
Abstract
Integrated and collaborative care models, in which mental/behavioral health providers work closely with primary care providers within a primary care setting, help support the quadruple aim of improved health outcomes, patient satisfaction, provider experience, and lower cost. In this paper, we describe patients’ general perspectives of integrated care and their unique experiences accessing this care within one health system. Qualitative (interviews with patients) and quantitative (surveys with patients) methods were used to collect and analyze these results separately and together. The results highlight important features to the provision of integrated care from the perspective of patients using integrated care. They include the importance and experience of access, whole-person care and a team-based approach, the availability and use of telehealth when appropriate, having high quality mental health providers, scheduling and service usage suggestions, and means to connect with longer-term services for ongoing mental health care when needed.
Introduction
The U.S. is facing a well-documented escalation in mental, emotional, and behavioral health need.1,2 Since the COVID-19 pandemic, patients lessened help-seeking behavior, with stigma prevailing as the highest barrier, 3 particularly for ethnic minorities, adolescents (especially younger men), and those in the military and health professions.4-6 Of those with a diagnosable mental illness, less than half seek treatment 4 citing limited access and difficulties navigating the mental health system. 7 The high cost of mental health services and limited insurance coverage further obstruct care. 8 Medicaid is the largest payer for mental health services in the United States; however, enrolled patients face the greatest hurdles to access due to high patient demand and low supply of providers accepting Medicaid. 9
As a result, in conjunction with other social and health-systems factors, primary care has been described as the de facto mental health system.10,11 Behavioral health is an overarching term that includes mental health and substance use conditions as well as health behaviors that impact preventive, acute, and chronic physical health conditions. Common conditions managed by behavioral health providers include depression and anxiety, but also include other mental health conditions, chronic disease management and other issues such as grief, stress, and screening for disorders such as attention deficit disorder. Up to 80% of people with a behavioral health disorder will visit a primary care provider at least once yearly, yet are often reluctant to seek mental health care. 12 Conditions that are exclusively psychological, psychiatric, or medical are rare. The most prevalent chronic medical conditions have high rates of behavioral health comorbidity. Increasingly, psychiatric disorders are diagnosed in the primary care setting 13 and expanded access to models of care that improve behavioral health access and outcomes are critical.
Integrated and collaborative care models, in which mental health providers work closely with primary care providers, help support the quadruple aim of improved health outcomes, patient satisfaction, provider experience, and lower cost.13-16 Improved access is a hallmark of integrated care and is particularly important in the pandemic aftermath.17,18 Patient perspectives are needed to inform all care models.19,20 Patient attitudes drive care seeking behavior and treatment adherence,3,21,22 consequently impacting outcomes including sustainability, expansion, and cost trajectories.23,24 Understanding patient experiences helps programs identify where to focus improvement efforts,24,25 yet patient perspectives are lacking in integrated care literature.26-28
The purpose of this paper is to describe patients’ general perspectives of integrated care and their unique experiences accessing mental health care within primary care in one health system. Patients’ perceptions about care barriers and integrated care's role in mitigating these barriers contribute to understanding which components of an integrated behavioral health care approach support a comprehensive value proposition for a patient-centered care system.
Methods
Ethical approval to report this case was granted by a local Institutional Review Board as an exempt protocol.
Colorado Integrated Behavioral Health Plus (CIBH+) Approach
The Colorado IBH + (CIBH+) approach is grounded in evidence-based foundations of collaborative care, 29 enhanced by whole-person care, and adapted to the unique needs of a clinic's population. Embedded psychologists team with psychiatrists (via telehealth) to provide both short-term patient appointments (1-6 visits) to the clinic's patients and direct support for physicians. CIBH + is designed to improve both care access and quality. Psychologists provide immediate access for services through warm hand offs (physician introduces the behavioral health provider [BHP] at the time of need during their primary care visit), crisis intervention, consultation and coordinated referrals. They offer patients diagnostic assessment and options for individual, family, couples, and group intervention. Team-based psychiatrists support primary care clinicians through interdisciplinary huddles and offer consultative patient visits for diagnostic evaluation, case conceptualization, and treatment recommendations including medication management. Digital tools, including a patient portal, facilitate communication. Patients may return for future episodes of care as indicated. When patients require long term mental health services, the CIBH + team helps establish them with community providers. A published, in-depth description of CIBH + is forthcoming.
Participants and Settings
This evaluation was conducted throughout seven family medicine clinics within one system in metro Denver, Colorado. Clinics range in size from four to 54 total full time equivalent medical providers. CIBH + began as a pilot program at one clinic in 2012 30 with six additional clinics joining by late 2020. The telepsychiatry portion of CIBH + began in 2015 and became fully staffed by 2022. Table 1 describes the patient demographics in the clinics. All BHPs in the clinics are doctorally-trained (PhD or PsyD). All psychiatrists are physicians with a MD or DO. We will use the term BHP to refer both psychologists and psychiatrists who work within clinics. The full behavioral health team includes other practitioners (eg, social workers, trainees).
Patient Descriptive Information.

*Includes 36 patients who are present in both methods.
**Based on EHR visit data from all participating practices from 7/1/2020–6/30/2023, de-duplicated at the patient level by unique patient ID.
***Not collected in EHR data.
Data Collection
Sampling: Data were collected between June and August 2022. Clinical personnel offered participation to eligible adult patients. To identify dates for research personnel to enroll patients, all 13 BHPs were asked to identify days during the sampling time frame they were present in clinic. A random number generator selected one day for recruitment from each BHP. A list of all adult patients scheduled to be seen by a BHP or trainee on the visit date, or all adult patients receiving behavioral care within a year who were scheduled for a medical visit on the day, was created to identify eligible patients. Patients were not approached for participation if their provider identified issues such as cognitive impairment or acute distress.
Procedures: On the visit day, eligible patients were first offered participation by their provider (medical or BHP) following a care visit and if accepting, introduced to the onsite research assistant. The assistant gave a brief verbal explanation of the study which included participation in a survey, interview, or both. Interested patients were given paper consent forms and provided verbal consent. Those completing the survey were sent an online link or given a paper survey. Those willing to be interviewed provided contact information and were scheduled for a phone or video interview at a later date. Patients who expressed interest but did not complete surveys or interviews received up to three email reminders.
Survey: The 41-question survey (supplemental file 1) assessed the participant's overall perception about integrated behavioral health, including barriers, benefits, and their personal experience with CIBH+. Participant demographic and background information were collected as well as current health status and quality of life using the 10-item Schwartz Outcome Scale (SOS-10). 31 Survey data were managed using the Research Electronic Data Capture (REDCap) system32,33 hosted at the University of Colorado. Participants received a $10 gift card for survey completion.
Interview: Individual 30–45 min semi-structured interviews were conducted by phone or videoconference by a researcher with qualitative training. The interview questions included the participant's conceptualization of behavioral health overall, and CIBH + specifically, including their initiation, care experience, use/non-use of telehealth, and overall satisfaction. Questions involved the perceptions of accessibility, confidentiality, prejudice, quality of care, and recommendations for improvement. Interviews were audio recorded and professionally transcribed. Participants received a $25 gift card for interview completion.
Data Analysis
Survey: Descriptive statistics were used, including mean scores for patient experience and satisfaction items and a total score for the SOS-10. A General Linear Model was used to understand variables associated with participants’ responses to the question “I would be less likely to access behavioral health care if it were not provided with primary care”. A priori variables selected were age, gender, race, and SOS-10 score.
Interviews: Transcripts were loaded into ATLAS.ti (version 9; Scientific Software Development, GmbH, Berlin, Germany). A grounded theory hermeneutic editing approach 34 was used. A coding team of two researchers and the study evaluation lead initially reviewed five transcripts together, discussing and refining themes and determining both inductive and deductive codes to be used. The remainder of transcripts were independently coded, and given a secondary review by another team member for consistency. The analysis was conducted by the two researchers who summarized quotation reports from the codes independently, then discussed and merged. Finally, one researcher read through all quotation summaries to identify the overarching themes that emerged from the interviews.
Mixed Methods: A convergent mixed methods design 35 was used for respective data from the survey results and the interviews were analyzed and described separately, and then results were integrated and analyzed together. The integration process utilized comparing (specifically matching) 36 using joint display analysis. 37
Results
A total of 55 patients completed the survey (76% of those approached), and 38 were interviewed (59% of those approached) with an overlap of 36 participants completing both methods. Table 1 includes demographic and background information for participants and for the total patient population of the seven clinics, demonstrating a representative sample. While we were unable to see full patient medical records, the top conditions patients were being seen for when they were recruited were depression (53%), anxiety (53%), stress (32%), relationship issues (15%), suicidality (15%), grief (14%), adjustment (12%), ADHD (12%), and pain (8%). The majority of patients were seen for more than one condition at the time of recruitment.
Survey results: Respondents had a mean score of 3.9 of 7 on the SOS-10, indicating moderate to high well-being at the time of survey completion (range 0.7 to 5.9; SD = 1.2). As shown in Figure 1, respondents reported positive feelings toward CIBH + generally and their CIBH + experience. The majority of participants (50-85%) responded “totally agree” with statements about CIBH + increasing access to and improving the quality of their care. Slightly over 50% agreed they would be less likely to access behavioral health if it was not provided with primary care. Findings on telehealth modality were mixed, with 41% of respondents responding “totally agree” that they prefer in-person sessions and 44% responding “totally agree” that they would prefer telehealth in the future. Open ended questions seeking suggestions for improvement mostly showed no improvement needed (mentioned 14 times) or increasing number of sessions/providing long term care (mentioned 10 times).

Behavioral health preference and satisfaction survey results (n = 55).
The General Linear Model revealed that selected participant demographics and SOS-10 scores were unrelated to the outcome of how likely participants were to access behavioral health care in the absence of CIBH + (not shown).
Interview results: Interview participants described their overall experiences with CIBH + as positive and were supportive of integrating behavioral healthcare as part of primary care. Key points and representative quotes are included in Table 2. Themes are outlined below.
Qualitative Themes and Supportive Quotes About Patient Experience of CIBH + (n = 38).
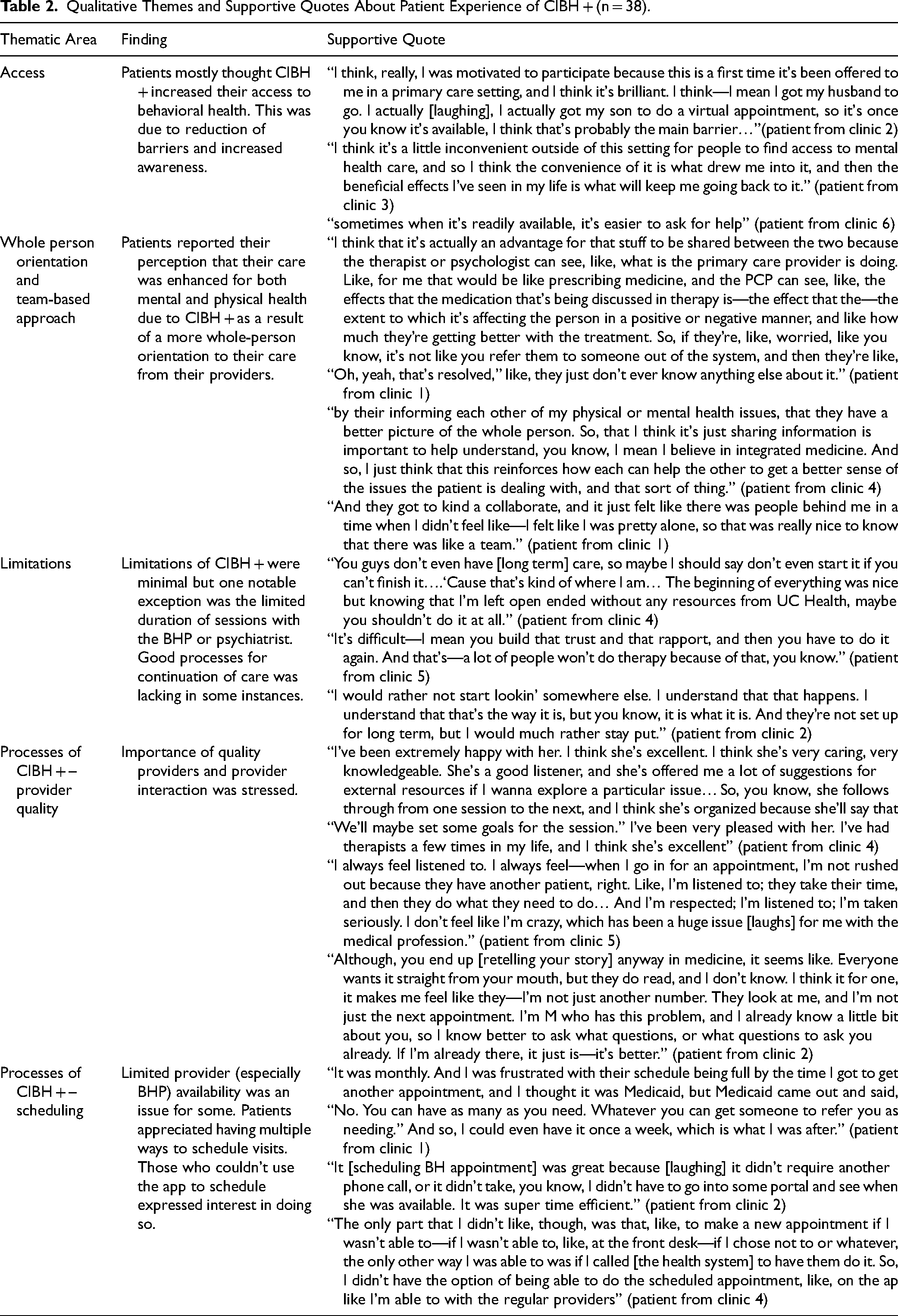
Access: Participants perceived that CIBH + increased access to behavioral health services, by enabling access to services that they previously were unable to due to personal or structural barriers, or did not know existed. Accessing behavioral health within primary care was described as convenient and changed participants’ perceptions of mental health care. CIBH + eliminated the barrier of finding a BHP. Participants considered the CIBH + BHPs as “pre-vetted” and approved by their trusted primary care team. Streamlined payment and insurance compatibility by the primary care office staff reduced financial barriers. Participants shared how having CIBH + decreased stigma by normalizing behavioral health as part of overall health care and reducing perceived public visibility (not using a mental health facility). Additionally, many participants became aware of behavioral health care by their medical provider offering services; they did not know about behavioral health care or thought it was personally irrelevant. Those who were aware of behavioral health services frequently stated that having integrated care eliminated barriers to accessing care that they would not have overcome independently; particularly because when participants are suffering and most in need of services, they are least able to navigate the often-unfamiliar community mental health care resources. Additionally, clinician encouragement to engage in behavioral health motivated participants to follow through with receiving care, revealing the importance of trusted care relationships.
Whole person orientation and team-based approach: Participants reported that CIBH + allowed all providers to work together to improve the quality of their mental, behavioral, and physical care. Participants described feeling seen as people rather than ailments (whole-person orientation to health), particularly those who felt their clinicians and BHPs had good communication with one another. Participants with complex health needs and/or were on psychotropic medications saw great benefit to CIBH+, describing how care providers communicated and worked together. Care improvements from CIBH + were seen as synergistic, not additive.
Minimal challenges for participants: Overall, there were minimal concerns with CIBH + . Aside from limited and one-off concerns about a specific BHP or scheduling challenges, most feedback was related to the short-term design of CIBH + . Although participants consented to short-term care prior to referral to CIBH+, some participants still needed long-term support and would have preferred to receive all behavioral health care needs within CIBH+, staying within their primary care setting. At the conclusion of their CIBH + episode of care, some participants who needed long-term behavioral health services relayed facing similar access challenges to those initially alleviated by CIBH + . Many interviewed participants desired ongoing care for their specific episode, either internally or in community settings. All participants hoped to maintain a relationship with their BHP in case a future need for care should arise. One participant described experiencing symptom exacerbation because the discontinuation of behavioral health services felt abrupt.
CIBH + Operations largely positive: Results for workflow and process elements such as scheduling, virtual visits, and team coordination were mixed. There was more positive than negative process feedback, but while some participants found it more convenient and quicker to schedule behavioral health visits with CIBH+, some desired more expediency and higher frequency of visits. Participant recommendations included enabling scheduling and payment via app or portal, processes already implemented in medical primary care services. All participants recommended retaining virtual visits as a scheduling option, although some preferred in-person visits. Most participants loved the coordination and communication between their providers, although a few wanted improvements.
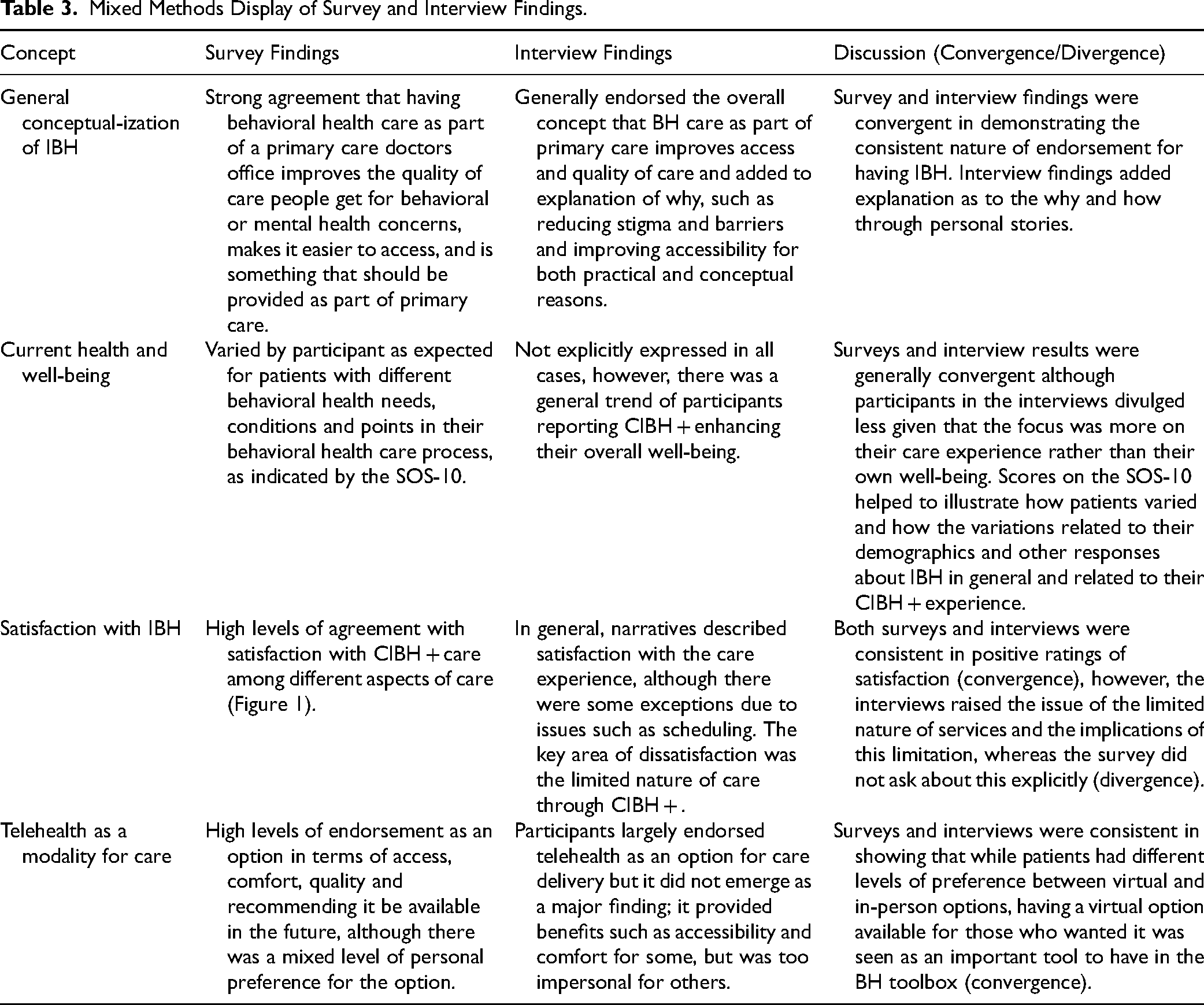
Mixed methods: Interview responses largely corroborated and expanded upon survey findings, adding detailed explanations to survey results. Mixed method integrated findings are provided in Table 3.
Mixed Methods Display of Survey and Interview Findings.
Discussion
Mixed methods results show that CIBH + effectively improved participant's perceived access to and quality of behavioral health care. Positive participant experiences echo the limited number of prior studies, 25 and recommendations about behavioral healthcare workflow add new detail to the literature. Since CIBH + offers a flexible model of care integration and is configured based on individual clinic and patient population characteristics, these details facilitate providers’ ability to implement choices for their own clinics tied directly to patient feedback.
One key finding includes the potential of CIBH + to mitigate behavioral health care access barriers. Many participants endorsed improved access due to practical and conceptual factors, including warm hand-offs from their trusted primary care clinician. Importantly, participants noted that when people need behavioral health support, they are often distressed, and have less capacity to manage access challenges. This distress may amplify perceived challenges, further impacting overall health outcomes. Well documented behavioral health care access challenges include stigma and financial barriers. CIBH + mitigated those barriers, adding support to the growing evidence for integrated models of behavioral healthcare and their ability to improve access.3,17,22,25-27
A second key finding was the perceived improvement in care quality due to coordinated whole-person care. Participants felt that CIBH + shifted providers’ views, helping to see participants as whole people rather than their presenting problems. This whole-person orientation helped participants feel care providers genuinely wanted them to be better and in turn, encouraged them to engage more in care.
Our findings mirror other reports showing that integrating behavioral healthcare supports positive patient and provider satisfaction.25,26 We received important feedback regarding CIBH + processes including recommendations to enable clinic-operated communication applications, portal-based scheduling, and payment options, and we heard the hope for longer term options for behavioral health episodes of care within primary care. More research is needed to evaluate the short-term nature of integrated care programs and the implications for patient experience. This issue is complex, as CIBH + intentionally and critically uses a short-term care approach to avoid long waitlists and enable rapid access for more patients. It is designed to expand quality coverage of mental health care within primary care. While participants were aware of service limits beforehand, results suggest difficulty with ending their episodes of care because of the positive rapport built with specific BHPs. Providers must continue to thoughtfully balance patient needs and preferences with operational limits and ongoing challenges of long-term care access. There is little existing research on this topic, 38 and it is imperative that healthcare systems continue to invest in collecting and understanding patient perspectives. Ongoing evaluation, including patient perspective, will aid in the iterative and continual improvement of integrated care delivery.
This mixed-methods study adds to the literature on the value of integrated behavioral healthcare by providing important patient perspectives. Results reveal key reasons that patients engage with behavioral healthcare and help maximize efficacy. Data described should be interpreted within study limitations, a descriptive analysis without a comparison sample. While participants were racially and ethnically representative of the clinic populations, they may not represent populations from other areas. Those surveyed and interviewed included only patients participating in CIBH + services; the perceptions of patients who could benefit from, but do not participate in, CIBH + are not represented. Due to limits of confidentiality, individual diagnoses for participants are unknown. While psychologist visits purposely exceed that of psychiatry in practice, experiences with psychiatrists were underrepresented in this data. These results represent cross-sectional data at one point in time and participants had varying length and depth of CIBH + experience. Finally, data reflect patient perceptions and not outcomes of their actual behavioral health care.
Our results demonstrate benefit of integrating behavioral care into primary care, showing the positive effect it has on patient perception of access and quality of care. This positive result may translate into increased utilization and decreased stigmatization of behavioral healthcare. Future research on specific components of the CIBH + model or other integrated care models looking for specific elements that improve access and quality, as well as which diagnoses particularly benefit, are warranted.
Conclusion
These results contribute to an improved understanding of the patient experience within an integrated behavioral healthcare approach, showing integration increases perception of access and quality of care, while having minimal challenges. CIBH + was viewed positively by participating patients, adding a patient-centered measure of value to integrated care.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241293877 - Supplemental material for Patient Perspectives of Integrated Behavioral Health in Primary Care: A Mixed Methods Analysis
Supplemental material, sj-docx-1-jpx-10.1177_23743735241293877 for Patient Perspectives of Integrated Behavioral Health in Primary Care: A Mixed Methods Analysis by Dennis Gurfinkel, Vanessa Owen, Carlee Kreisel, Patrick Hosokawa, Samantha Kluger, Courtney Legge, Jacqueline Calderone, Alisha Eskew, Maryann Waugh, Jay H Shore and Shandra M Brown Levey, Jodi Summers Holtrop in Journal of Patient Experience
Footnotes
Acknowledgements
We would like to acknowledge the full CIBH+evaluation and implementation teams at the University of Colorado and participating primary care clinics.
Author Contribution Statements
DG wrote the initial draft of the manuscript, managed revisions, and analyzed data.
VO contributed to writing and substantially editing the manuscript, collected and analyzed data, and managed the project.
CK and AE substantially edited the manuscript and collected data.
PH substantially edited the manuscript analyzed data.
SK, CL, and JC contributed to writing and substantially editing the manuscript, and were involved in project design and implementation.
MW contributed to writing and substantially editing the manuscript.
JHS and SMBL substantially edited the manuscript, conceptualized the study, and were involved in project design and implementation.
JSH contributed to writing and substantially editing the manuscript, and led evaluation efforts for the project including overseeing data collection and analysis.
Conflicts of Interest
Dr Shore is the Chief Medical Officer for AccessCare which provides telebehavioral health services in Colorado and Alaska, and receives royalties from American Psychiatric Association Press and Springer. No other authors have conflicts of interest to report.
Data Sharing Policy
The data presented in this manuscript was collected as part of an internal evaluation. We will provide anonymized individual data if requested with a valid reason, per approval of the University of Colorado, who own the data.
Ethics Statements
Ethical approval: Ethical approval to report this case was granted by the Colorado Multiple Institutes Review Board (ID 21–3917) as a Not Human Subjects Research submission. Statement of human and animal rights: All procedures in this study were conducted in accordance with the Colorado Multiple Institutes Review Board's protocols under ID 21-3917 Statement of informed consent: Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by the University of Colorado School of Medicine.
Prior Publication
This manuscript has not been published elsewhere and will not be submitted elsewhere if accepted. Portions of the data presented here were presented at the 2022 Society for Behavioral Medicine
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.