
Abstract
To identify medical phrases utilized by the critical care team that may have an unintended impact on the critically ill patient, we administered an anonymous survey to multi-professional critical care team members. We elicited examples of imprecise language that may have a negative emotional impact on the critically ill. Of the 1600 providers surveyed, 265 offered 1379 examples (912 unique) which were clustered into 5 categories. Medical jargon (eg, “riding the vent”) was most prevalent (n = 549). There were 217 negative suggestions (eg, “you will feel a stick and a burn”). Hyperboles (eg, “black cloud”) were common (n = 198) while homonyms (ie “he fibbed”) accounted for 150 examples. Phrases such as “code brown in there” were categorized as metonyms (n = 144). 121 metaphors/similes (eg, “rearranging deck chairs on the Titanic”) were provided. Phrases that have the potential to negatively impact critically ill patient perceptions are commonplace in critical care practice. Whether these everyday communication habits lead to an unintended nocebo effect on mental health outcomes of the critically ill deserves further study.
Introduction
“Words kill, words give life; they’re either poison or fruit—you choose.” – Solomon
The power of language stems from one of the first senses human fetuses develop—hearing. 1 Ability to process speech seems to be preserved even in the most unlikely situations including minimally conscious state, coma, traumatic brain injury, and deep sedation.2–6 The language spoken around critically ill patients therefore can be both impactful and saved in their long-term memory despite their overt lack of awareness. The “nocebo effect,” well described in non-critically ill patients, is a phenomenon whereby negative expectations can lead to negative outcomes. 7 The pain literature includes many examples of socially transmitted nocebo effects8,9 including a report on how manipulating providers’ expectations directly impacts patients’ subjective experiences of pain. 10 This suggests that provider expectations and communication style can directly influence patient outcomes. Hospitalized and critically ill patients may experience nocebo effect from limited or poor communication, including the use of unintentional negative suggestions by physicians and nurses,11,12 Common medical jargon may also contribute to patient confusion and affect health outcomes. 13 For example, everyday expressions used by the medical team (eg, “she is trying to die on us”) may reflect a subconscious provider construct in which the doctor–patient relationship is viewed as antagonistic, setting the stage for negative expectations. 14 Previously, the hidden impact of imprecise language has been described in the ICU in context of consent process (description of risks leading to increased fear, anxiety and subsequently harm), invasive procedures (negative suggestions such as “pain” and “sting” resulting in hyperalgesia and distress), and family meetings (using phrases such as “withdrawal of care” or “limitation of treatment”). 15 Interviews with critical illness survivors who remembered their intensive care unit (ICU) stay revealed that “communication” exchanges, for example, when ICU team members talked “over” patients, made distressing remarks in their presence, or failed to inform them about ICU-related care, resulted in patients feeling dehumanized, losing trust in the medical team and motivation to participate in their ICU recovery, as well as feelings of distress, guilt, depression, and anxiety. 16
Increasing awareness of language in critical care is particularly important, as the impact of words may be the most consequential in this setting since memories of frightening and delusional experiences from the ICU stay are strong and potentially modifiable risk factors for substantial psychiatric morbidity in this population.17–22 The extent of medical jargon and figurative (imprecise) language use in critical care is currently not known. Therefore, the aim of this study was to identify common phrases used and heard in the ICU setting that may have an unintended nocebo effect on critically ill patients.
Methods
We surveyed critical care attending physicians and trainees, advanced practice providers, bedside nurses, chaplains, social workers, physical, speech, and occupational therapists across several ICU settings at a large U.S. tertiary care center. The survey and study protocol was reviewed and deemed exempt by the Mayo Clinic Institutional Review Board (IRB). As such, informed consent was not required, and a response to the survey constituted agreement to participate in the study. Participants were notified that responding was completely voluntary and would not impact employment.
To develop the survey questions, LK, LW, DS, KP, JC, OG, MW, ES, DP, and KV reviewed available literature and discussed the most common phrases that may be misunderstood by someone outside the medical field or in an altered state to determine potential categories of imprecise language. Others proposed an excellent system for classification of medical jargon (technical terminology, alphabet soup, medical vernacular, medicalized English, unnecessary synonyms, euphemisms, and judgmental jargon). 23 In reviewing common examples from critical care practice we recognized that many other forms of imprecise language were also commonly employed and therefore decided to broaden our inclusion categories. We defined “medical jargon” as language used by a particular group or profession that is difficult for others to understand (eg, “float a swan”, “occult blood loss”); its untoward impact on patient-provider relationship has been well described.13,23,24 “Negative suggestion” included any phrase that primed an individual to expect a negative experience, such as “rate your pain,” “you will feel a stick and a burn,” “he can die at any time”.11,15 “Metaphors” and “similes” were defined as figures of speech that are applied to an object or action which is not literally applicable (eg, “your mother is a vegetable” and “big gun antibiotics”).25,26 “Metonyms” are figures of speech where a concept is referred to by the name of something closely associated (“I just have admitted an interesting sepsis”, “the hernia ate breakfast”). 27 It was less clear whether to create separate categories for “homonyms” or phrases that can have multiple meaning (eg, “patient eloped”, “sundowning”) and for exaggerated statements or “hyperboles” such as “he is trying to die on us” and “the RRT (rapid response team) is coming in hot”. We decided to keep these separate to have a broader range of responses from survey participants. The final survey included eight questions with multiple choice and open-ended formats; examples were provided for each category (see Supplemental Table S1).
Questionnaires were sent using the REDCap online survey database (Nashville, 2020) to ICU stakeholders working across two medical, two surgical, and one combined medical/surgical ICU. Potential participants were identified through their respective department's email distribution list. Each participant received a unique link which was de-activated once that individual's survey was completed. A reminder email was sent to those who did not respond after one week. Data were collected between May 17 and June 9, 2021.
All responses were reviewed by the investigators (LK, AN, LW, IRG) and types of imprecise language grouped using the abovementioned definitions. Responses were recategorized when necessary to create a library of the most commonly used phrases that may have an unintended nocebo effect in the critical care setting.
Results
The survey was sent to 1600 interprofessional critical care team members, and was completed by 265 individuals (17% response rate). Stakeholders with the highest response rate were registered nurses (40%), followed by critical care attending physicians (20%), advanced practice providers (13%), respiratory therapists (7%), occupational therapists (7%), and physical therapists (5%). Stakeholders with the lowest response rate were social workers (0.4%), chaplains (2%), speech language pathologists (3%), and fellows (3%) (Figure 1). Provided responses captured 1379 examples (912 unique) of imprecise language common in the ICU setting. Representative quotes that are suitable for publication are displayed in Table 1.

Breakdown of responses by care team member group.
Key Quotes.
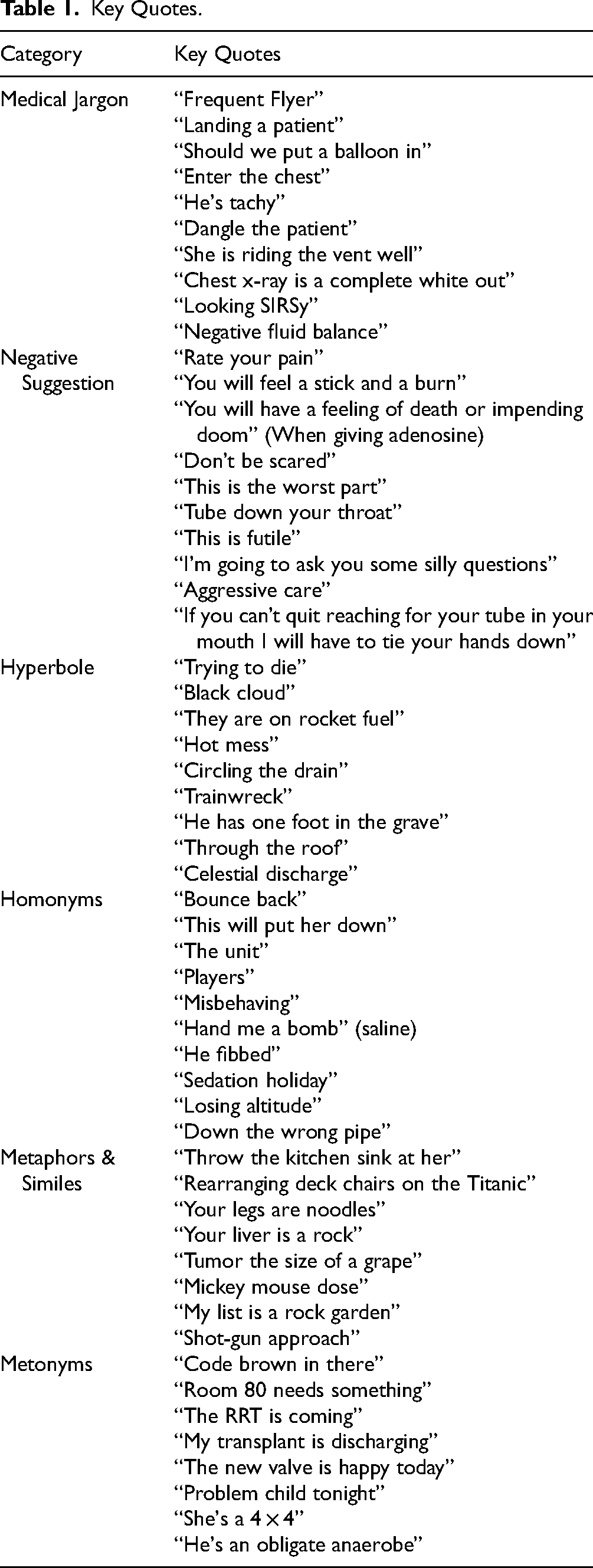
Use of medical jargon to describe patient interventions, behavior and changes in clinical status was most common (549 examples). For example, interventions were commonly defined by such expressions as “titrate meds,” “trach and peg,” “up the pressors,” “weaning sedation,” “renal replacement therapy,” “post arrest, being cooled,” “can you get a bomb” (referring to lavaging endotracheal tube with saline). Patient behavior descriptors included “riding the vent,” “she is tachy,” “patient has a lot of output,” and “will withdraw to pain.” Expressions as “unstable vitals,” “train wreck,” “tanking,” “they RRT’d last night,” and “looking septic” were used to describe change in clinical status.
Negative suggestions were used to describe patient experience, prognosis and change in clinical status (217 examples). For instance, phrases such as, “you may feel a burning sensation,” “your memory will fluctuate,” “impending doom,” and “this won’t be comfortable” were common when warning a patient of potentially uncomfortable experiences, mostly surrounding procedures. Communicating prognosis to patients, family members, and between care team members often included phrases like “not going to make it,” to “high risk” or, “we will withdraw care.”
Hyperboles were mostly used to describe patient or provider characteristics (113 unique examples). Examples included “he is bone dry,” “gallons of blood,” and “black cloud.” Hyperbole was often employed to describe patient prognosis, such as “trying to die,” “patient is tanking,” and, “they are a corpse in there.” Phrases like, “throw the kitchen sink at her,” “he is an anaerobe”, “rearranging deck chairs on the Titanic,” “your liver is a rock,” “this one is running to the light,” “my list is a rock garden” were representative examples of metaphors/similes (121 examples) used to describe patient interventions and status. Homonyms such as “bounce back,” “this will put her down/snow her,” “he fibbed,” “the patient is on rocket fuel, they won't be going anywhere for a while,” accounted for 150 examples. Lastly, 144 metonyms were provided mostly referring to a patient by their chief complaint (“the bleeder is coming up,” “COPD’er needs CPAP”) or as a procedure (“that hip needs to walk”).
There was a wide range of responses to the last question asking to provide the most memorable phrase one can think of that might sound confusing or have a potentially negative impact on a patient in the ICU. Most of the quotes were examples of communication with patients, such as “I once heard a physician give a patient a prognosis by stating, ‘we know people don't live forever’.” “We don’t want to give up, you just need to get stronger to get further treatment (in the setting of patient dying).” “The operation was a success, but your husband was not strong enough for my procedure.” “From a personal ICU experience as a patient—‘it wasn’t as bad as it seemed’—I felt so invalidated by another physician during a time when I was so vulnerable.” “I once heard a surgeon tell a family they would attempt a procedure, but if it wasn't going well, ‘they would abort’; after he left, the family asked me who was going to get an abortion.” “Some patients think when we order a ‘diet’ we are putting them on a diet (and it just means we are feeding them normally).” “Do you want to live or do you want to die?” was once used when discussing goals of care and code status.” “I often hear ‘you FAILED your swallow study … you did not PASS your swallow study’ by physicians, nurses, and occupational therapists—this is incorrect, you cannot fail a swallow study, just like you cannot fail a chest X-ray or CT; it can be incredibly demoralizing for patients to hear this”.
In reviewing response categories by the provider group, majority of responders included examples in most survey categories without a clear pattern of preferring specific category by one's role in the ICU.
Discussion
Our study demonstrates that the use of imprecise language that has the potential to confuse or suggest negative outcomes in critically ill patients is common in the ICU, with medical jargon being most prevalent.
While the nocebo effect of common medical language has been recognized in general medical literature,11,28–30 there is limited awareness of its potential implications in the critical care setting. Critically ill patients experience inattention and resultant impairment in abstract thinking. Subsequently, they may be particularly vulnerable to misperceiving imprecise language. Imprecise language may contribute to patient anxiety, distrust in their medical team, and even clinical deterioration 31 as semantic processing is preserved even in deep sedation or comatose states.4,32,33 We identified 912 phrases used by critical care team members to serve as a foundation for further dialogue on the potentially deleterious therapeutic effects that may arise from imprecise language in the ICU. Our study demonstrated that imprecise language is observed in all aspects of critical care including interventions, patient behavior, clinical status, prognosis, provider-patient communication, and even provider characteristics. A critical care physician who was also a patient in her ICU observed that negative suggestions prompted by questions such as, “Do you feel anxious?” or announcing that a patient will “feel a little pressure or pain” may also diminish the therapeutic benefit of active medical interventions. 14 Others commented that the frequent use of violent metaphors in the ICU setting promoted an oppositional and subjugatory relationship between the patient and the healthcare system while not providing actionable clinical information. 34 In our study the majority of metaphors were not violent but no less stigmatizing. Recognizing that critically ill patients do process speech even when sedated but have very limited in ability for abstract thinking, use of metaphors describing their clinical condition as a “hot mess,” “kidneys are toast,” “circling the drain,” or hyperboles such as “rip-roaring sepsis,” “flooded with fluid, “nothing is going to help her” can only promote their insecurity and fear.
Why is the imprecise language so prevalent in the ICU? Despite only a 17% response rate, the number and diversity of unique examples provided in our survey were surprising. Some have hypothesized that the use of figurative language adds color and may reinforce group cohesion, or that this rather dark humor can serve as armor that clinicians use to protect themselves from constant exposure to human suffering. 35 Other ICU clinicians observed that disconnecting from patients through imprecise language while reinforcing the hierarchy of power can indeed lead to “us versus them” mentality.34,35 But do the “armor” of depersonalization and a sense of isolation truly represent an attribute of professional joy, or are they symptoms of burnout?36,37 And if is the latter, why do we keep doing it to ourselves (and patients)?
The answer is likely that our words reflect our intentions, but the power of intention is often not recognized as a factor in anyone's outcomes, either patient or provider. Yet our intentions and expectations can influence both. Intention could be expressed verbally: provision of simple orientation during emergence from general anesthesia as opposed to just issuing a command to open eyes has significantly lowered emergence agitation. 38 Intention can also be non-verbal. In a double-blind study of dentists who thought they were administering placebo, naloxone, or fentanyl (but could not verbally communicate this to patients), perceived pain scores were dramatically lower in the “fentanyl” group although all patients actually received placebo. 39 Moreover, a recent qualitative study revealed that physicians used imprecise “hedging” language a median of 74 times per enconter in communications with surrogates of critically ill patients when making decisions about care. 40 Patients may also remember more information than medical teams anticipate. A study of 313 mechanically ventilated adults revealed that 47% had factual memories and another 34% had delusional memories with or without factual recall. 21 In describing the power of language in medical interactions, David Cheek, a famous researcher of the power of hypnosis on body's physiology, said, “If a statement can be interpreted optimistically or pessimistically, a frightened person will interpret it pessimistically. If a critically ill patient is frightened, an ambiguous stimulus is more likely to be interpreted as threatening.” 31
Our study has several strengths. It highlights an underemphasized area of critical care practice. The impact of provider language has been recognized in other areas of medicine, yet understanding of the power of its impact in the critical care setting is limited. Additionally, we involved a variety of interprofessional critical care stakeholders who provided a large diversity of examples. The study limitations include a low response rate, limited knowledge about interrater reliability of the communication types, and sampling restricted to a single academic institution. As only provider feedback was obtained, our understanding on the actual impact of this figurative language on the patients is limited. It is possible that provider self-reflection has a positivity bias and the prevalence of these negative phrases is actually higher than what was reported. Although imprecise language appears to be routinely used in the critical care setting, the frequency of its use and any effect on patient outcomes is still unknown.
Conclusion
Imprecise language is common in critical care practice. Whether these communication types lead to an unintended nocebo effect on mental health or other outcomes in survivors of critical illness deserves further study, and incorporating patient perspective is the next step in this line of research. Meanwhile, critical care team members can adopt communication practices that may reduce harm. Suggestions include: (a) always speak as though patients can hear you; (b) reduce communication that is not directed at the patient while in their presence; (c) describe negative states like pain, anxiety, restraints as normal for the circumstances and temporary; (d) limit the use of hyperbole and negative metaphor, which rarely improve clarity of communication with patients in altered states of consciousness.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241272148 - Supplemental material for Communication in the ICU: An Unintended Nocebo Effect?
Supplemental material, sj-docx-1-jpx-10.1177_23743735241272148 for Communication in the ICU: An Unintended Nocebo Effect? by Irene Riestra Guiance, Lindsey Wallace, Katalin Varga, Alexander Niven, Megan Hosey, Jillene Chitulangoma, Kemuel Philbrick, Ognjen Gajic, Madeline Weiman, Emily Schmitt, David Pasko and Lioudmila Karnatovskaia in Journal of Patient Experience
Footnotes
Abbreviation
Acknowledgments
we thank Danielle Shilling, MD for contributing to the survey development and distribution.
Author Contributions
IRG and LW wrote the first draft of the manuscript; KV, AN, MH edited the initial manuscript; LK, LW, KV, JC, KP, OG, MW, ES, and DP participated in drafting of the initial survey and manuscript editing; LK finalized and distributed the survey and edited the manuscript; LK, AN, and MH collaborated on responding to reviewers.
Consent Statement
Not applicable.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mayo Clinic Critical Care Research Committee provided funding for the publication of this article. Dr. Karnatovskaia is supported by a grant from the National Heart, Lung, and Blood Institute K23HL146741-1.
IRB Approval
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.