
Abstract
Lynch syndrome (LS) is a genetic cancer syndrome that puts affected individuals at a significantly higher risk of developing multiple cancers. Participants (n = 57) were recruited through social media. Data were collected through online surveys and phone interviews; the interview data (n = 55) were analyzed to identify provider terminations and the factors that motivated these decisions. Results indicate that individuals with LS terminated their patient–provider relationships due to lack of provider LS knowledge, poor interactions, or a combination of both factors. Findings from this study suggest a need for better interactions between LS patients and providers and increased knowledge of LS-specific care.
Keywords
Introduction
Lynch syndrome (LS) is a genetic cancer syndrome that puts individuals at a considerably elevated risk of developing multiple cancers. While colorectal cancer is the most common for individuals with LS (30%-54% for women and 74%-82% for men), there also is an increased risk of stomach, small intestine, hepatobiliary tract, urinary tract, skin, brain, and pancreatic cancers (1,2). Women with LS have an elevated risk of gynecologic cancers, with a 40% to 60% lifetime risk of endometrial cancer and 10% to 15% risk of ovarian cancer (1,2).
After an individual is diagnosed through genetic testing indicating mutations in DNA mismatch repair genes (MLH1, MSH2, MSH6, and PMS2 as well as an EPCAM deletion), recommended screenings include annual or biennial colonoscopies starting around 20 to 25 years old and annual gynecologic screenings (1,3). Adherence is critical, but compliance has been less than ideal, particularly for gynecologic screenings (4). These screenings are invasive and can be uncomfortable; the complexity of screening and surveillance protocols, and the high patient burden places a high importance on these patient–provider relationships.
Individuals have reported educating their providers on LS if they did not feel confident about their providers’ LS-specific knowledge. Some patients reported feeling that their provider was not receptive to the information, while others indicated that they were satisfied with the outcome of these provider interactions (5). In some situations, a provider’s lack of understanding regarding screening and surveillance procedures as well as a low concern for LS-specific health care needs may lead a patient to terminate their patient–provider relationship. To the best of our knowledge, this study is the first to evaluate the reasons individuals with LS choose to terminate their provider relationships.
Methods
The institutional review board of Albany College of Pharmacy and Health Sciences approved this study. Participants were recruited through social media. Lynch Syndrome International, a patient advocacy organization, posted a recruitment announcement on Facebook. Individuals who were interested in participating were called by a member of the research team to confirm eligibility. Eligibility criteria included being able to read and speak English, being able to be contacted by phone and email, and having undergone genetic testing and counseling for LS. Both previvors (individuals with an LS diagnosis who have not yet had cancer) and survivors were included in this study. The first 65 eligible participants were emailed a detailed survey via REDcap (6). Upon completion of the survey (n = 57), participants were contacted for an in-depth telephone interview. There was a 96% response rate for the telephone interview (n = 55) as 2 participants could not be contacted during that time. Details of the recruitment methodology are outlined in a prior publication (7).
Descriptive analysis was conducted for the demographic data, and the interview transcripts were analyzed for indications of a change in provider. In this study, the term “providers” refers to primary care physicians, nurse practitioners, and specialists (ie, oncologists, gastroenterologists, gynecologists). For situations where there was a provider change, members of the research team (E.B. and A.B.C.) determined the primary factor driving that change. E.B. took the lead in coding these provider changes, and E.B. and A.B.C. continuously reviewed the data until determinations were made for all provider changes. Factors identified by E.B. and A.B.C. included poor interaction, lack of LS knowledge, no need for that provider any longer, change by referral, a patient or provider move, provider retirement, and insurance reasons. More than one reason was recorded per provider change, if indicated by the participant.
Results
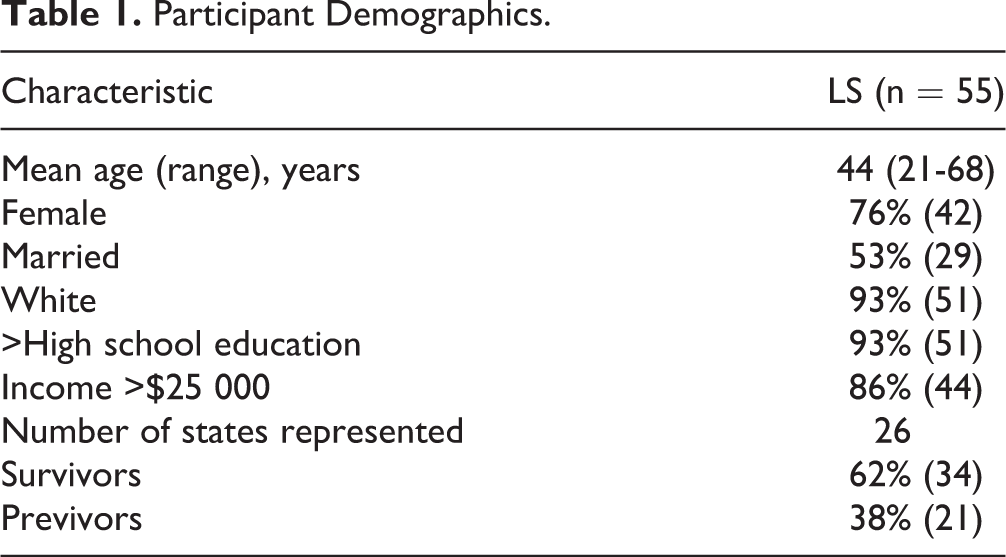
Demographic data are reported in Table 1. Transcripts were analyzed for confirmation of provider changes and reasons provided for the relationship terminations. Of 55 interviews, there were 123 indicated provider changes. Reasons given for termination of a patient–provider relationship include poor interactions (n = 15; 12.2%), lack of LS knowledge (n = 16; 13.0%), or both (n = 24; 19.5%). Some of the provider changes (n = 31; 25.2%) were due to the provider no longer being needed as part of the health care team. For example, a patient had surgery and no longer needed to see that surgeon. Insurance issues also led to provider relationship terminations (n = 8; 6.5%). Figure 1 shows the number of provider changes per factor. Excluded from Figure 1 were 3 instances of poor interactions that the participant indicated they were unable to change their provider.
Participant Demographics.
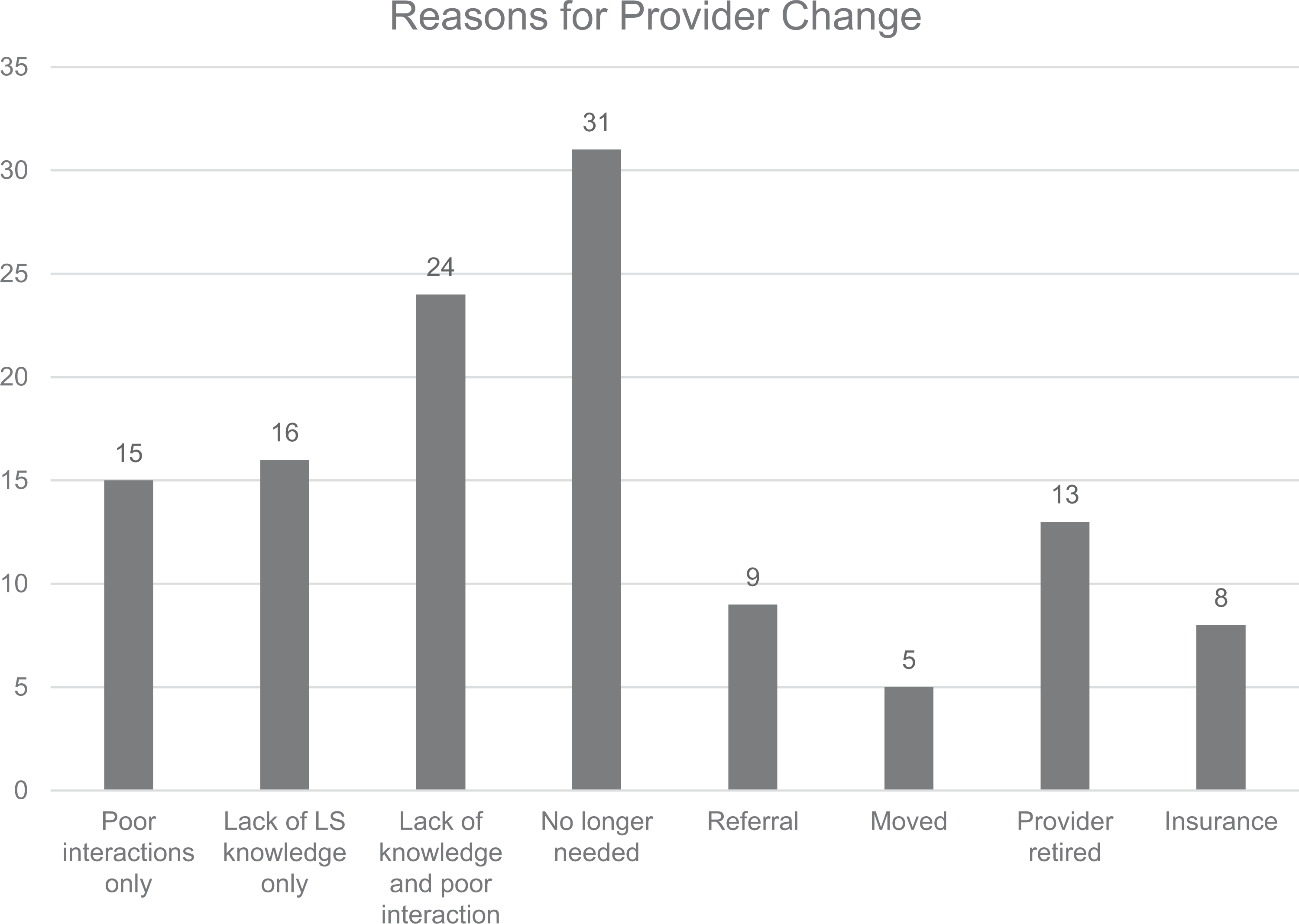
Reasons individuals with LS terminated a provider relationship. LS indicates Lynch syndrome.
These data indicate there are many reasons why individuals with LS terminate provider relationships. Of the 123 provider changes, lack of LS knowledge was indicated to be all or part of the reason in 40 of the changes (32.5%), and poor interactions for all or part of 39 of the changes (31.7%). Most of these situations overlapped, which is shown in the lack of knowledge and poor interaction column in Figure 1 (n = 24; 19.5%).
The provider interactions described by individuals with LS vary but the following demonstrate illustrative examples of each of the situations noted above. For lack of LS-specific knowledge, one participant said: “The last time I got a colonoscopy, the [doctor] told me that he never heard of…getting [endometrial or ovarian cancer] screenings on an annual basis.” For poor interaction with a provider, one participant relayed the following conversation following abnormal bleeding: “I [said] well, this isn’t normal for me. And she [says] “Oh, get over it.” She’s a GYN nurse practitioner that I’ve seen. And she [just says] “Oh, get over it. It’s just your period.” The poor interactions identified consisted of dismissive behavior, lack of consideration, general inappropriate conduct, not spending enough time with patients, and not listening to concerns; many of these interactions resulted in the patients feeling dismissed and invalidated. One participant described a poor interaction with an oncologist that she also perceived as lacking LS knowledge: “He never did any other follow-up tests [except for a breast exam]. He just asked me about my breasts and gave me a breast exam every time, and so I decided I didn’t need to see him anymore.”
Discussion
To the best of our knowledge, these data are the first to examine the factors that lead to the termination of provider relationships in individuals with LS; these data also support prior findings that LS patients face a unique set of obstacles in their provider relationships. It is evident that specific knowledge is required for proper care; when this knowledge is not adequate, the patient–provider relationship may be terminated. The considerable overlap between lack of LS knowledge and poor interaction supports the literature stating that a lack of knowledge may lead to patients educating providers or advocating for themselves in a way that is not always appreciated by providers (5). It is possible that some of these poor interactions are due to patients being more aware of their care needs and feeling that a provider is dismissing them. Participants in this study appear to have been motivated enough by unsatisfactory provider interactions to search for alternative providers who can properly handle the higher risks associated with LS. While there is no other LS-specific literature regarding provider relationships, other literature regarding conditions like HIV and diabetes, which also require specialized and detailed care, supports the idea that poor relationships decrease screening and treatment adherence (8,9). Adherence to screening and surveillance protocols for individuals with LS is imperative to detect developing cancers. Individuals with LS require highly specialized care focused on mitigating their cancer risks, which adds importance to the quality of their provider relationships.
Our results suggest that provider’s LS-specific knowledge and ability to interact effectively with patients are the most important characteristics individuals with LS consider when deciding to either maintain or terminate a provider relationship. Longitudinal studies are needed that examine changes in provider relationships over time. The literature also would benefit from having the provider perspective on these complex patient–provider relationships. Ultimately, both knowledge regarding LS and improvements in patient–provider interactions are things that can be addressed through educational intervention. The literature indicates that provider interventions that improve communication and patient-centered skills may improve patient–provider interactions (5). Since most poor interactions were due to patients feeling dismissed or invalidated, these changes could significantly improve the quality of care for individuals with LS and their satisfaction with that care.
Limitations
This study relies on 1-time, patient self-report data; it is possible that the number of provider changes are even higher than we found in our data. It also is possible that there are additional details about these changes that we were unable to document. Another limitation is that participants were recruited through social media and may not be representative of the entire LS population. Individuals who are active on a social media page for LS may be more aware of their care needs, more likely to advocate for themselves, and more likely to respond to a call for participation in a research study. As is common with hereditary cancer studies, the small sample size and lack of diversity limits the conclusions of this study; therefore, it would be beneficial to conduct a larger, longitudinal study to achieve more representative results. We were, however, able to recruit participants from 26 states who were receiving care outside of noncomprehensive cancer centers, which adds some diversity to our population. Finally, lack of LS knowledge does not refer to actual provider lack of knowledge, but only that which was perceived by patients since provider input was not included. Therefore, it is necessary in future research to get both perspectives on the termination of patient–provider relationships.
Footnotes
Authors’ Note
Data available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially supported by a grant from the Collaborative Fund of the CGA (PI: A.M. Burton-Chase.