
Abstract
Patient experience is a key aspect of care quality. Since the 2007 release of the Consumer Assessment of Healthcare Providers and Systems Clinician and Group (CG-CAHPS) survey, no systematic review of factors associated with CG-CAHPS scores has been reported. We reviewed 52 peer-reviewed English language articles published in the United States using CG-CAHPS data. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines and used the Checklist for Analytical Cross-Sectional Studies. We identified several interventions (eg, adding a care coordinator focused on chronic care management) associated with improved overall provider rating and 2 interventions (eg, peer shadow coaching) that improved provider communication scores. Studies evaluating the implementation of patient-centered medical homes or patient-reported outcomes found mixed results. We identified site-level factors (eg, better team communication) and provider-level factors (eg, physician empathy) associated with better patient experience. In contrast, patient-level factors (eg, medication adherence) found mixed associations with patient experience. Policymakers, clinicians, and healthcare leaders can leverage this evidence for quality improvement efforts and interventions supporting patient-centered care.
Key Points
Our review identified several interventions (eg, adding a care coordinator focused on chronic care management) associated with improvement in overall ratings of the provider and 2 interventions (eg, peer shadow coaching) that improved provider communication.
Patient experience was inconsistently associated with patient-centered medical homes and the use of patient-reported outcomes in care.
Several site-level factors (eg, better team communication) and provider-level factors (eg, physician empathy) were associated with better patient experience. In contrast, patient-level factors (eg, medication adherence) had mixed associations with patient experience.
Introduction
Patient experience is an integral aspect of care quality and is positively associated with the performance of recommended clinical processes. 1 The Consumer Assessment of Healthcare Providers and Systems Clinician and Group (CG-CAHPS®) survey, which asks patients to report on their experiences with providers and staff in primary care and specialty care settings, was developed for public reporting, assessing the impact of care delivery interventions, facilitating patient selection of care provider, and providing actionable information to ambulatory care providers and stakeholders.2,3 Multiple versions of the CG-CAHPS survey exist.2,4–7 And they can be administered in several survey modes and languages.8–10 Survey domains include provider communication, access to care, and care coordination. Optional, supplemental CG-CAHPS survey items are available for specific topics of interest: the patient-centered medical home (PCMH), 11 health literacy, 12 health information technology, 13 cultural competence, 14 and patient narratives. 15
A recent review documented the types of studies using CG-CAHPS survey data since its 2007 release, of which 37 were cross-sectional, 9 case-control comparisons, 3 cohort studies, and 3 randomized control trials. 16 The review also found that CG-CAHPS data was used primarily to evaluate interventions (24 studies) and cross-sectional associations (21 studies), with 4 studies examining disparities in patient experience. The authors concluded that the widespread use of CG-CAHPS data indicates its value in measuring and improving care quality. They suggested that policymakers, researchers, clinicians, and healthcare leaders leverage CG-CAHPS data in quality improvement (QI) efforts and interventions that support patient-centered care. However, no systematic review has examined the evidence on associations of CG-CAHPS patient experience measures with interventions and site-level, provider-level, and patient-level factors.
We examine studies using CG-CAHPS data in the United States since 2007 to identify interventions and associations with CG-CAHPS scores. This information can help policymakers, researchers, clinicians, and healthcare leaders use CG-CAHPS survey data for QI, and interventions to improve patient-centered care.
Methods
This paper extends the systematic review of how US research has used CG-CAHPS data. 16 It identifies interventions and factors associated with patient experiences measured by CG-CAHPS data. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines17,18 and we have updated the reporting of our review based on PRISMA 202019,20 (see Supplemental Digital Content 1 for the PRISMA Checklist).
Search Strategy and Selection Criteria
We searched 6 databases (PubMed (using Ovid Medline®), Web of Science, Scopus, Cochrane Database of Systematic Reviews (CDSR) (via Wiley), American Psychological Association PsycInfo, and Cumulative Index of Nursing and Allied Health Literature (CINAHL)) using a structured search strategy involving terms including patient experience, outcomes, surveys, and CG-CAHPS to identify peer-reviewed US English-language articles published from January 1, 2007, to July 31, 2023. Two reviewers independently screened each abstract using standardized eligibility criteria to identify articles for full-text review.
We excluded articles that did not use CG-CAHPS (n = 66), only concerned the measurement properties of CAHPS surveys (n = 24), used CG-CAHPS but not as an outcome (n = 21), were not conducted in the United States (n = 10), involved only pediatric care (n = 4), were a literature review (n = 5), were before 2007 (n = 2), or were not empirical studies (ie, commentaries) (n = 14).
Data Abstraction and Quality Assessment
One reviewer reviewed and abstracted each article; another reviewed the abstracted information to ensure accuracy. Abstracted information included the study's objective, use of CG-CAHPS, study design and type, statistical methods, and main findings. 16
Most of the articles were cross-sectional, so we used the Joanna Briggs Institute (JBI) Checklist for Analytical Cross-Sectional Studies to assess study quality and risk of bias. We also excluded 12 studies because they did not possess at least 6 of the 8 JBI-Critical Appraisal Tool Checklist elements. These 12 studies reported information about exposure and outcomes but did not describe information on sample selection or did not control for confounding factors.
We grouped articles by study type (eg, intervention, association), by CG-CAHPS measure(s), and by statistical significance found (P-values < .05). We also reviewed them by year published.
Results
This search identified 210 unique articles. Following screening and full-text review, we included 52 in our synthesis. The methods, population, measures, and main topic for each included study are described elsewhere. 16 Most studies (27 of 52) involved primary care settings (either general populations, people with diabetes, or Medicare beneficiaries). Since 2012, an average of 5 studies have been published annually, 2 to 9 each year.
Overall provider rating (n = 42 studies) and the provider communication composite (n = 41) were the most commonly used CG-CAHPS measures. Access measures were also used often (n = 22), as were the global recommendation (n = 17), office staff courteousness (n = 12), and PCMH items (n = 9).
Many studies used CG-CAHPS data to assess the impact of interventions (n = 24 studies) or identify associations between patient experience and factors of interest (n = 21 studies). Six studies compared subgroups, and 1 conducted external benchmarking. Table 1 presents studies using CG-CAHPS data grouped by setting.
Included Studies’ Main Use of CG-CAHPS Survey by CG-CAHPS Measure and Grouped by Setting.
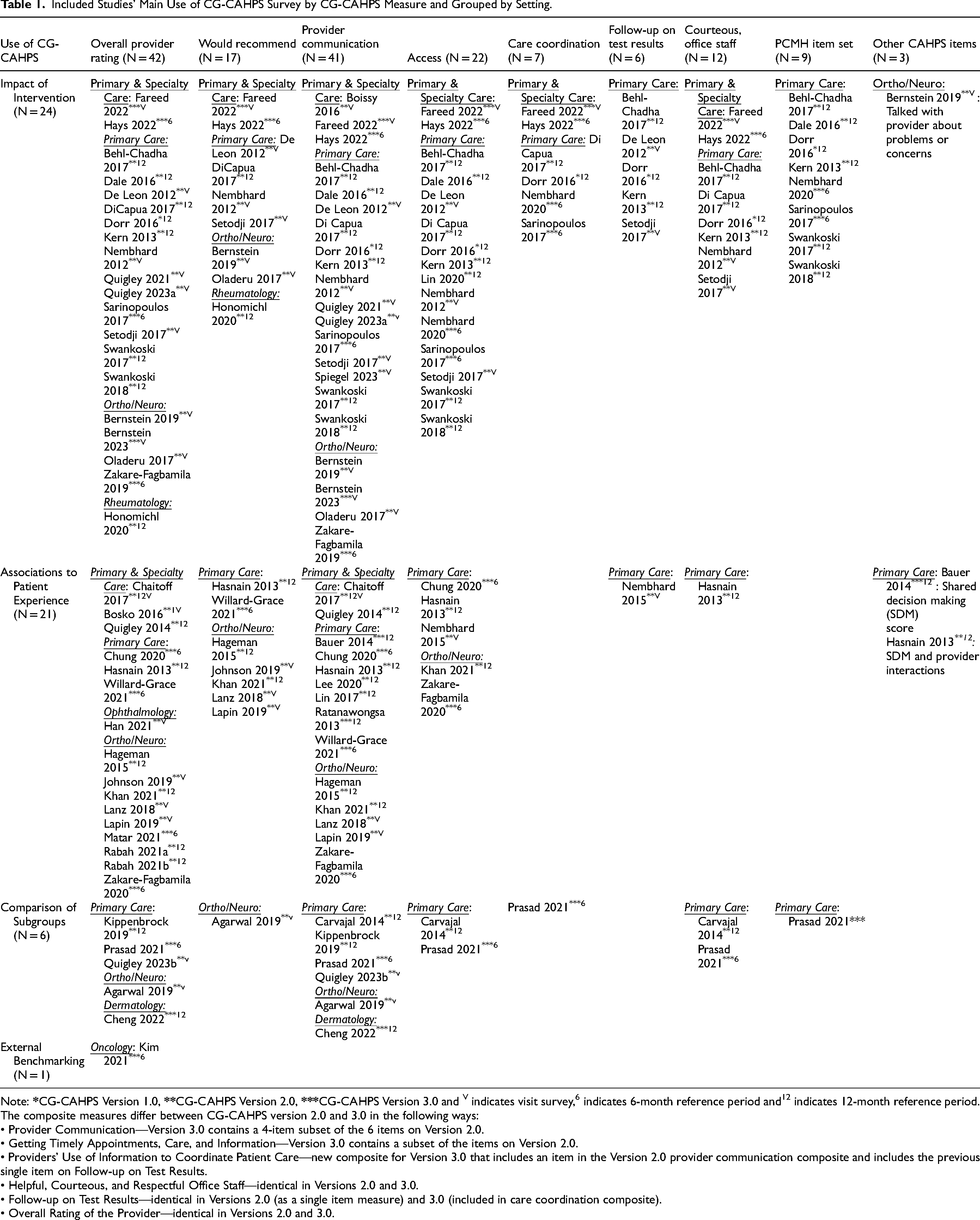
Note:
The composite measures differ between CG-CAHPS version 2.0 and 3.0 in the following ways:
• Provider Communication—Version 3.0 contains a 4-item subset of the 6 items on Version 2.0.
• Getting Timely Appointments, Care, and Information—Version 3.0 contains a subset of the items on Version 2.0.
• Providers’ Use of Information to Coordinate Patient Care—new composite for Version 3.0 that includes an item in the Version 2.0 provider communication composite and includes the previous single item on Follow-up on Test Results.
• Helpful, Courteous, and Respectful Office Staff—identical in Versions 2.0 and 3.0.
• Follow-up on Test Results—identical in Versions 2.0 (as a single item measure) and 3.0 (included in care coordination composite).
• Overall Rating of the Provider—identical in Versions 2.0 and 3.0.
Associations of Interventions With Changes in CG-CAHPS Measures
Twenty-four studies used CG-CAHPS data to assess improvement in patient experience following an intervention. Table 2 summarizes these intervention studies and the extent to which the interventions were associated with improvements. We highlight several patterns, using bold text to highlight the evaluated interventions.
Impact of Interventions on CG-CAHPS Measures, by Type of Ambulatory Care and Intervention (n = 24 Studies).
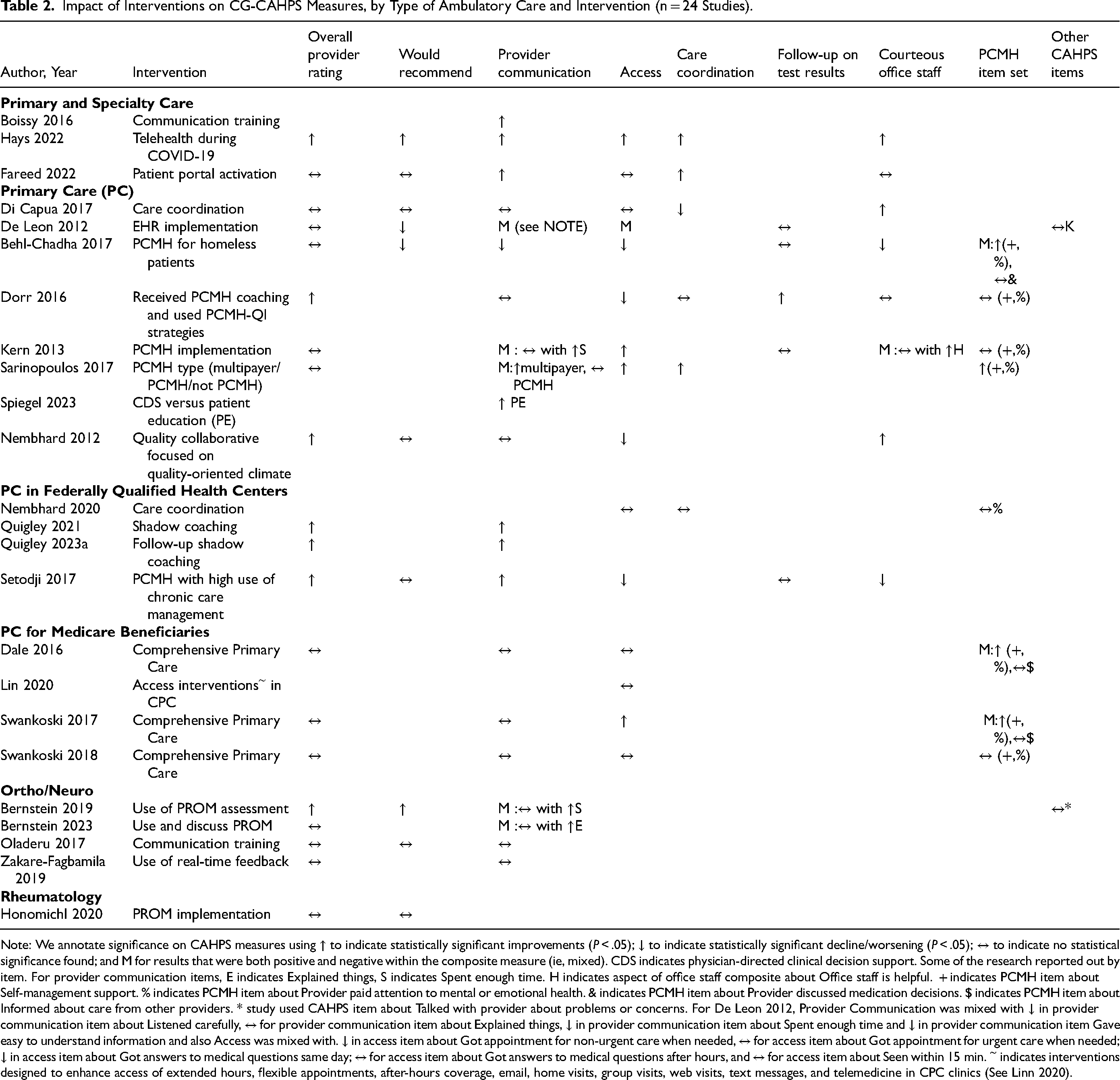
Note: We annotate significance on CAHPS measures using ↑ to indicate statistically significant improvements (P < .05); ↓ to indicate statistically significant decline/worsening (P < .05); ↔ to indicate no statistical significance found; and M for results that were both positive and negative within the composite measure (ie, mixed). CDS indicates physician-directed clinical decision support. Some of the research reported out by item. For provider communication items, E indicates Explained things, S indicates Spent enough time. H indicates aspect of office staff composite about Office staff is helpful. + indicates PCMH item about Self-management support. % indicates PCMH item about Provider paid attention to mental or emotional health. & indicates PCMH item about Provider discussed medication decisions. $ indicates PCMH item about Informed about care from other providers. * study used CAHPS item about Talked with provider about problems or concerns. For De Leon 2012, Provider Communication was mixed with ↓ in provider communication item about Listened carefully, ↔ for provider communication item about Explained things, ↓ in provider communication item about Spent enough time and ↓ in provider communication item Gave easy to understand information and also Access was mixed with. ↓ in access item about Got appointment for non-urgent care when needed, ↔ for access item about Got appointment for urgent care when needed; ↓ in access item about Got answers to medical questions same day; ↔ for access item about Got answers to medical questions after hours, and ↔ for access item about Seen within 15 min.
Interventions that Improved Overall Provider Rating. Seven interventions were associated with statistically significant improvement in overall provider rating. One of these 7 studies was also related to improving all aspects of the measured patient experience. That intervention was
Four interventions (of the 7) had statistically significant improvements in adjusted mean overall provider rating but mixed results on other measures. Primary care sites that joined QI collaboratives (such as Leading a Culture of Quality Action Group
25
) focused on improving
Furthermore, there was no significant difference in overall provider rating for several interventions. These were a
PCMH Interventions that Improved CG-CAHPS Measures. Nine studies27,28,30–34,40,41 evaluated the effect of
Three
Care Coordination Interventions that Improved CG-CAHPS Measures.
Provider Communication Interventions that Improved CG-CAHPS Measures. Regarding provider communication interventions, only
Patient Engagement Interventions that Improved CG-CAHPS Measures. Two strategies were studied to increase patient engagement in care. One study provided patients with an outpatient patient portal, providing 24/7 access to communicate with their providers and manage their healthcare; patient portal activation improved provider communication and care coordination scores but did not improve the overall provider rating, office recommendation, access, or office staff scores. 35 The dimensions of patient experience that were not improved by activated patient portal status were those that the study authors indicated were unlikely to be related to patient portal use, such as better experiences with office staff (ie, office staff courteousness scores).
The other study of patient engagement compared 2 strategies commonly used to promote appropriate opioid use for chronic pain and found that
PROMs Interventions that Improved CG-CAHPS Measures. Regarding PROMs, 2 studies found improvements with the
Cross-sectional Associations With CAHPS Measures
Twenty-one studies examined relationships of patient experience with other variables, including patient-, provider-, and site-level factors. Additionally, 1 study examined associations with survey mode 46 and several others examined which CAHPS measures are most correlated with the overall provider rating.46–49
Table 3 summarizes the 21 cross-sectional studies and the statistical associations with patient experience by CG-CAHPS measures used. We review the findings of the cross-sectional associations by site-level, provider-level, and patient-level factors, using bold text to identify the examined factor.
CG-CAHPS Measures Used in Association Studies, by Type of Ambulatory Care (n = 21 Studies).

Note: In some studies, we can also annotate significance on CAHPS measures using ↑ to indicate positive statistically significant associations (P < .05); ↓ to indicate negative statistically significant associations (P < .05); ↔ to indicate no statistical significance found; and M for results that were both positive and negative within the composite measure (ie, mixed). SDM indicates the shared decision-making item about involvement in decisions. PI indicates items about provider interactions.
Site-level factors associated with CAHPS Measures. Four studies examined site-level factors. Leader-reported
Provider-level factors associated with CG-CAHPS Measures. Seven studies examined provider-level factors. Two of these examined associations between CG-CAHPS measures and
The seventh study found that for 23 out of 28 provider ambulatory care specialties
Patient-level factors associated with CAHPS Measures. Ten studies examined patient-level factors across several care settings.
Three primary care studies were conducted in a community health center primary care setting, and 2 were specific to diabetic patients. For general primary care, the
Two studies examined the
Four studies examined patients who had lumbar surgery.
For spine surgeons in the outpatient setting, 1 study also examined the relationship between overall rating and
One study found that better patient
For ophthalmology,
Assessment of Subgroups Using CG-CAHPS Measures
Six studies used CG-CAHPS measures to assess differences by subgroups. Four of these studies found significant subgroup differences. At the site level,
There were no differences by provider–patient gender concordance in adjusted overall provider rating and adjusted scores measuring provider communication, access, care coordination, office staff courteousness, and PCMH-items about self-management support, got information about needed care on evenings/weekends/holidays, and informed about care from specialists. 72
CG-CAHPS Measures and External Benchmarking
One study conducted external benchmarking. Kim et al 2021 73 identified differences in the overall provider rating of the same provider, whether measured by CAHPS versus external physician-review websites for outpatient visits with oncology physicians; the ratings were higher for CAHPS measures.
Supplemental Table 1 provides detailed study findings for each CG-CAHPS measure and rating (see Supplemental Digital Content 2).
Discussion
This review builds on a previous systematic review, which documented the types of studies that used CG-CAHPS survey data since its inception but did not review study findings. It systematically examines the evidence on which factors are significantly associated with CG-CAHPS measures and which interventions significantly changed CG-CAHPS measures as outcomes. We identified several interventions and site-level or provider-level factors that practice leaders can implement as strategies to improve patient experience measured by CG-CAHPS.
Interventions that significantly improved the CG-CAHPS overall provider rating included participation in QI collaboratives focused on improving quality-oriented climate, implementing PCMH-specific QI strategies, increased chronic care management activities, using peer shadow coaching for providers, offering tele-video visits as an encounter option (other than office or phone visits), and performing PROMIS® assessments during routine care. Experiential relationship-centered communication skills training and peer shadow coaching significantly improved provider communication. PCMH interventions, use and discussion of patient-reported outcomes during an encounter, and care coordination interventions had mixed improvements on patient experience.
Site-level factors associated with better patient experience included better team communication. Better primary care practice team communication and increased chronic disease management activities were associated with better provider communication. Co-worker feedback on physicians’ awareness of their impact on others was associated with a higher overall provider rating, and the provider showed respect and explained things. Less in-room wait time was associated with better access scores. Less waiting room time and higher clinic-level patient volume (ie, clinic monthly total visits) were associated with better overall provider rating, access, and communication. Provider-level factors associated with better patient experience included more empathy and emotional stability. More physician empathy was associated with better provider communication, whereas the emotional stability of orthopedic surgeons was associated with higher provider ratings. Better physician performance on clinical quality measures was associated with better overall provider ratings. Provider burnout had mixed associations with patient experience and may be mediated by provider engagement in the care and treatment of their patients.
Our search focused on peer-reviewed literature with adequate study quality since we were interested in studies with broad generalizability. This approach excluded non-peer-reviewed work, such as foundation reports, single-case evaluation of QI, and other healthcare-driven patient-centered initiatives, since they are hard to publish in peer-reviewed journals but often contain helpful lessons. Future work that includes a grey literature review identifying and describing existing QI strategies for rural or small practices may help the field, as would work summarizing the evidence for interventions targeting specific CG-CAHPS domains or item sets.
This examination of research evidence using CG-CAHPS data has several implications. CG-CAHPS survey data have been consistently and widely used in research as valid measures of patient experiences of ambulatory care to assess overall care and specific aspects of care. CG-CAHPS measures are related to and reflect site changes and provider-level and patient-level factors. Importantly, CG-CAHPS measures are sensitive to changes in outcomes and associations across a wide range of ambulatory settings, including general primary and specialty care, care at community health centers (ie, FQHCs), primary care specific to diabetic patients, primary care for Medicare beneficiaries, outpatient care for orthopedic, spine and neurological surgical patients and multiple specialties (eg, Ophthalmology, Rheumatology, Dermatology). Despite this, CG-CAHPS surveys are not required by the Centers for Medicare and Medicaid Services (CMS) for performance-based payment adjustments to clinicians’ Medicare payments; however, the CMS Merit-based Incentive Payment System (MIPS) uses the CAHPS for MIPS survey, which includes the 10 core CG-CAHPS measures, as an optional quality measure. This evidence review demonstrates the broad use of CG-CAHPS survey data for measuring patient experience of ambulatory care.
Our review has limitations. First, we found inconsistent use of the same specific metrics of patient experience across the studies. There was heterogeneity across study settings (ie, about half of the studies took place in primary care settings [27 of 52]), selected outcome measures of patient experience (ie, overall provider rating was in 42 of 52 studies, whereas access scores were in 22 of 52 studies), and calculation of measure scores (ie, some studies calculated case mix adjusted mean scores while others used top-box scores), restricting our ability to perform a meta-analysis. We also by design limited our review to studies using patient's quantitative assessment of their experience using the CG-CAHPS survey data and did not include studies assessing the use of the open-ended narrative text responses from the CG-CAHPS survey, as we were assessing evidence from interventions and associations using CG-CAHPS. We have published on the potential use of CG-CAHPS open-ended responses for QI. 74 However, qualitative studies based on narrative text responses are not appropriate for understanding significant improvements related to an intervention or for assessing associated factors or directionality of findings with aspects of patient experience. Our review, however, highlighted possible interventions and factors that merit more attention based on studies using CG-CAHPS scores.
Conclusion
Since its release in 2007, the CG-CAHPS survey has been used by healthcare providers to assess a wide range of pre-post interventional changes in global ratings. CG-CAHPS data is also widely used to understand important cross-sectional relationships with patient experience of care at the site, provider, and patient levels, in addition to assessing differences across patient and provider groups. Our review identified several promising interventions and site-level or provider-level factors that practice leaders can implement to improve patient experience. Policymakers, researchers, clinicians, and healthcare leaders can leverage this evidence for QI efforts and selecting interventions that support patient-centered care.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241283204 - Supplemental material for Associations of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician and Group Survey Scores with Interventions and Site, Provider, and Patient Factors: A Systematic Review of the Evidence
Supplemental material, sj-docx-1-jpx-10.1177_23743735241283204 for Associations of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician and Group Survey Scores with Interventions and Site, Provider, and Patient Factors: A Systematic Review of the Evidence by Denise D. Quigley, Marc N. Elliott, Nabeel Qureshi, Zachary Predmore and Ron D. Hays in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735241283204 - Supplemental material for Associations of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician and Group Survey Scores with Interventions and Site, Provider, and Patient Factors: A Systematic Review of the Evidence
Supplemental material, sj-docx-2-jpx-10.1177_23743735241283204 for Associations of the Consumer Assessment of Healthcare Providers and Systems (CAHPS) Clinician and Group Survey Scores with Interventions and Site, Provider, and Patient Factors: A Systematic Review of the Evidence by Denise D. Quigley, Marc N. Elliott, Nabeel Qureshi, Zachary Predmore and Ron D. Hays in Journal of Patient Experience
Footnotes
Acknowledgements
We acknowledge the time and support of Jody Larkin who assisted with the literature searches conducted in this study and Lynn Polite for her administrative support.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a cooperative agreement from the Agency for Healthcare and Research Quality (AHRQ) (Contract number U18HS025920, U18HS029321).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.