
Abstract
Optimal information sharing between people with cystic fibrosis (PwCF), caregivers, and clinicians is key to managing CF. Based on research indicating the CF community’s interest in improved care conversations, the Cystic Fibrosis Foundation partnered with the Academy of Communication in Healthcare to customize their relationship-centered communication training program for CF and pilot the Partnership Enhancement Program (PEP). Facilitated by interprofessional certified CF clinicians, PEP consisted of a full-day workshop and follow-up session with CF care teams. Over 98% of survey responses highly rated the applicability of the skills to respond to PwCF, and caregivers needs more effectively.
Keywords
Introduction
Despite the advances in cystic fibrosis (CF) care, daily life for people with CF and caregivers remains complex, requiring them to navigate a time-intensive therapeutic regimen and a myriad of physical and psychological issues (1). Meeting the demands of CF requires people with CF and caregivers to constantly make decisions at home to continue to meet their goals. Given the major shifts in CF care in the past 2 years, including highly effective modulators (HEMT) and telehealth CF visits due to the pandemic, it is even more critical for CF care teams to understand these goals and decisions to optimize health care outcomes.
Key to this understanding is the presence of strong, bidirectional information sharing in the partnership between people with CF, caregivers, and the multidisciplinary care team (2). Research indicates that people with CF and caregivers may fear judgment or disappointment from their care team and may not be as forthcoming with concerns about managing their CF (3). Perceptions about barriers to CF care differ between people with CF, caregivers, and care teams, and, when not explored, lead to missed opportunities to improve adherence and CF outcomes (4,5). Cystic fibrosis clinicians, people with CF, and caregivers have explicitly acknowledged the value of communication training to gain skill understanding and responding to the preferences and values of people with CF and caregivers to strengthen the coproduction of CF care (3,6).
Recognizing the importance of productive patient–clinician communication to improving health outcomes and containing health care costs (7,8), organizations such as the Academy of Communication in Healthcare (ACH) developed communication training programs for clinicians (9) that are designed to increase physician and patient satisfaction, patient health outcomes, and institutional patient experience scores (10,11). The ACH relationship-centered communication training program teaches 3 skill sets (establishing trust, creating open dialogue, and setting goals by partnering) to deepen understanding about what matters to the patient and collaboratively create treatment plans (12). The skills are integrated into clinical encounters and apply to all health care professionals. Committed to addressing the needs of the CF community, the Cystic Fibrosis Foundation (CFF) partnered with ACH to customize their training program for CF and pilot the Partnership Enhancement Program (PEP). The aim of this pilot was to assess the feasibility and acceptability of a CF-tailored communication training among CF interprofessional care teams across the United States.
Methods
Partnership Enhancement Program training sessions included a 1-day in-person workshop comprised of didactics and skills practice using small group role play and a subsequent 3-month follow-up session (Figure 1). Modifications made to the ACH model included certifying interprofessional CF clinicians as facilitators of these workshops (PEP facilitators), focusing training with intact, interprofessional CF care teams, and providing post-workshop skill reinforcement. Nine CF clinicians received training and were certified by ACH faculty to deliver content and facilitate small groups. Staff from the CFF developed central logistic processes to support the care teams in preparations for the on-site training.

Pilot and evaluation design.
The PEP pilot consisted of 4 phases (A1, A2, B1, B2) throughout which PEP facilitators advanced in their development with coaching from ACH faculty to become fully autonomous at the conclusion of the pilot (3). Phases A1 and A2 were designed to test the acceptability of the CF-tailored curriculum. We tested the first version of the customized curriculum in A1 and, based on input from the PEP facilitators and participants, refined and retested the curriculum in A2. Phases B1 and B2 were designed to test the acceptability of the delivery of the trainings by PEP facilitators observed by an ACH faculty member (B1) and unaccompanied (B2). Each phase included 4 to 6 care centers of varied patient populations. We identified 19 participating centers based on their interest and previous engagement in CFF initiatives. Each center included 6 to 12 members of the clinical team (eg, physicians, nurses, nurse practitioners, respiratory therapists, physical therapists, psychologists, social workers, dietitians, pharmacists, and administrative staff) as participants. Continuing education credits were provided for participation.
Participants completed anonymous online surveys following the workshop and follow-up session to assess program acceptability and feasibility. We measured acceptability as relevance and utility of the workshop content in clinical practice, satisfaction with facilitators, and likelihood of recommending PEP to colleagues. We measured feasibility across all phases by surveying the subset of participants who assisted in preparations for the on-site training to understand the ease of identifying a date/time for each session, securing meeting rooms, and participating in planning calls. At the end of each phase, we reviewed feedback to inform refinements to the content and the delivery model using Plan-Do-Study-Act (PDSA) quality improvement techniques (13). As this pilot was classified as quality improvement, no institutional review board approval was required.
Results
A total of 210 individuals participated in 20 workshops at 19 care centers. The size of one site required 2 separate workshops. Fourteen workshops were conducted by PEP Facilitators in collaboration with ACH and 6 by PEP facilitators independently. Based on feedback from phases A1 and A2, we finalized the curriculum, shortened the 1-day workshop by 1 hour, and adjusted the format of the follow-up session from a 4-hour in-person session to a 2-hour virtual session. By the end of B1 and B2, the PEP facilitators were certified to lead the trainings independently, and we established standard central logistic processes.
Among the 149 participants who completed post-workshop surveys (71% response rate), over 98% indicated that they could use PEP in their clinical practice and would recommend it to colleagues. Participants also found the workshop to be “very helpful” and “very relevant,” with reported average scores of 4.62 and 4.70 of 5, respectively. There was a general upward trend in acceptability scores as the pilot progressed (Table 1). The PEP facilitators had an “excellent” ability to help participants learn, with a reported average score of 4.82. Nineteen follow-up sessions were completed. Participants rated follow-up sessions favorably with average scores of 4.49 and 4.75 for helpfulness and relevance, respectively. Participants involved in the planning process did not find workshop or follow-up session preparations to be difficult. Scores for workshop feasibility and facilitator follow-up training exhibited the greatest variation across pilot phases.
Response Rates, Acceptability, and Feasibility Scores by Pilot Phase and PEP Session.a
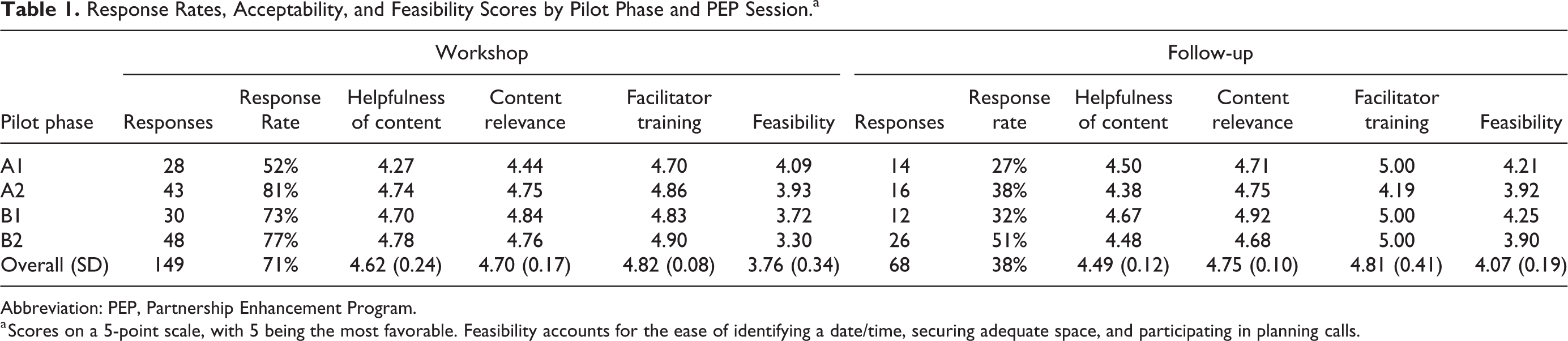
Abbreviation: PEP, Partnership Enhancement Program.
a Scores on a 5-point scale, with 5 being the most favorable. Feasibility accounts for the ease of identifying a date/time, securing adequate space, and participating in planning calls.
Qualitative results indicated that the teaching format of the small-group role play, with specialized strength-based facilitator feedback, offered individuals a safe place to practice new skills with colleagues. Participants commented that PEP “brought the whole team together on clinical reasoning and interviewing skills” and equipped them with a “common language” to use in discussions that resulted in greater understanding about the patient perspective.
Discussion
This pilot demonstrates the acceptability and feasibility of a CF-specific communication skills training program led by certified PEP facilitators, delivered to interprofessional CF care teams, and supported with central operations. Use of the PDSA methodology throughout allowed for course refinements, and acceptability scores showed an upward trend as the pilot progressed, suggesting that curriculum changes and the enhanced role of CF clinicians as facilitators bolstered the experience. Variation in facilitator follow-up training scores may be due to the timing of course refinements and ability of facilitators to familiarize themselves with changes. Although feasible, differences across pilot phases in workshop feasibility scores suggest that the ease of conducting the training is impacted by the center’s resources.
These findings suggest that this communication training provided skills to enhance information sharing between people with CF, caregivers, and care team members and among care team members. Based on these positive results, broader implementation of the PEP training program will include a larger scale rollout to all CF care centers, strategies to help clinicians embed the skills into daily CF practice, and the inclusion of more rigorous measures to assess the impact of PEP on decision-making and team care. Additional efforts will focus on supporting communication skill development for people with CF and caregivers based on expressed interest from the community (3) and from pilot care teams. These efforts will include the development of complementary resources and involvement in the care team training workshops.
Strengths of this pilot included the use of certified CF clinician facilitators who provided a positive and safe learning environment for participants and the diverse sampling of participants from multiple disciplines and care centers across the United States. Limitations of the pilot included lower-than-expected participation in survey completion and follow-up sessions, and potential skewing of data due to iterative changes to program elements.
Optimizing communication among people with CF, caregivers, and CF care teams is essential for effective partnerships in care, especially in an era of HEMT and increased telehealth clinic visits due to the pandemic. Daily life for people with CF taking HEMT looks different as patients report better health, which may result in them finding ways to simplify their treatment regimen without care team input. While telehealth offers many benefits, it requires greater focus on effective communication as patients may feel less able to share information and more disconnected from the provider (14). Given these developments, intentionally strengthening clinician communication to enhance understanding of people with CF and caregiver perspectives and incorporating them into clinical discussions is imperative to coproducing health and wellness.
Footnotes
Authors’ Note
This article does not contain any studies with human and animal subjects. Informed consent for human information to be published was not obtained because this pilot was classified as quality improvement.
Acknowledgments
The authors would like to acknowledge the Academy of Communication in Healthcare (ACH) and the ACH Faculty Leaders: Krista Hirschmann, PhD, and Robert Shochet, MD; Brandi Middour-Oxler, DNP, Carol Chace, LICSW, Elizabeth Bryson, CNP, Ferdinand Coste, DO, Michelle Prickett, MD, Staci Self, LCSW, and Susan Marshall, MD; and all participating CF care centers.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Cynthia George is an employee of the Cystic Fibrosis Foundation. Mrs. Raymond reports that during pilot activities, Katherine Raymond was employed by the Cystic Fibrosis Foundation. Lauren Collins is an employee of the Cystic Fibrosis Foundation. Zafreen Arefy is an employee of the Cystic Fibrosis Foundation. Dr. Kazmerski reports grants from the Cystic Fibrosis Foundation, grants from the Children’s Hospital Foundation, outside the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is supported by the Cystic Fibrosis Foundation.