put me in a chokehold, herniated 2 discs in my neck, and sprained my back. I was out of work for 8 months. If I had this teaching back then, it would be a different narrative.” and “The class was very informative and, I believe, effective. It was a great reminder of our purpose in the healthcare setting while also reminding us to take care of ourselves as we take care of our patients. The instructors were very good with the presentation.” and “This course was very useful and gave insight on how to respond/de-escalate.”
Postintervention Participant Questionnaire.

Note. 5-point Likert Scale: strongly disagree–strongly agree.
Likelihood to recommend practice mean scores improved 0.04 on average across four clinical divisions. N size, standard deviations, and P-values can be found in Table 3. Likelihood to recommend practice top box ratings improved 2% top box on average across four clinical specialties. When compared against vendor national benchmarks, this improvement equates to 17 percentile rank improvement on average (Table 4). The two clinical specialties with greater than 50% of their staff trained saw higher average top box rating improvement (+2.6% or +21 percentile rank) than the 2 clinical specialties with less than 50% of their staff trained (+1.5% or +13 percentile rank (Table 4).
Patient Satisfaction Survey Likelihood to Recommend Practice—M, SD, and P-Value.

Patient Satisfaction Survey Likelihood to Recommend Practice—Top Box Ratings and Ranks.
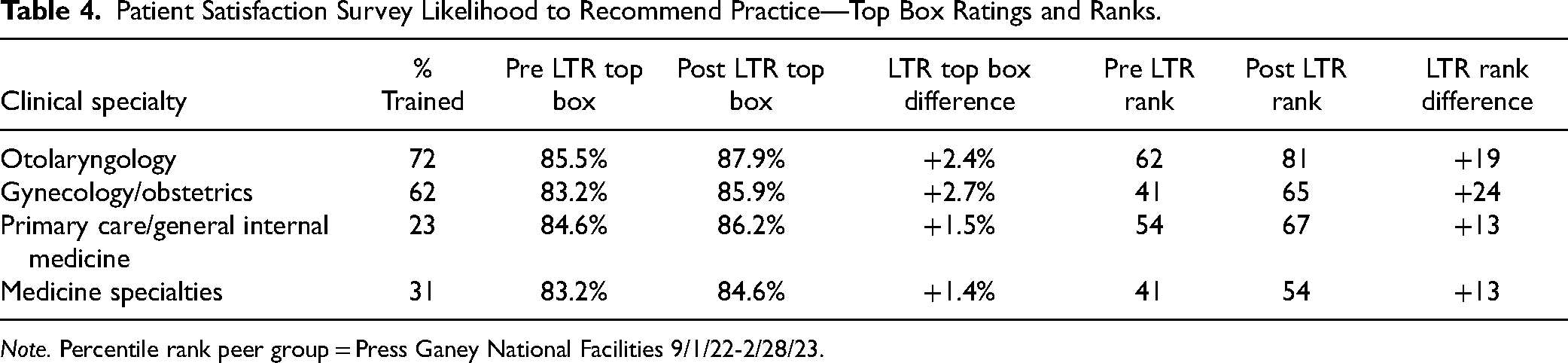
Note. Percentile rank peer group = Press Ganey National Facilities 9/1/22-2/28/23.
Complaint and grievance cases fell by 15 cases on average across the four clinical divisions. No standard benchmarking is available for these data (Table 5). Those divisions with over 50% staff trained did not see greater case count decreases than those divisions with less than 50% staff trained (Table 5). Only one clinical specialty saw the number of patient-involved workplace violence cases decline and only by one case pre to post. Workplace violence cases increased by five cases on average across four clinical specialties.
Patient Complaint and Grievance Case Counts.

No external benchmarking available.
Limitations and Future Considerations
One limitation for this study is the varied teaching methodology. This course was written to be in-person and interactive, but the length of the course and limited availability for staff across multiple sites to participate in-person encouraged us to shift to a virtual option. Another limitation is the various patient populations, care settings, safety resources, and staffing models across the four clinical specialties which likely impacted our comparisons. Other improvement initiatives executed simultaneously with the deescalation course throughout the various clinics during the study period may also have impacted our outcomes. Our organization continues to remind staff to document both verbal and physical escalation events. Increased event reporting may have impacted workplace violence case counts during the study period.
For future consideration, we would like to interview staff who received this deescalation course and those who did not, after they have experienced a patient escalation event, to better understand the application of the course content. We would also like to compare participants who completed deescalation training with empathy and self-awareness training to those who completed deescalation training without empathy and self-awareness training. The inclusion of objective measurement alongside self-reported outcomes would also be beneficial to future research.
Conclusion
By incorporating principles of cognitive therapy, physiological response, value listening, and other empathic practices, employees felt better equipped to practice de-escalation strategies. Participants rated their confidence 0.61 higher on average after the de-escalation course (Table 1). Deescalation training coupled with empathy and self-awareness content may also improve patient experience outcomes and decrease unsolicited patient complaints. Unfortunately, healthcare escalation events continue to rise. This requires unique, creative employee training that incorporates empathy, self-awareness and safe deescalation practices to ensure effective and compassionate responses to escalation events.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable.
Statement of Human and Animal Rights
Not applicable.