
Abstract
Many family members whose loved ones stay in the intensive care unit (ICU) have post-traumatic stress disorder (PTSD) after the hospitalization. A mixed-methods longitudinal randomized trial studying family members of medical ICU (MICU) patients was conducted. Participants were randomized into 2 groups (intervention and control). Post-traumatic stress symptoms checklist-14 scores for the intervention group trended downward over time, but no differences were detected in PTSD risk between the intervention and control groups. The ICU experience for family members is traumatizing. A simple gesture of providing ICU diaries for them to use during the ICU stay may help reduce their emotional burden and requires further investigation.
Keywords
Introduction
One-third of family members have post-traumatic stress disorder (PTSD) after the intensive care unit (ICU) stay, and it increases to 60% if they die (1). PTSD risk increases when emotional distress is present, coupled with a lack of understanding of the ICU stay. Often, families of ICU patients express misunderstandings due to a lack of communication between them and the healthcare team. Another factor that impacts understanding is that emotional distress impairs one's ability to understand or digest large quantities of information (2). While the healthcare team is omnipresent in the ICU, the most communication between the healthcare provider and family occurs once a day in the form of “rounds,” which families are not always attended by the family. In non-ICUs, patients themselves can sometimes provide critical information about the occurrences in the hospital to their families. In the ICU, patients are too ill to fully understand the ICU stay, either due to sedating medications or directly due to their illness. Family members need to know how their role in the family shifts while their loved one is critically ill. The family member also needs to have a concrete understanding of the ICU stay as related to the Facilitated Sensemaking middle-range theory, which helps family members of patients make sense of what has transpired and their new roles (3). The ICU diary is a tool that can support both of these needs.
Using a concurrent triangulation approach, (4) the objectives of this mixed-methods pilot study were to (1) evaluate if family utilization of a diary during a loved one's ICU stay would decrease the risk of PTSD for family members, (2) understand if the severity of their loved one's illness had an impact on the risk of PTSD of family members, and (3) understand if the diary was considered a valuable tool for family members of ICU patients.
Methods
The setting was a large academic medical center located in the northeastern United States. The teaching hospital is an 886-bed, four-time Magnet-designated® hospital with 8 adult ICUs and 2 adult step-down units. The unit where subjects were enrolled is a 12-bed medical ICU (MICU) within the hospital. A clinical nurse conducted a longitudinal randomized trial as part of a hospital-based nursing research internship, which provides protected time for scholarship (5). This study was submitted to the university's institutional review board and was granted expedited approval. Family members of MICU patients were consented to enroll in the study. Inclusion criteria included age greater than 18 and English literacy. Excluded from the study were paid caregivers, those under 18 years of age, and those with cognitive impairments that would impede their ability to consent to the study.
Once enrolled in the study, the family members filled out a demographic survey at consent. At the time of consent, a coin was flipped to ascertain if the family member would receive a diary (intervention group—heads) or not (control group—tails). The diary provided was a simple notebook titled “My ICU Diary.” On the first page, instructions for use were provided to the participants.
About 6 weeks (Time 1, T1) after the ICU stay, the participants in the intervention arm responded if they found the diary helpful and rated its usefulness on a Likert scale. At T1, the participants from each arm completed a PTSD risk scale titled post-traumatic stress symptoms checklist-14 (PTSS-14), (6) and a survey about the frequency of diary use and severity of their loved one's illness during the ICU stay. The PTSD risk scale was repeated at 3 months (Time 2, T2) and 6 months (Time 3, T3) post-discharge.
Results
This study used a pragmatic mixed-methods paradigm since it is flexible, adaptable, problem-centered, and real-world practice-oriented (7–9). Quantitative analyses were performed using SPSS Version 29, (10) and statistical significance was set to P < .05. Dedoose (11) was used to examine the qualitative data.
Quantitative
From September 2017 to December 2019, 41 participants from the MICU enrolled in the study. There was a nearly even distribution between the control (56%) and intervention (44%) groups. An even distribution of age groups was split across the 2 groups: most were spouses, 39% versus 56%; White, 78% versus 56%; females, 87% versus 72%, control versus intervention, respectively. Most family members were nonparents and split between significant others and nonsignificant others, eg, siblings. Forty-four percent of family members completed the Time 1 data collection, 32% completed both the Time 1 and the Time 2 data collection, and 17% completed all longitudinal data collection. Of note, subjects who completed the study were nearly all female (86%) and White. All minority groups dropped out of the study, consistent with previous literature citing high attrition rates among minority research subjects (12,13).
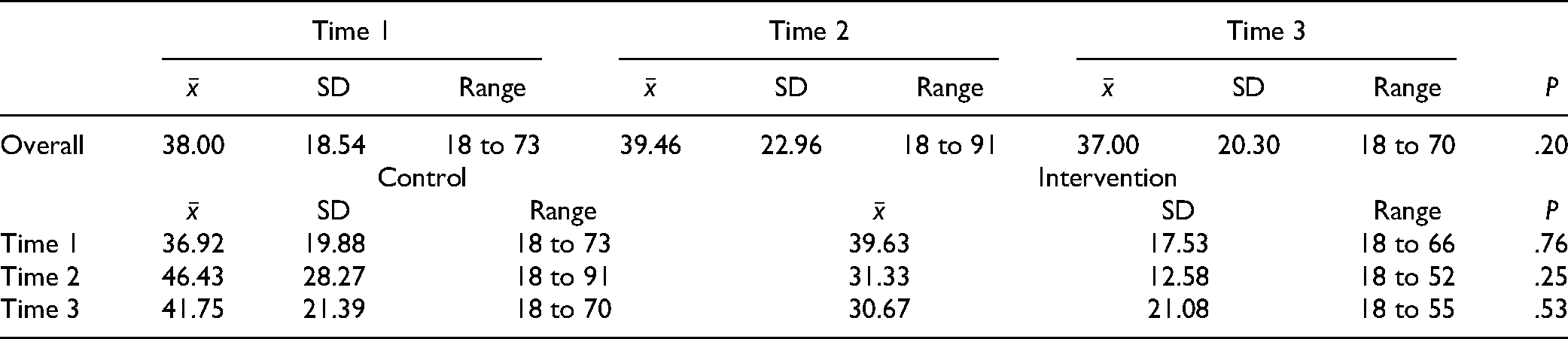
As seen in Table 1, the mean PTSS-14 scores remained consistent for those families who completed the study. The PTSS-14 scores for the control group increased over time, while the scores for the intervention group decreased over time. The trendlines for both groups over time appear in Figure 1. None of these differences were statistically significant. One hundred percent of family members reported that the diary was a useful tool at Time 1, while two-thirds of families said the diary being helpful at Time 2. Using a scale of “Not helpful” (1) to “Helpful” (3), respondents found the use of the diary helpful (

Mean PTSS-14 scores over time.
PTSS-14 Scores.
Qualitative
Twenty-three participants provided open-ended feedback. Ten participants wrote how they used the diary to make sense of their family's time in the ICU. Specific quotes revealed that subjects valued the diary, for example: “Gave me something to do, also when you’re there. I just kept replaying what happened, but once I wrote it down, I was able to kinda move on. Think about the future and what got us there (sic)” and “It helped get feelings out on paper and keep track of his daily progress.” The most common co-occurrence of themes was “Caregiver experience” and the “ICU stay/experience” (n = 11). When quantified, these 2 codes were the most frequently used in the data set (n = 36 and n = 21, respectively).
Discussion
The PTSS-14 scores remained consistent for family members, with scores in the control group increasing over time and scores in the intervention group decreasing over time. The thematic analysis confirms this with the majority (79%) of comments related to mental health being provided by the intervention group. Participant comments like “It helped get feelings out on paper…” indicate that the diary helped with the stress levels. Additionally, the intervention group was more likely to discuss their experiences when compared to the control group (81% vs 19%). However, family members in the control group were the only ones to describe experiences with the death of a family member. These themes relate to the reported length of ICU stay in days, as the control group had a longer length of stay than the intervention group (Control:
Limitations
The study was powered for 100 subjects, with 50 in each arm, to detect statistical differences between the 2 groups. Unfortunately, due to hospital visitor restrictions because of the COVID-19 pandemic, the feasibility of recruiting family members in the critical care units became impossible, and the study was stopped before the acquisition of 100 subjects. Also, the attrition rate by T3 was 83%, and among minority family members, 100%. Thus, attrition poses a methodological threat to all research concerning the validity of conclusions drawn from longitudinal studies. Also, it is essential to note that 13% of subjects in the control group independently used a journal due to being exposed to the study. The mental health history of family members was not collected when demographic data were collected, which prevents the data from being analyzed further to determine if prior mental conditions mediated the results. These data would be beneficial to include in future research.
The limitations of this pilot study demonstrate the need for further research on this topic. Future studies should acquire at least 100 subjects, with 50 in each arm, to detect statistical differences between the study groups. In addition, researchers should collect data on stress levels at the outset of the study to understand better how this changed over time concerning the intervention.
Conclusions
The analyses did not detect differences in PTSD risk between the diary and control groups in the study. However, it is important to note that most participants felt the diary helpful. Multiple participants remarked that the diary helped them make sense of the ICU stay and gave them something to do during a difficult time which resonates with the Facilitated Sensemaking Theory. It is also important to note that while the results did not reach statistical significance, the PTSS-14 scores for the intervention group trended downward, supporting the idea of providing diaries to families. This finding is consistent with other small studies that have shown a reduction in post-traumatic stress symptoms in family members of ICU who have either written in diaries or were provided diaries written by the healthcare team (14–16). The ICU experience for family members is traumatizing, and a simple gesture of providing ICU diaries for them to use during the ICU stay may help reduce their emotional burden.
Footnotes
Acknowledgements
The authors would like to acknowledge the Strong Memorial Hospital Research Internship for Nurses which provided time for this creation of this project as well as E. Kate Valcin, DNP, RN, NEA-BC, CCRN-K, CNL, Director of Adult Critical Care Nursing, Strong Memorial Hospital, for her continued support of the project.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval.
Ethical approval to report this case was obtained from the University of Rochester Office of Human Subjects Protection STUDY00001243.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institution at Which the Work was Performed
Strong Memorial Hospital, University of Rochester Medical Center, Rochester, NY.
Statement of Informed Consent.
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the University of Rochester Office of Human Subjects Protection STUDY00001243.