
Abstract
Hypertensive disorders of pregnancy are a leading cause of pregnancy-related morbidity and mortality. The primary objective of this study was to compare the frequency of documentation of postpartum blood pressure through remote blood pressure monitoring with text-message delivered reminders versus office-based follow-up 7–10 days postpartum. The secondary objective was to examine barriers and facilitators of both care strategies from the perspectives of individuals who experienced a hypertensive disorder of pregnancy. We conducted a randomized controlled trial at a tertiary care academic medical center in the southeastern US with 100 postpartum individuals (50 per arm) from 2018 to 2019. Among 100 trial participants, blood pressure follow-up within 7–10 days postpartum was higher albeit not statistically significant between postpartum individuals randomized to the remote assessment intervention versus office-based standard care (absolute risk difference 18.0%, 95% CI −0.1 to 36.1%, p = 0.06). Patient-reported facilitators for remote blood pressure monitoring were maternal convenience, clarity of instructions, and reassurance from the health assessments. These positive aspects occurred alongside barriers, which included constraints due to newborn needs and the realities of daily postpartum life.
Keywords
Key Findings
The frequency of blood pressure monitoring at 7–10 days postpartum was higher albeit not statistically significant between postpartum individuals randomized to remote assessment versus office-based care (76.0% vs 58%, absolute risk difference 18.0%, 95% CI −0.1 to 36.1, p = 0.06).
Participants positively rated the postpartum blood pressure information handout and intervention text messages.
This randomized controlled trial identified facilitators and barriers to both at-home and office-based postpartum blood pressure monitoring from the perspectives of postpartum individuals who experienced a hypertensive disorder of pregnancy.
Introduction
Hypertensive disorders of pregnancy (HDP) are a leading cause of pregnancy-related morbidity and mortality, contributing to 6.3% of maternal deaths in the United States from 2017 to 2019. 1 HDP rates have risen dramatically, from 2.8% of births in 1989 to 8.2% of births in 2020. 2 Prompt recognition and treatment of HDP during the postpartum period is critical to improve clinical outcomes. 3
Guidelines recommend blood pressure (BP) evaluation with HDP within 7 to 10 days postpartum after a pregnancy complicated by HDP. 4 Despite the importance of these assessments, postpartum BP visits are not always completed. Telehealth is a promising component of postpartum services. 5 However, patient adherence varies. 6 Little is known about maternal experiences with remote BP monitoring, with one study suggesting that some individuals may feel more in control with remote monitoring while others prefer contact with a healthcare professional. 7
The primary objective of this randomized controlled trial (RCT) was to compare the frequency of documentation of postpartum blood pressure through remote monitoring with text-message delivered reminders versus office-based follow-up 7–10 days postpartum. The secondary objective was to examine barriers and facilitators of both care strategies from the perspectives of individuals who experienced a hypertensive disorder of pregnancy. Our hypothesis was that providing validated at-home BP monitoring devices at postpartum hospital discharge would increase adherence with the recommended postpartum BP evaluation.
Methods
The study was a two-arm randomized controlled trial, registered in ClinicalTrials.gov (NCT03613714). University of North Carolina at Chapel Hill Biomedical IRB approval (#18-0995) was obtained. The study was conducted at a tertiary-level hospital in the southeastern US. Prior to study enrollment, the clinical investigators (NF, AG, AMS) performed on-site and web-facilitated engagement meetings with staff at all participating clinics. Between September 2018 and November 2019, 100 individuals diagnosed with HDP who delivered at North Carolina Women's Hospital or were admitted within 3 days of delivery were enrolled. Inclusion criteria included planned postpartum care at UNC Health-affiliated facilities or clinic partners. Prior to postpartum hospital discharge, potential participants were approached, and those who enrolled were randomized to either the intervention, which entailed at-home, BP monitoring by the participants with a validated device, or standard care with an in-office BP evaluation at 7–10 days postpartum. The research team followed up with staff monthly to optimize processes for patient follow-up.
Individuals who delivered at North Carolina Women's Hospital on or after 20 weeks’ gestation, or were admitted within 3 days of delivery, were screened for inclusion criteria. Inclusion criteria were age at least 18 years, diagnosis of hypertensive disorder of pregnancy or chronic hypertension requiring medications, and able to communicate in English or Spanish. Individuals were excluded if they were less than 18 years of age, had a diagnosis of chronic hypertension not requiring medications during pregnancy or postpartum or no diagnosis of HDP, or reported that they lacked access to a cellular phone.
Potential participants were identified through Electronic Health Record (EHR) screening and approached by a research assistant (RA). After informed written consent, participants were randomly assigned 1:1 to the intervention or standard care (Figure 1). Because of the nature of the intervention, it was not blinded to participants or clinicians. All participants received the Preeclampsia Foundation “Still at Risk” handout, 8 with signs and symptoms of worsening HDP and instructions regarding management.
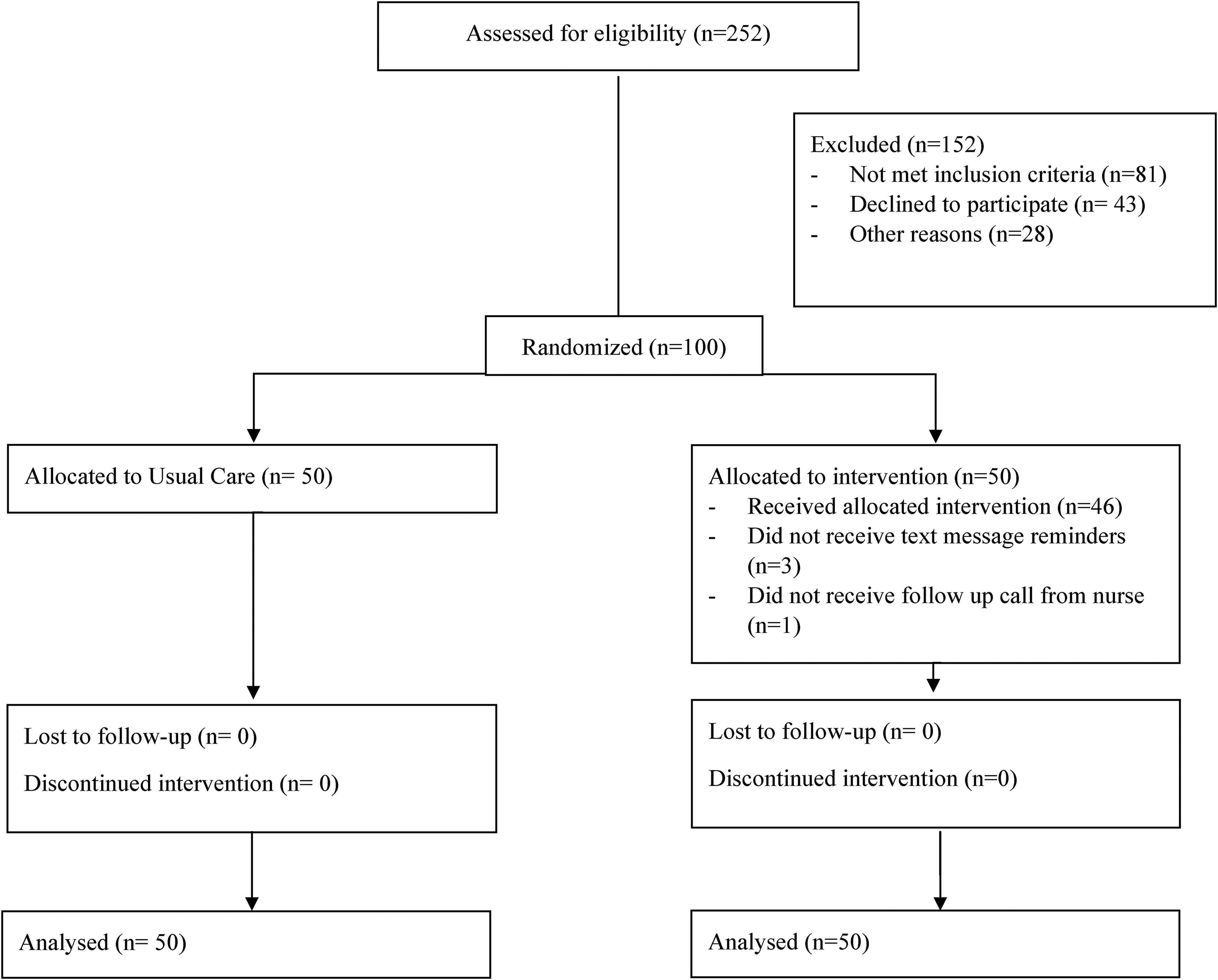
CONSORT flow diagram.
For participants allocated to the intervention, the RA provided the patient with an appropriately sized and validated digital BP cuff device (OMRON BP742N), AA-batteries, and an AC-power adapter prior to hospital discharge. Additionally, intervention participants were provided with a study handout (Appendix 1 in Supplementary Material), adapted from the “Blood pressure measurement instructions” from the American Heart Association. 9 Participants also received a paper BP log to note measurements and review during clinical follow-up assessment. The RA confirmed each participant's contact information and discussed study telephone follow-up and, for those in the intervention, text messages. Study communication and all materials were provided in English or Spanish, according to participant request.
The study team notified outpatient clinical sites when a patient enrolled. The clinicians were instructed to contact intervention participants by telephone to review their log at 7–10 days postpartum so that information could be documented in the EHR. Participants were sent one text message per day for 4 days regarding symptoms of worsening HDP and prompting BP self-assessment, with their clinic phone number embedded in two of the text messages (Appendix 2 in Supplementary Material). The texts were one-way and sent through the software program Qualtrics.
For participants allocated to standard care, their clinic was notified of the need for 7–10 day blood pressure check, which staff contacted the patient to schedule. At the visit, the participants’ BP levels was assessed and recorded in the EHR. For all participants, signs and symptoms of worsening HDP or persistent severe-range BP were discussed with a supervising member of their health care team (physician, certified nurse-midwife, or nurse practitioner) as part of standard care.
The primary study outcome was the proportion of participants who underwent a BP evaluation at 7–10 days postpartum that was documented in the EHR. The secondary outcome was birthing parent acceptability of the postpartum BP care strategies, assessed through their accounts of facilitators and barriers of at-home or in-office evaluation. Fifty of the 100 participants were invited to complete a semi-structured telephone interview around 2 weeks postpartum to explore their experiences with the intervention (n = 26) or with standard care (n = 24). The interview guide (Appendix 3 in Supplementary Material) included closed-response questions regarding health and clinical experiences, with a Likert-scale of 1 = poor to 5 = excellent, and open-ended questions about postpartum recovery and BP monitoring. Audio files were professionally transcribed and translated into English, as applicable, and de-identified. Transcriptions were reviewed for accuracy and completeness.
Descriptive statistics included chi-square and t-tests for categorical and continuous variables respectively and were used to compare study outcomes by study arm. In analyses of births at the study site before the study period (July 2014 and June 2016), 20% of postpartum individuals with HDP had a BP assessment within 7–10 days postpartum. An a priori sample size of 100 patients (50 patients per arm) provided 80% power to detect a hypothesized improvement from 20% to at least 50%, with a 0.05 two-sided significance level and accounting for 20% loss to follow-up. Given this was a randomized trial, statistical adjustment for baseline covariates was not performed. SAS 9.4 was used for quantitative analysis. A p-value threshold of p < 0.05 was used to interpret statistically significant results.
Qualitative analysis was used to identify facilitators and barriers of blood pressure monitoring from the perspectives of postpartum individuals. An inductive approach meant that codes were constructed and finalized from patients’ experiences, 10 to address the knowledge, feelings, and practices they described as being important for at-home or office-based assessment. Transcribed responses were read in their entirety for initial familiarization. Then, two authors (a non-clinician researcher and a medical student) independently conducted thematic content coding. 10 Similar keywords and phrases were grouped into categories with memos. A collaborative selective coding process was used to cluster categories into themes, with consensus reached through review and discussion.
Results
Participants were in average 29.7 years of age, with 43.0% being first-time mothers, 28.1% self-identified as non-Hispanic Black, 22.9% self-identified as Hispanic, and 11.3% were Spanish-speaking (Table 1). About half of the individuals had public or no insurance (52.1%). Participant characteristics were balanced between the intervention and standard care arms (p > 0.05), except for hospital discharge on antihypertensive medication (36.0% intervention vs 16.0% standard; p = 0.02).
Participant Characteristics Overall and by Randomized Trial Arm.

Note. Categorical variables were compared with chi-square test and continuous variables with Student T-test.
The proportion of documented BP evaluation at 7–10 days postpartum was higher in the intervention compared to standard care (Table 2, 76.0% vs 58.0%, absolute risk difference 18.0%, 95% CI −0.1 to 36.1%), but the difference was not statistically significant (chi square p = 0.06). Individuals enrolled in the study were more likely to undergo postpartum BP evaluation (67.0% overall) than observed prior to the project (20%).
Study Outcomes Overall and by Randomized Trial Arm.

Note. *Postpartum acute care utilization included experiences of chest pain that resulted in ambulance transport, blurry vision and headaches that led to an in-office clinic evaluation and hospital readmission, and another individual was passing “a lot of blood clots” in the neonatal intensive care unit. The participant went from that unit to labor and delivery triage, which led to diagnosis of an infection.
In the intervention arm, text messages were successfully sent to 48 of the 50 participants. Although participants were informed by the research team that texts were one-way, some participants responded to study message with “ok” (one English-speaking and three Spanish-speaking), and one participated replied with their BP levels (English-speaking).
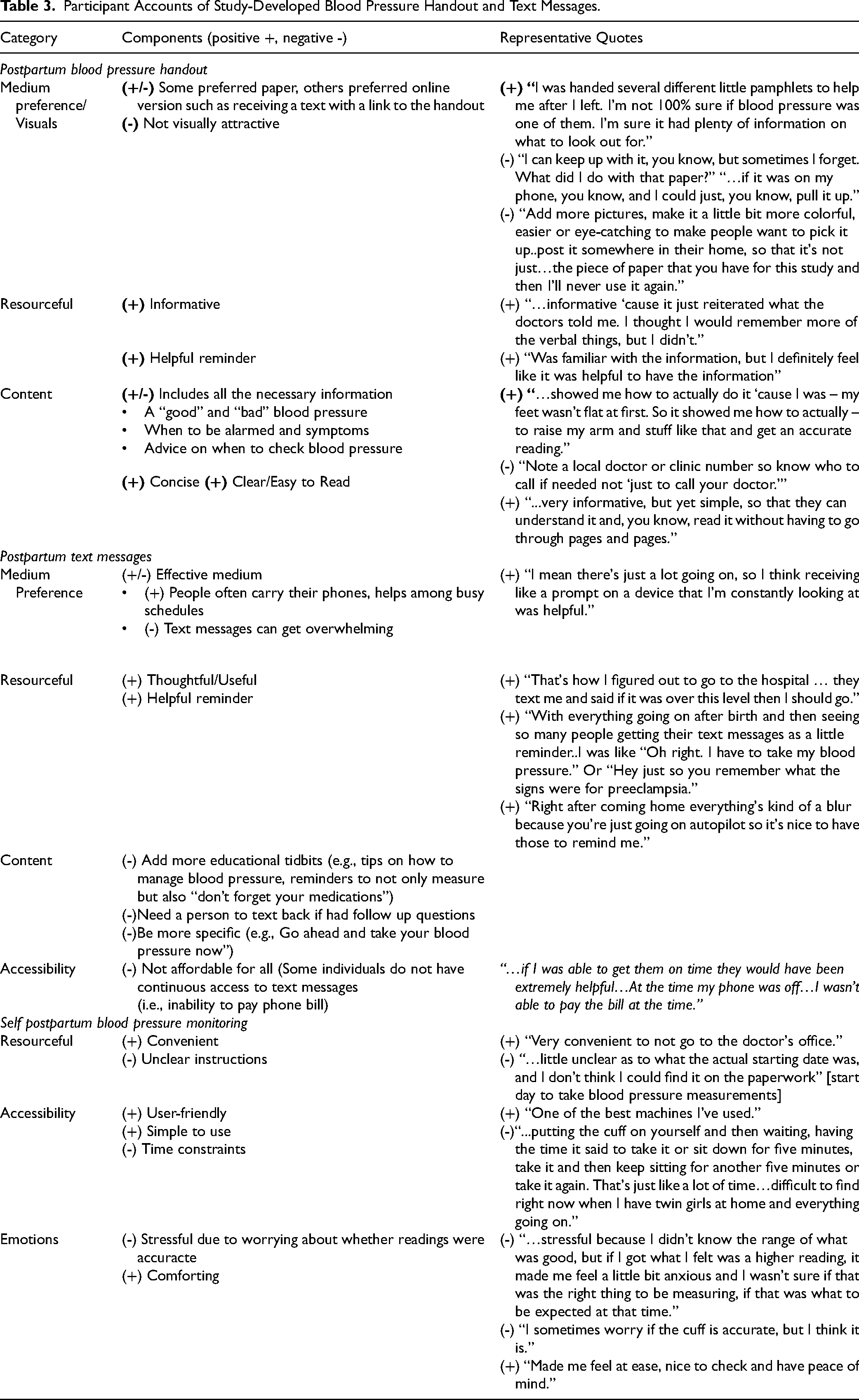
Participants rated their health care experiences and the study materials positively (Appendix 4 in Supplementary Material). All the interviewed participants in the intervention reported evaluating their BP at home. Additionally, a 6/24 (25.0%) of the interviewed participants in standard care reported home BP monitoring, which they conducted with their own devices outside of the study. Participant accounts suggested remote BP monitoring was acceptable (Table 3), with themes of (1) maternal convenience coupled with uncertainty, (2) inadequate access to postpartum health information, and (3) determining the need for acute care utilization, which occurred (4) in the context of their daily postpartum lives described below.
Participant Accounts of Study-Developed Blood Pressure Handout and Text Messages.
Maternal Convenience Coupled with Uncertainty
At-home BP monitoring was described as a simple technical process that participants valued being able to do at their convenience. Some were accustomed to completing home BP evaluations because of self-monitoring during the study pregnancy or with previous pregnancies. Access to at-home BP monitoring was reassuring to participants, particularly since some knew that hypertension could worsen following childbirth. A participant described being vigilant of potential complications and BP thresholds since postpartum “doesn't mean the switch was flipped and I necessarily was out of the woods for preeclampsia.”
At-Home Monitoring Permitted Individuals to “Keep an eye on” their BP Levels
It was important for them to be able to check when feeling “really off” or when experiencing symptoms. Yet, not all participants had clarity on maternal health warning signs. One participant was readmitted to the hospital and recounted surprise at being asked about symptoms that they had experienced but did not realize were problematic at the time. Another did not know if their post-discharge headaches were a side effect of an epidural or related to elevated BP. Although participants generally described that home monitoring itself as feasible, easy, and helpful, one participant worried about whether the cuff readings were accurate. Further, the BP level threshold for concern was not always clear. Some anticipated readings would “bounce around” as part of regulation. For others, BP fluctuation could cause distress. Additionally, a Spanish-speaking participant with standard care was worried about their BP and was waiting on a call to schedule an appointment.
Inadequate Access to Postpartum Health Information
Participant readiness to recognize and respond to BP levels was positioned in relation to inpatient health education. They reported need for being more equipped to know what to expect and when to call clinicians, and they said that reading a handout on postpartum blood pressure did not provide adequate depth. Further, their experience of inpatient care as rushed, with health care team members in their room like a “revolving door” undermined their hospital discharge care planning. One English-speaking participant was not aware of the possibility of postpartum preeclampsia until after they experienced a hypertensive crisis. Although in the intervention, the participant did not receive the study text messages because their phone line was inactive due to financial constraints.
Determining the Need for Acute Care Utilization
Participants assessed their health and health care needs based on their BP levels and symptoms. An intervention participant shared gratitude for detecting high BP levels with at-home monitoring. The participant had felt “normal” but realized, one evening, that their readings were “very high,” so they sought emergency care. The study text messages kept them “on track.” Another participant described feeling unwell and internally debating whether they needed acute care, since there were various contributors to how they were feeling: I was thinking some things because I was going to pay bills that I had to pay and I was not going to have enough money…and since my kids were being mischievous, they were throwing toys, there was noise and all, it was as if my ears – I don’t know what happened, they were as if – nerves I think. So, I got scared and said, well, “Why is this happening to me?” My heart started beating really fast, too fast…I grabbed some cold water and placed it over my face, my back, and then I controlled myself. I was starting to feel better and when my daughter came home, because I was all alone with my kids and my daughter arrived, so I said to her: “I’m going to head to the hospital because this happened, what if there is a problem and I better go and get checked to get rid of the doubt.” So, I went to the emergency room. (Standard care, Spanish-speaking)
One of the participants who experienced readmission suggested that her BP management could have been more proactive. The participant felt like if they had been prescribed medication postpartum, their levels would have been more controlled and they would not have had to go to the hospital, where they then received medication. In contrast, another participant did not answer a follow-up call because they felt well.
The Context of Daily Postpartum Life
Maternal postpartum overwhelm meant that BP information could get “pushed to the side.” The individuals described a “rollercoaster of adapting to the new mom life.” This “hard transition” included recovery from childbirth, navigating health complications, shifts in weight, learning infant needs, and establishing breastfeeding, including in relation to medication side-effects. Overall, “getting into the groove” occurred with a focus on the infant and necessitated strong maternal “willpower to carry on.” Participants recommended texting a digital copy of the BP handout to have it more readily available. Another participant reflected, “I don't think there's a problem with the [study] handout. It's more having two kids.”
Support from loved ones, including with food, was important for participants to “try to follow recovery guidelines” such as resting. Additional postpartum challenges included stress from the system of insurance coverage (eg, paying out of pocket while Medicaid was not yet active for the infant), transportation challenges (from weather, finding a ride, and car service needs), and financial stress. Additionally, maternal sleep was a specific challenge that impacted their emotional and physical health, including BP levels. A participant framed their readings in relation to “having no sleep” and wished their health could be “separated from sleep.” Others said they assumed their headaches and lightheadedness were due to fatigue. When the symptoms “wasn’t so much or so bad” they did not call. Overall, BP problems in addition to postpartum strains were “really exhausting, worrisome – it was very stressful.”
Discussion
In this randomized clinical trial of at-home versus in-office postpartum BP monitoring, we found that at-home BP monitoring was an effective and acceptable monitoring modality for postpartum individuals who had experienced a hypertensive disorder of pregnancy. Qualitative analyses revealed patient satisfaction consistent with previous research 11 as well as opportunities for strengthening postpartum blood management, including the provision of more relevant inpatient health information and education. Text messages were acceptable to patients for blood pressure assessment reminders in the postpartum period.
Participants positively rated the postpartum BP information handout and intervention text messages. Overall, at-home postpartum BP monitoring was helpful to better align postpartum health needs with patient-focused, timely services. The self-assessments identified health problems for some and offered reassurance for others, as part of a complex and sometimes worrisome process of disentangling postpartum symptom overlap following a HDP.
Qualitative analyses revealed that enhanced care in the control arm occurred on the individual-level, with patients receiving more verbal communication and written health information around postpartum BP, and on the systems-level, as study personnel elevated the importance of postpartum BP assessment and coordinated the office-visits as part of standard care for study participants. The higher rates of postpartum BP documentation in both trial arms compared to the previous rate at the study setting limited our statistical ability to evaluate group differences between postpartum blood pressure approaches. However, the 18% absolute difference in BP evaluation rates (95% CI −0.1 to 36.1%) is clinically meaningful, and consistent with previous studies evaluating post-discharge remote BP monitoring. 5
Particularly since the COVID-19 pandemic, at-home BP monitoring has been found to be an effective way of meeting current clinical guidelines for postpartum BP.5,12 Our results extend these findings and qualitative work.7,11 Participants took their BP when they felt fine in response to study prompts, which in at least one case led to acute care utilization and treatment. Routine, at-home BP postpartum assessments may enable detection of hypertensive problems that might otherwise be unrecognized and untreated. Efforts are underway from both Medicaid and commercial insurers to finance remote patient blood pressure monitoring, given the potential to decrease maternal morbidity and reduce healthcare costs. 13
Multiple participants described a need for more preparation to monitor and manage their postpartum blood pressure, specifically to alleviate worry about cuff accuracy and to help disentangle health complications in the context of postpartum fatigue and BP normalization. Participant experiences in this study included the inability to receive texts due to the loss of cellular service and individuals not answering follow-up calls because of feeling well. When health care communication is conducted via telephone/ texting, it may be helpful to proactively address potential patient gaps in coverage due to their financial barriers. Further, patients may not answer when they feel well. These results suggest that it is important for health care professionals to understand that recommended patient practices may seem easy, but people's ability to adhere to guidance can be limited because of the reality of their daily lives and lack of access to relevant health information. In addition to remote blood pressure monitoring as investigated in this research, the ability for postpartum individuals to engage in other supportive practices such as taking their medications as prescribed warrant attention.
Limitations
Study strengths included mixed methods, with EHR evaluation and patient-reported closed-response and open-ended accounts of intervention and standard care. Limitations include study conducted with participants who gave birth or were admitted within 3 days postpartum of a single site. The multifaceted study approach to coordinate patient engagement across a range of postpartum ambulatory care sites meant that more attention and perhaps more quality care was offered to standard care participants. This aspect of the study, along with the increased attention and resources to postpartum blood pressure, may have increased blood pressure evaluation in the standard care group through both self-monitoring at home with their own devices and office-based care. The enhanced standard may have limited our ability to test our hypothesis between remote monitoring and office based care. The generalizability of the findings is limited by the study being conducted before the COVID-19 pandemic, which increased access to and familiarity with remote BP monitoring. Further, the sample was relatively highly educated. We were not able to disaggregate data by this variable or others such as maternal race-ethnicity, language, or payor status. These variables are associated with access to postpartum care 14 and so are important to inform future strategies and research.
Conclusion
In this RCT of individuals who had experienced a HDP, there were no significant differences in the rate of clinically documented BP monitoring at 7–10 days postpartum between those randomized to remote assessment versus office-based care. Remote BP monitoring in the postpartum period was feasible and important to birthing parents, but provision of a monitor with instructions and texted reminders was not sufficient support. Patient access to tailored information, timely care, medication titration, and overall postpartum support are areas to address alongside innovations with health monitoring.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241272217 - Supplemental material for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy
Supplemental material, sj-docx-1-jpx-10.1177_23743735241272217 for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy by Kristin P. Tully, Sonum Tharwani, Kartik K. Venkatesh, Laarni Lapat, Narges Farahi, Angelica Glover and Alison M. Stuebe in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735241272217 - Supplemental material for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy
Supplemental material, sj-docx-2-jpx-10.1177_23743735241272217 for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy by Kristin P. Tully, Sonum Tharwani, Kartik K. Venkatesh, Laarni Lapat, Narges Farahi, Angelica Glover and Alison M. Stuebe in Journal of Patient Experience
Supplemental Material
sj-docx-3-jpx-10.1177_23743735241272217 - Supplemental material for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy
Supplemental material, sj-docx-3-jpx-10.1177_23743735241272217 for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy by Kristin P. Tully, Sonum Tharwani, Kartik K. Venkatesh, Laarni Lapat, Narges Farahi, Angelica Glover and Alison M. Stuebe in Journal of Patient Experience
Supplemental Material
sj-docx-4-jpx-10.1177_23743735241272217 - Supplemental material for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy
Supplemental material, sj-docx-4-jpx-10.1177_23743735241272217 for Birthing Parent Experiences of Postpartum at-Home Blood Pressure Monitoring Versus Office-Based Follow up After Diagnosis of Hypertensive Disorders of Pregnancy by Kristin P. Tully, Sonum Tharwani, Kartik K. Venkatesh, Laarni Lapat, Narges Farahi, Angelica Glover and Alison M. Stuebe in Journal of Patient Experience
Footnotes
Acknowledgment
The authors thank participants for their time and willingness to contribute. We are also appreciative of Catalina Montiel's editorial contributions.
Contribution List
Kristin Tully contributed to data acquisition, data curation, investigation, supervision, formal analysis, data validation, and writing both the original draft and writing-review and editing. Sonum Tharwani contributed to formal analysis, writing-original draft, and writing-review and editing. Kartik Venkatesh contributed to formal analysis, data validation, and writing-review and editing. Laarni Lapat contributed to data acquisition and writing-review and editing. Narges Farahi contributed to conceptualization, funding acquisition, investigation, methodology development, project administration, and writing-review and editing. Angelica Glover contributed to conceptualization, funding acquisition, investigation, methodology development, project administration, and writing-review and editing. Alison Stuebe contributed to conceptualization, funding acquisition, investigation, methodology development, project administration, resources, supervision, data validation, and writing-review and editing. All authors approved the writing for publication.
Conflict of Interest Statements
Drs. Tully and Stuebe are inventors on a patented medical device. The University of North Carolina at Chapel Hill intellectual property is licensed. The device is not referenced or otherwise related to the content of this manuscript. The other authors report no conflicts of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the UNC Center for Health Innovation. The funding organization was not involved in the data collection, analysis, and interpretation or the preparation of the manuscript and has no right to approve or disapprove publication of the finished manuscript. The authors are solely responsible for this document's contents, findings, and conclusions.
Ethical Approval
University of North Carolina at Chapel Hill Biomedical IRB approval (#18-0995) was obtained.
Grant Number
Not numbered.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the University of North Carolina at Chapel Hill Biomedical IRB approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.