
Abstract
This study used the Medical Expenditure Panel Survey data (2010-2018) to examine associations between diabetes patients’ satisfaction with their provider and ratings of healthcare received, diabetes care self-efficacy, and monitoring adherence among nonpregnant reproductive age women with diabetes. The sample included nonpregnant women of childbearing age (18-45) with diabetes mellitus (n = 767; weighted n = 1.3 million women). The results indicated that patients who reported that their usual care provider always asked/showed respect for medical, traditional, and alternative treatments that the person is happy with had 2.59 times greater odds (95% confidence interval [CI]:1.32-5.10) of giving high ratings of healthcare (8-10) compared to those whose provider did not show respect for treatments. Results also showed that patients who reported they were asked to decide between a choice of treatments had 1.76 greater odds (95% CI:1.03-3.01) of diabetes care monitoring adherence. Findings demonstrate the importance of patient-centered communication experiences in relation to diabetes care monitoring adherence. Implications of the findings for clinical encounters are discussed.
Introduction
Inadequate or low-quality communication between patients and healthcare providers can result in lower rates of access to healthcare and quality of healthcare received, contributing to decreased patient satisfaction. 1 Working toward improving patient satisfaction is important, particularly in the diabetes care context, as overall patient satisfaction with patient-provider communication is associated with improved HbA1c (glycated hemoglobin) values (average glucose levels over the past 2-3 months) and quality of life. 2 Patient-reported outcomes are complementary in assessing whole-person care, rather than relying solely on biophysical health measurements, as are patient satisfaction. 3 More positive patient experiences are often related to self-reported health outcomes and even medication adherence. 4 Improvement in satisfaction may also improve treatment adherence, potentially decreasing the risk of developing diabetes complications like neuropathy or nephropathy. 3 People with diabetes who rate their providers higher on communication variables (often a proxy for patient satisfaction) are less likely to report racial and ethnic discrimination during clinical encounters, 5 yet it is unclear how patient satisfaction with healthcare providers among nonpregnant women with (type 1 or type 2) diabetes mellitus (DM) are related to DM care variables.
It is estimated that over 38 million adults in the United States have diabetes, yet nearly 1 in 4 who meet the laboratory criteria for having diabetes do not know they have it. 6 The number of DM cases in the United States is increasing, with over a million Americans diagnosed each year.6,7 The American Diabetes Association estimates the total costs of diagnosed DM increased from $245 billion in 2012 to $327 billion in 2017. 8 Recent recommendations for DM self-management practices include a proper diet, exercise, medication adherence, hypoglycemia prevention, and healthy coping. 9 Standards of DM preventive care include the following areas: (1) foot exam, (2) eye exam in which pupils were dilated, (3) blood cholesterol check, (4) influenza vaccine, and (5) HbA1c (number of times per year). 10
Previous research indicates patient experience, as assessed through ratings of healthcare received, is recognized as an indicator of healthcare quality. 11 DM outcomes are often associated to patients’ perceptions and related ratings of clinical encounters. 12 Further, improving DM patient self-efficacy is a strongly recommended practice for clinicians hoping to improve self-management behaviors and diabetes health outcomes. 13 DM self-efficacy refers to how confident one feels about performing DM-specific health behaviors, like administering medication, maintaining a healthy diet, exercising, and taking care of one's feet. 14 Better DM self-efficacy is associated with better glycemic control among adults with type 2 DM, 15 which is in turn associated with improved outcomes like foot care behaviors. 14 However, while there is some self-efficacy-related research among women with gestational DM,16,17 less is known about women with pre-existing DM. 18
There is a need to investigate associations between a DM patient's satisfaction with their provider and ratings of healthcare received, DM care self-efficacy, and monitoring adherence specifically among nonpregnant reproductive age women (18-45 years old) with DM. Most previous studies have investigated these variables from small cross-sectional samples,19,20 or have focused on women with gestational DM.17,21 Therefore, the purpose of this study is to use 9 years (2010-2018) of the Medical Expenditure Panel Survey (MEPS) dataset, 22 which is a large and nationally representative dataset to examine the aforementioned relationships in a population of interest. Studies using MEPS data focused on people with disabilities broadly, or people with DM more specifically, have investigated access to healthcare, 23 healthcare expenditures, 24 disparities in patient-physician communication for people with a disability, 1 and patient- and family-centered care.25,26
The theoretical framework guiding this study is the modified Interaction Model of Client Health Behavior (IMCHB).18,27 According to modified IMCHB, this framework demonstrates how patient singularity (eg, demographic characteristics of the patient population and perceived health status) can influence patient-provider interactions (eg, communication and satisfaction), intermediate patient outcomes (eg, ratings of care received, DM self-efficacy, and DM management), and even longer-term patient outcomes (eg, glucose control and improved maternal health outcomes).
While research shows the relevance of patient satisfaction, ratings of healthcare received, DM self-efficacy, and DM monitoring experience, there are no known studies to date that examine these constructs among nonpregnant women of childbearing age with DM (type 1 or type 2). Few studies have investigated more than 1 year's worth of data at a time. Therefore, in a sample of nonpregnant women of childbearing age with DM, we examine associations between satisfaction with their provider and (1) ratings of healthcare received, (2) DM care self-efficacy, and (3) monitoring adherence.
Method
Study Design and Data Sources
We used longitudinal data from the 2010 to 2018 MEPS. MEPS is a nationally representative dataset based on an in-person interviewer-administered household survey that collects information on healthcare use, expenditures, sources of payment, insurance coverage, satisfaction with healthcare, and quality of care for the US civilian noninstitutionalized population. MEPS uses a multistage 5-panel design that spans 2 years consisting of in-person interviews and self-administered questionnaires which facilitate the examination of changes in selected variables. In this study, predictor variables were measuring during panel 2 (year 1) and the outcome variables measured during panels 3 and 5 (year 2). More details of the MEPS complex sampling design and data collection procedures are reported elsewhere. 28 The sample included nonpregnant women of childbearing age (18-45) with DM. The final sample included 767 women (1,341,061 women when weighted).
Key Independent Variable
Satisfaction with healthcare provider. Individuals were asked: to rank (1 = never, 2 = sometimes, 3 = usually, 4 = always), “if there were a choice between treatments, how often would a provider ask you to help make the decision?”; whether providers (yes/no) “usually ask about prescription medications and treatments other doctors may give them”; and whether they “present and explain all options.” Individuals were asked: “thinking about the types of medical, traditional and alternative treatments that you are happy with, how often does a medical person/provider show respect for these treatments?” A combined variable was created to identify adults who were satisfied with their healthcare providers on all 4 aspects of patient-provider satisfaction compared to those who were less satisfied. 29
Dependent Variables
Dependent variables were ratings of healthcare, DM care self-efficacy, and DM monitoring adherence. For ratings of healthcare, women were asked to rate their overall healthcare received in the past 12 months on a scale from 0 (worst) to 10 (best). Based on the skewness of the data and previous studies, 18 ratings were dichotomized (0-7 and 8-10).
For DM care self-efficacy, women were asked, “How confident are you in taking care of your diabetes?” Responses were based on a Likert scale (1 = not confident to 4 = very confident). Responses were dichotomized (0 = not confident/somewhat and 1 = confident/very confident).
For diabetes monitoring adherence, 5 questions (yes/no) consisting of whether in the past 12 months women reported receiving: (1) foot exam, (2) eye exam in which pupils were dilated, (3) blood cholesterol check, (4) influenza vaccine, and (5) HbA1c (number of times per year) were combined. A total score of all the items was created and dichotomized based on whether patients adhered to all five recommendations.
Covariates
We evaluated age, marital status (never married, married, or divorced/widowed/separated), education level (no degree/less than high school (HS), HS graduate or general education degree [GED], bachelor's degree or higher), income (<200%, ≥ 200% federal poverty level), health insurance (any private, public, and none), time since diagnosis, and perceived health status (poor/fair and good/very good/excellent).
Data Analysis
Unweighted frequencies and weighted percentages for women overall and by ratings of healthcare, diabetes care self-efficacy, and diabetes care monitoring are reported. Chi square tests determined statistically significant differences between groups. We estimated multiple regression models for each of the dependent variables adjusting for covariates. Data analyses were conducted using STATA 17.0. The longitudinal weight was divided by nine to reflect the total number of years based on analytics recommendations.
Results
Selected Characteristics
Selected characteristics of nonpregnant women of childbearing age by ratings of healthcare, diabetes care efficacy, and diabetes care monitoring are presented in Table 1. Results are reported for women who had high healthcare ratings (8-10 on scale 0-10), diabetes care self-efficacy (confident/very confident), and diabetes care monitoring (met ≥5 recommendations). The overall mean age of women was 36.6 years. The weighted percentages were highest among women who were non-Hispanic White, married, had a high school diploma or GED as their highest level of education, any private health insurance, and good/very good/excellent perceived health status for all health outcomes. Results from the overall patient-provider satisfaction composite demonstrate that less than half of women with high healthcare ratings (46.9%; P < .05), diabetes care self-efficacy (44.0), and diabetes care monitoring (43.9%) were satisfied with all patient-provider satisfaction domains.
Bivariate Relationships Between Selected Characteristics and Ratings of Healthcare, Diabetes Care Monitoring Adherence, and Diabetes Care Self-Efficacy, MEPS, 2010-2018, N = 767.

Significance at * P < .05.
Abbreviations: GED, general education degree; FPL, Federal poverty level; HS, high school; MEPS, Medical Expenditure Panel Survey; SE, standard error.
Multivariate Results
Overall Patient Satisfaction With Provider
Results for the multivariable regression models are reported in Table 2. In adjusted models, overall patient-provider satisfaction was not statistically significantly associated with rating of healthcare (odds ratio [OR] = 1.86; 95% confidence interval [CI’: 0.95-3.62), diabetes care self-efficacy (OR = 1.35; 95% CI:0.62-2.93), nor diabetes care monitoring adherence (OR = 1.35, 95% CI: 0.78-2.36).
Crude and Adjusted Logistic Regression Models for Each Domain of Patient-Provider Satisfaction and Ratings of Healthcare, Diabetes Care Self-Efficacy, and Diabetes Care Monitoring Adherence in the United States, MEPS 2010-2018.
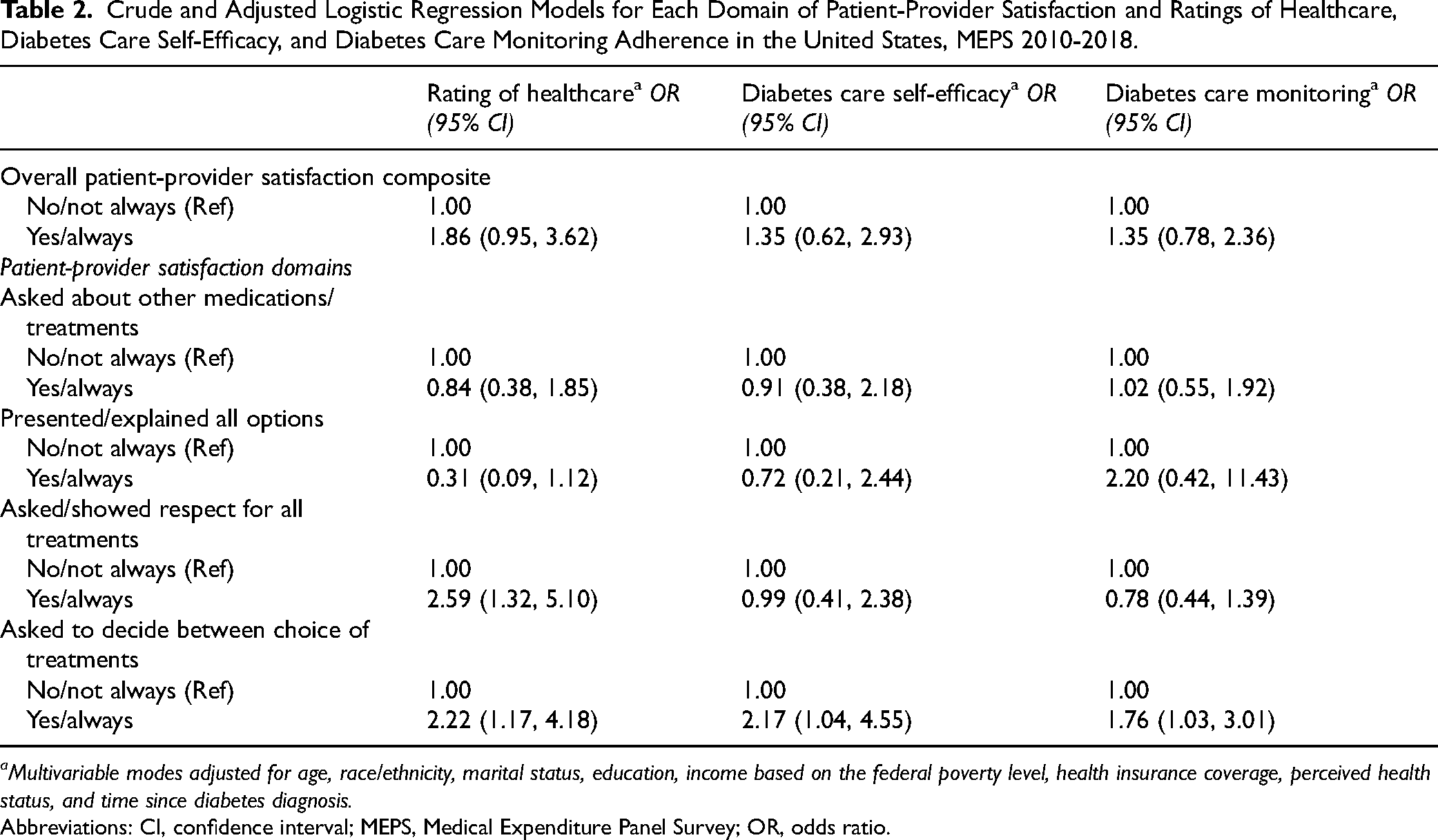
Multivariable modes adjusted for age, race/ethnicity, marital status, education, income based on the federal poverty level, health insurance coverage, perceived health status, and time since diabetes diagnosis.
Abbreviations: CI, confidence interval; MEPS, Medical Expenditure Panel Survey; OR, odds ratio.
Patient Satisfaction With Provider by Domain
In terms of ratings of healthcare, after adjusting for covariates, nonpregnant women of reproductive age with diabetes who reported that their usual care provider always asked/showed respect for medical, traditional, and alternative treatments that the person is happy with 2.59 times greater odds (95% CI:1.32-5.10) of giving high ratings of healthcare (8-10) compared to those whose provider did not show respect for treatments. Also, nonpregnant women of reproductive age with diabetes who reported their usual care provider always asked them to help make decisions between a choice of treatments had 2.22 times greater odds (95% CI:1.17-4.18) of reporting high healthcare ratings (8-10) compared to those whose provider did not ask them to participate in decision making after adjustment. Having a usual healthcare provider who presented or explained all options and asked about other medications/treatments was not statistically significantly associated with ratings of healthcare.
Regarding diabetes care self-efficacy, after adjusting for covariates, nonpregnant women of reproductive age with DM who reported their usual care provider always asked them to help make decisions between a choice of treatments had 2.17 times greater odds (95% CI: 1.04, 4.55) of reporting high healthcare ratings (8-10) compared to those whose provider did not ask them to participate in decision making. There were no statistically significant associations between the other patient satisfaction domain variables and diabetes care self-efficacy.
For diabetes care monitoring adherence, nonpregnant women of reproductive age with DM who reported their usual care provider always asked them to help make decisions between a choice of treatments had 1.76 times greater odds (95% CI:1.03-3.01) of reporting high healthcare ratings (8-10) compared to those whose provided did not ask them to participate in decision making after adjustment. There were no statistically significant associations between the other patient satisfaction domain variables and diabetes care monitoring adherence.
Discussion
Two main findings are noteworthy. First, patient satisfaction with healthcare provider was significantly associated with better healthcare ratings. This is consistent with previous studies with other populations living with diabetes.30,31 Yet, these studies focused on the logistical elements of healthcare ratings, including assessing availability of night or weekend appointments, waiting time, and ease of access or location. 30 The present study's findings extends such research by centering communication processes, like showing respect, in efforts to achieve truly collaborative care and decision making. 32
Second, while there were no other statistically significant differences between patient/provider satisfaction and diabetes care self-efficacy and diabetes care monitoring, there were statistically significant findings between components of provider satisfaction and higher ratings of healthcare and diabetes care monitoring adherence (eg, the intermediate patient outcomes of the modified IMCHB). Specifically, women of childbearing age with diabetes who reported that their usual care provider always asked/showed respect for medical, traditional, and alternative treatments that the person is happy were more likely to give high ratings of healthcare (8-10) compared to those whose provider did not show respect for treatments. Further, women of childbearing age with diabetes who reported their usual care provider always asked them to help make decisions between a choice of treatments had higher odds of reporting high healthcare ratings, and diabetes care monitoring adherence compared to those whose provider did not ask them to participate in decision making. These findings show the importance of respect for patient treatment preferences and participatory decision making. These findings are consistent with previous research examining dimensions of patient-provider communication demonstrating that nonpregnant women of childbearing age who reported that their provider always listened to them, explained things, showed respect, and spent enough time with them had greater odds of reporting high overall healthcare ratings and adherence. 33 Improving shared decision-making practices is considered as one of the best patient-centered communication strategies; simultaneously, recent research demonstrated that by not including shared decision-making strategies within a patient-provider interaction, there could be negative ramifications. Among parents of children with physical health conditions, including diabetes and other chronic conditions, lower shared decision-making practices and lower provider communication satisfaction were key factors associated with forgone care. 34 While we did not examine forgone care specifically, lower diabetes care monitoring adherence is problematic for long-term health outcomes for the patient and can lead to increased healthcare expenditures.
A strength of this study was the use of nationally representative data to measure patient satisfaction with provider among nonpregnant reproductive age women with diabetes—an understudied population. Because of the panel nature of the MEPS, we were able to examine the associations longitudinally, across 5 panels in 2 years. That is, we explored whether patient satisfaction with provider (measured during the first year) influenced ratings of healthcare, diabetes care self-efficacy, and diabetes care monitoring adherence (measured during the second year). Despite these strengths, there are several study limitations.
Limitations
One limitation is sample size which is due to the study sample being limited to nonpregnant women of reproductive age with diabetes who reported a healthcare visit in the past 12 months. As a result of our small study sample, even after combining multiple years of data, we were unable to evaluate other characteristics such as specialty or clinic type or stratify by patient race and/or ethnicity. Future studies could benefit from larger, more diverse samples to improve the statistical power and generalizability of the results. Our outcome measures were self-reported, which is subject to recall bias for diabetes care monitoring behaviors. Integrating patient healthcare records could alleviate this issue. Finally, the MEPS household survey does not distinguish between type of DM (type 1 or type 2). While there are some similarities in the 5 primary adherence behaviors, the day-to-day diabetes management strategies can vary by DM type (eg, people with type 1 DM may use insulin injections or insulin pumps, while people with type 2 DM are more likely to use oral insulin) and could play a role in the perceptions of care. Future research identifying DM type could provide more nuanced insights into diabetes care for different patient groups.
Practice Implications
Healthcare providers should encourage increasing shared decision-making practices for nonpregnant women of childbearing age, especially since it can improve both diabetes care monitoring adherence and improve patient healthcare ratings. Patient preferences may not always align with the clinical evidence (and related treatment options) that providers have, which complicates the process of achieving shared mind. While engaging in a dialogue to reach a collaborative decision is based on finding common ground and discussion to reconcile differences, 32 the rise of telehealth as a healthcare delivery modality adds another challenge. Healthcare providers should be trained on eliciting patient values and beliefs through mediated channels, such as BlueJeansTM or ZoomTM, rather than relying on the trust and rapport that is often easier to build through face-to-face channels. Interventions examining the use of digital tools in diabetes management have found the tools to be helpful in shared decision making. 35 Further, particularly for people with diabetes in rural areas, telehealth can positively affect patient-provider communication and shared decision making, resulting in improvements in self-reported understanding of diabetes and decreased HbA1c values. 36 Finally, the present study did not examine the influence of these factors among various ethnoracial groups due to sample size. Research shows that racially and ethnically minoritized women are less likely to report high healthcare ratings and high levels of diabetes care management than non-Hispanic White women. 18 Therefore, the study results do have important implications for racially and ethnically minoritized women with DM, who experience higher rates of diabetes diagnosis and report lower levels of satisfaction with care. Significant disparities also exist in racial and/or ethnic and gender patient/provider concordance among racially and ethnically minoritized women with DM. 37 Future studies should examine the influence of such characteristics on diabetes-related outcomes specifically among racially and ethnically minoritized women with DM.18,20
Conclusion
Recent research shows that disparities related to perceptions of care exist among women with DM; according to the modified IMCHB18,27 this study showed how patient singularity (eg, demographic characteristics of the patient population) is associated with patient-provider interactions (eg, communication and satisfaction), and intermediate patient outcomes (eg, ratings of care received, DM self-efficacy, and DM management), with the potential of affecting even longer-term patient outcomes (eg, glucose control and improved maternal health outcomes). Specifically, given that shared decision making is linked with both diabetes care monitoring adherence and improved patient healthcare ratings in the population of interest, healthcare providers can use existing resources like telehealth to engage nonpregnant women of childbearing age in conversations to improve their health outcomes.
Footnotes
Acknowledgments
We would like to thank Dr Godfred O. Boateng at York University (Canada) for his contributions to this work.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under the Maternal and Child Health R50 MCH Secondary Data Analysis Research (SDAR) Program (1 R40MC41752-01-00).
Ethical Approval
We used publicly available de-identified data; no institutional review or approval was required to undertake this study because it did not meet the federal definition for human subjects’ research.
Statement of Human and Animal Rights
MEPS has been reviewed and approved by the Westat IRB, established under a multi-project assurance (MPA M-1531) granted by the Office for Protection from Research Risks, (OPRR). The project is reviewed and the approval renewed annually.
Statement of Informed Consent
Not applicable because the study used publicly available secondary data previously collected.
Appendix: Patient-Provider Satisfaction Questions From 2010 to 2018 Medical Expenditure Panel Survey

| Variable names | Questions |
|---|---|
| TREATM42 | Does {someone at} (PROVIDER) usually ask about prescription medications and treatments other doctors may give them? |
| EXPLOP42 | Does {a medical person at} (PROVIDER) present and explain all options to (READ NAME(S) BELOW)? |
| RESPCT42 | Thinking about the types of medical, traditional, and alternative treatments that (READ NAME(S) BELOW) (is/are) are happy with, how often does {a medical person at} (PROVIDER) show respect for these treatments? |
| DECIDE42 | If there were a choice between treatments, how often would {a medical person at} (PROVIDER) ask (READ NAME(S) BELOW) to help make the decision? |