
Abstract
Nurse–patient communication is the foremost step in providing professional care. Nurses can use effective communication as a simple and powerful tool to create comfort, happiness, and vitality to reduce the patient's grief and suffering. This study aimed to explain the nurses’ perception of empathetic nurse–patient communication. This qualitative study was conducted with a content analysis method in 2020. Seventeen hospital nurses were recruited with maximum variation from the educational hospitals affiliated to Qom University of Medical Sciences, Qom, Iran, and semi-structured interviews were conducted until data saturation was reached. Data analysis was performed using Graneheim and Lundman approach. Nurses establish empathetic communication with patients through three main categories of: (1) having humanistic and unique behaviors with the patients; (2) providing a calm and happy environment for the patients; and (3) reducing the patients’ fear and consolation to them. These findings indicate empathetic communication that is appropriate to the conditions and needs of hospitalized patients. The three main categories were accomplished through 14 subcategories. The finding of this study can help to develop a training framework of empathetic nurse–patient communication and design instruments for measuring it.
Introduction
Nursing communication is a vital element in all nursing areas such as prevention, treatment, rehabilitation, education, and health promotion (1). The quality of communication between nurse and patient is recognized as an influential factor in improving patients’ care (2). Luker et al. showed that effective patient care is achieved through effective communication (3). Also, effective communication can improve patients’ independence and satisfaction (4,5) and protect the patient from adverse health consequences caused by ineffective communication such as medication error (6). One of the techniques of effective communication with the patient is empathetic communication (7). Empathy is one of the communication tools that we use to understand others and share our feelings, thoughts, and experience (8). According to some studies, empathy plays a crucial role in effective nurse–patient communication (7,9,10). Therefore, considerable attention has been paid to empathy in nursing, and this concept has firmly embedded in the nursing discourse (11).
In the social sciences, two empathy theories that explain this critical communication process include the theory of the mind and the theory of simulation (12). The theory of the mind shows the human ability to attribute mental states, such as desires, intentions, and beliefs, to others to other people using a controlled, thoughtful process (13,14). The theory of simulation reflects the attributions about others’ thoughts and emotions, which are more automatic or reflexive (15). The theory of simulation refers to our cognitive capacities to simulate and pretend to be in the situation of others (13). In the nursing profession, also, various theories have been proposed. Peplau emphasizes empathetic relationships with patients at all stages of nurse–patient communication (16). In the theory of human-to-human relationships, Travelbee states that the empathic nurse can understand another person's distress, identify its source, and predict the behavior that will result from it (17). Paterson and Zderad's emphasized that the experience of the nurse–patient relationship is interactive and empathetic (18). In these theories, theorists have theoretically explained the nature, importance, necessity, and elements of relationship between two people or between the nurses and patients based on their and perspective and professional knowledge. However, empathetic communication formed on the values, feels, needs, and special and unique socio-cultural conditions of human beings and cannot be explained solely by these theories (19). Therefore, if we want to understand the empathetic relationship between the patient and the nurse, we must pay attention to the experiences and perceptions of the main stakeholders in the clinical context, namely the patient and nurse.
Some studies have discussed empathetic nurse–patient communication. Pehrson et al., based on the experiences of cancer ward nurses, introduced a model of empathetic communication with the patients. This model's strategies included recognizing or eliciting a patient's empathic opportunity, working toward a shared understanding of the patient's emotion/experience, empathically responding to the emotion/experience, and facilitating coping and connecting to social support (7). Wu, based on the experience of psychotherapists, describes ten practices of nurses in establishing empathetic communication with patients as follows: partaking in the clients’ feelings or thoughts, offering comfort, sharing the same experiences as clients, formulating the gist of clients’ problematic experiences, formulating the upshot of clients’ problematic experiences, offering an empathic diagnosis, offering a candidate a method for solving the reported problem, elaborating on clients’ emotional experiences, making a positive assessment of the client's action toward solving their problems and displaying downgraded epistemic access to clients’ problematic experiences (20). Tyner, based on the experiences of dying patients and their families, commented that the nonverbal behaviors of empathetic communication with the cancer patients included using facial expressions to convey a message that we understand the patient's concerns, intentional sitting and facing the patient to create a feeling of interest, bodily movements to show understanding and hand gestures to establish proper humility and sensitivity (21). Raudonis, based on the experiences of hospice nurses, argues that an empathic relationship means acknowledging patients as valuable individuals regardless of their physical diagnoses and have a friendly relationship with them (22).
These studies have described the empathetic nurse–patient communication in different settings, statuses, and stakeholders as various forms and meanings. According to our search, no study in Iran has examined the meaning of empathetic nurse–patient communication. As shown, the way of empathetic communication is different in different cultures. Therefore, Iranian nurses cannot fully use the patterns of other cultures to communicate empathetically. Also, non-Iranian nurses will be challenged if they want to have empathetic communication with Iranian patients according to their cultural patterns. Therefore, this study was conducted to clarify empathetic communication with the patient based on the experiences of Iranian nurses.
Method
Design
Qualitative content analysis is a systematic method to analyse qualitative data (23). Content analysis is used for condensing and abstracting a large amount of textual data (23) and direct extraction of participants’ messages without imposing a researcher's opinion (24) to gain new insights into the study phenomenon. Therefore, according to the question of the study, “what's the meaning of empathetic nurse–patient communication?” we chose the qualitative content analysis approach.
Setting and Participants
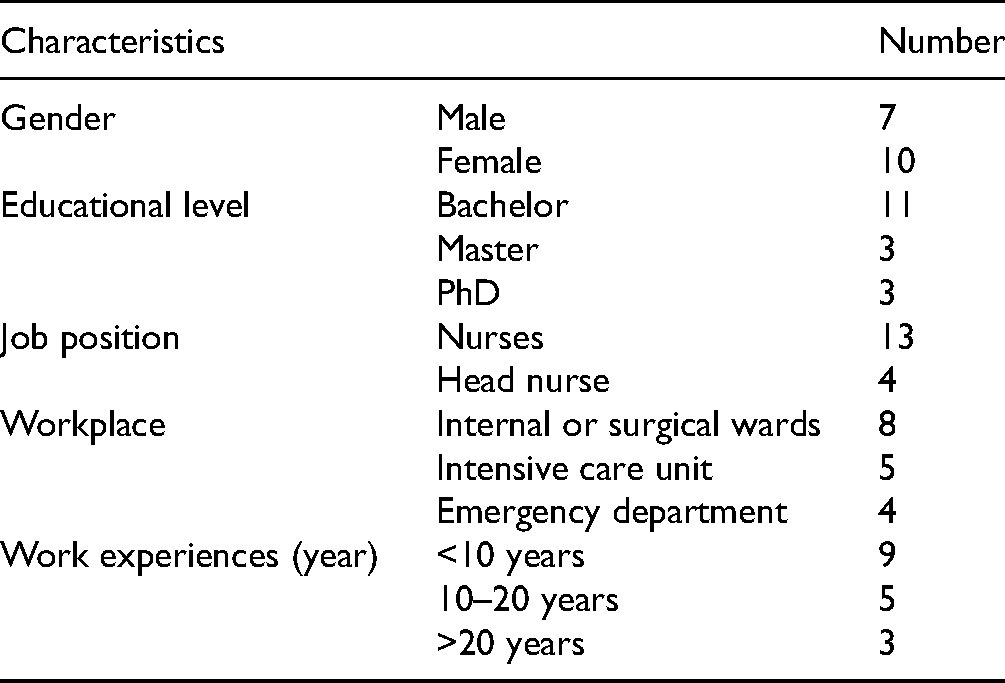
The setting was hospitals affiliated to Qom University of Medical Sciences, Iran. Seventeen nurses were purposefully selected and entered the study. Inclusion criteria included having at least 2 years of nursing experience, having at least a bachelor's degree, having direct communication with the patients, and having informed consent to participate in the study. As shown in Table 1, we select the participants that have the most diversity in terms of gender (male or female), education levels (from bachelor to PhD degree), job positions (nurses, head nurse), workplaces (internal ward, surgical ward, intensive care unit, and emergency department), and work experiences (from three to 23 years).
Characteristics of Study Participants.
Data Collection
In the qualitative analysis methods, the extracted data are based on the perception and daily experience of the participants (25). From March to September 2020, we used face-to-face interviews to extract nurses’ experiences from empathetic communication with the patient. The first author conducted the Persian language interviews in a convenient and quiet place in the hospitals. In the two interviews, some ambiguities did not allow for deep extraction of the data. Therefore, the participants were reinterviewed. Each interview lasted for 40–90 min. At the beginning of the interview, the nurses’ trust was gained using the adequate description of their confidentiality and preserving the interviews and audio files. Text notes were immediately reviewed and completed to ensure an accurate record of the participants’ experiences. Interview questions were: “In day-to-day care of patients, please describe your experiences about communication with the patient,” “Please describe your successful experiences of communicating with the patient,” and “How do you try to make your relationship with your patients happy?” Then, probing questions were also used to clarification or elicit further details during the interviews: “Can you explain more?”, “What does it mean?” or “Give an example, please.” Also, the field notes over the interaction of nurse(s) were recorded. The interviews continued until the saturation of the data. It means that no additional data are being found whereby the researcher can develop a new category (26). The categories seemed saturated regarding their properties and dimensions after the 15th interview. However, two additional interviews were conducted to ensure no new data emerged and no new conceptual code emerged. The research team and the external reviewer made the decision about achieved data saturation by continuous review along with data collection.
Data Analysis
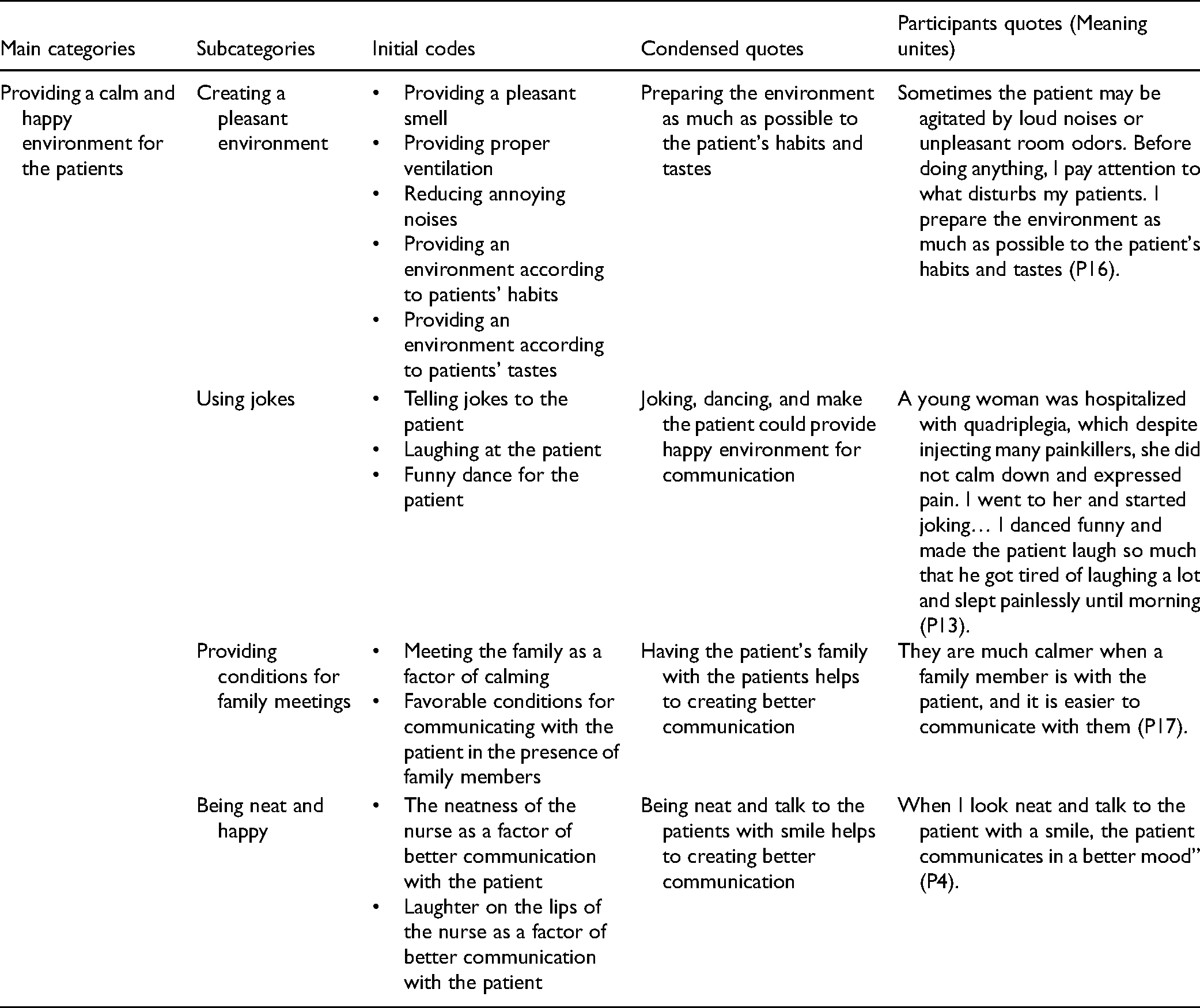
All interviews were recorded with the permission of the participants. After each interview, the content was transcribed with Microsoft Office Word software and analyzed by Graneheim and Lundman (27). In the first step, each interview was transcribed word by word. In the second step, each interview's text was read several times word by word, sentence-to-sentence, and paragraph-to-paragraph to obtain a sense of the whole. In the third step, the meaning units of each interview transcript were identified and coded. The first author analyzed the total data, while the second and third authors analyzed half of the textual data. Three authors then compared the codes and revised minor disagreements after discussion. In the fourth step, codes are grouped into subcategories according to their conceptual similarities and differences. In the fifth step, subcategories compared with each other and the latent data content identified and presented as the main categories. The final three categories were examined by all authors to ensure a clear difference between the main categories and subcategories and fit the data within each category. Also, all the codes, subcategories, and main categories were given to one of the faculty members outside the research team. He separately reviewed and confirmed the appropriateness of data analysis. Parts of the audiotape were translated from Persian into English by an independent translator blind to the study to check for consistent translation. An example of the process of category formation is shown in Table 2.
An Example of the Process of Categories Formation.
Trustworthiness
Lincoln and Guba criteria, including credibility, transferability, dependability, and confirmability, were used (28). The credibility was established by allocating enough time for each interview and member check-in the interview and data analysis stages. Also, two research supervisors checked the quality of interviews, coding, and categories to reach a consensus. Dependability was accomplished by long-term engagement with participants and the constant comparative method. In this way, the initial codes were examined and compared several times, and the repeated codes were analyzed and categorized. For dependability, all stages of the study were reported in detail. For confirmability, codes and categories were reviewed and approved by a faculty member outside the research team. Finally, transferability was established through maximum variation sampling.
Findings
Data analysis led to three main categories and 14 subcategories (Table 3). According to the findings of this study, nurses establish empathetic communication with patients through three main categories of: (1) having humanistic and unique behaviors with the patients; (2) providing a calm and happy environment for the patients; and (3) reducing the patients’ fear and consolation to them.
The Products of Data Analysis in This Study.

Having Humanistic and Unique Behaviors with the Patients
Nurses’ quotes showed that they have humanistic and individual behaviors with the patient. Friendly behavior, the unique way of dealing with each patient, maintaining patients’ dignity, considering the patient's beliefs and culture, and paying attention to changing patient behavior indicate nurses’ humanistic and unique relationship with patients.
A male nurse said, “When patients feel that all their needs have been met and respected, they trust us more … This creates a stronger relationship between the patient and us” (P4).
A female nurse said, “It is not possible to communicate with all patients in the same way … Patients have different cultures and beliefs … In my first encounter with the patient, I tried to understand his cultures and beliefs so that I can have a good relationship with him/her” (P17).
Friendly Behavior with Patients
Most participants stated that they put themselves in the patients’ shoes to understand their needs and establish close and friendly communication. They indicated that they spoke to patients with humility, in a pleasant and sincere tone, and answered patients’ questions in a kind and straightforward language.
A female head nurse commented, “I try to use simple words to get closer to the patient, and if the patient asks me a question about the treatment process, I am not indifferent. Modestly, with openness and a good tone, I make the patient's mood a little better” (P2).
A female nurse described, “When the nurse is agitated, the patient becomes agitated too … I tell the novice nurse that if you want to have an empathetic relationship with the patient, you must speak to them friendly with humility, and sincere tone” (P16).
The Unique Way of Dealing with Each Patient
Participants believed that each patient had their personality, and nurses should not have the same stereotypical behavior in empathetic communication with the patients. Instead, they should establish a unique communication based on the personality and interests of the patients.
In this regard, a male nurse said, “I do not treat all patients in the same way. By my understanding of each patient's personality, I communicate with them. I talk to some of them very seriously, and I communicate with some patients with jokes and laughter” (P15).
Maintaining Patients’ Dignity
Some participants stated that using appropriate words, introducing oneself at the beginning of communication, explaining and informing the patient about interventions, respecting patient decisions, and avoiding sarcasm make the patient feel good about nurses and softens communication.
A female nurse commented, “One of my colleagues uses harsh words with the patients, which causes arguing. However, I talk to the patients very respectfully. When I enter the room… I introduce myself. I call them with friendly words, like “dear mom” I teach them with simple and soft expressions, so when I am a shift nurse, the patients are delighted and in a good mood” (P9).
A female nurse said, “Nurses who talk to a polite patient are less likely to argue with the patient, and the patient is more likely to follow their treatment recommendations” (P3).
Considering the Patients’ Beliefs and Culture
Most participants believed that effective and uplifting communication with patients required communication according to patients’ culture, language, preferences, or religious beliefs. Because if you ignore the patient's beliefs and culture, who have lived with that for many years, they suddenly become very anxious, and the communication continues to be disrupted.
A male nurse stated, “I give patients clothes, prayer books, or poems, consistent with religious and cultural beliefs. I care for the dying patient as much as possible according to the patient's beliefs. I allow the family to be present at the bedside and prepare them for the patient's death according to the family's preferences and beliefs. In this way, they will communicate more with me, and they will have more peace and joy” (P1).
A female head nurse commented, “ After heart surgery, a patient insisted on having a radio … he said that if I did not have a radio, I would be stressed … I gave him a radio … he calmed down after I gave him the radio and I was able to communicate well To have with him” (P10).
Paying Attention to Changing Patients’ Behavior
Participants in this study believed that when we pay attention to the patient's appearance and behaviors and give him feedback about changes in these issues, the patient realizes that he is important for the nurse and feels closer with the nurse.
A male head nurse said, “Some nurses work like a robot without paying attention to the patient's nonverbal reactions, But I try to act differently. For example, when I do IV Cath and see the patient is scared, I try to talk to distract her” (P8).
Providing a Calm and Happy Environment for the Patients
Clinical nurses establish empathetic nurse–patient communication by creating a pleasant atmosphere, using jokes, providing conditions for family meetings, and being neat and happy.
A female head nurse expressed, “In a pleasant and happy environment, patients feel more relaxed and more inclined to communicate” (P10).
A female nurse described, “Agitated people are not focused and do not have the patience to communicate with others … Sometimes, providing a pleasant atmosphere allows the patient to calm down and communicate with them” (P3).
Creating a Pleasant Environment
Participants stated that the strange and noisy environment of the ward causes patient anxiety and impedes proper communication with nurses. They emphasized that providing a pleasant smell, adequate ventilation, reducing annoying noises, and providing an environment according to patients’ habits, tastes, and beliefs can help to establish empathetic communication.
A female nurse described, “Sometimes the patient may be agitated by loud noises or unpleasant room odors. Before doing anything, I pay attention to what disturbs my patients. I prepare the environment as much as possible to the patient's habits and tastes so that I can calm the patient down and be able to communicate with him easily” (P16).
A female nurse commented, “I went to the patient who had just been admitted to talking to him about his illness, the patient was constantly moving around the bed, and he was not paying attention to me …I found that the patient is bothered by the hospital pillow …After his wife brought his pillow, the patient calmed down, and I was able to have a good relationship with him.” (P7).
Using Jokes
Participants stated that joking with patients, using funny sentences, encouraging patients to define happy memories, and, if possible, celebrating on different occasions had a significant effect on establishing close communication with patients.
A male nurse commented, “A young woman was hospitalized with quadriplegia, which despite injecting many painkillers, she did not calm down and expressed pain. I went to her and started joking… I danced funny and made the patient laugh so much that he got tired of laughing a lot and slept painlessly until morning” (P13).
A male nurse described, “By turning the patient away from grief using funny sentences, you can have an effective relationship with the patient” (P1).
Providing Conditions for Family Meetings
Most of the participants stated that loneliness and being in an unfamiliar environment cause nostalgia and discomfort to patients, and in such cases, patients are reluctant to communicate. The nurses had experienced that a family member's presence calms the patient and creates more favorable conditions for the patient to communicate.
A female nurse said, “They are much calmer when a family member is with the patient, and it is easier to communicate with them” (P17).
Being Neat and Happy
Most of the participants stated that most patients were reluctant to communicate with sloppy and untidy nurses. They emphasized that a nurse at the patient's bedside with clean clothes, beautiful appearance, smiling face, and pleasant smell can lead to empathetic communication.
A male nurse said, “When I look neat and talk to the patient with a smile, the patient communicates in a better mood” (P4).
Reducing the Patients’ Fear and Consolation to Them
Participants showed that stress, anxiety, pain, and suffering are the barriers to empathetic nurse–patient communication. Participants argued that by giving hope, using distraction, spirituality, and normalizing new circumstances, they provided the conditions for empathetic communication.
A male nurse commented, “Existence of numerous medical types of equipment and unfamiliar environment leads to patients’ fear and anxiety …. Patients’ fear makes them distrust us and have no desire to communicate” (P6).
A male nurse described, “Patients with pain or stress avoid communication … By turning on the TV or encouraging them to listen to music, I distract them from their pain and anxiety so that I can give them the training they need” (P5).
Giving Hope to Patients
Sometimes the condition of the disease causes the patient to feel frustrated. The frustrated patient is reluctant to communicate. Participants stated that they give patients hope for a better future by talking about the transience of periods of suffering and showing successful people with similar conditions.
A female head nurse said, “I told a patient who had deformed appearance due to burns not to be disappointed that cosmetic surgery could alleviate your problem, and despite these changes, you can have good days in the future” (P10).
A female nurse commented, “ I went to teach a diabetic patient about her self-care… she did not listen to me at all … she said that if you cut off my toe, I could not return to normal life … … I asked a patient who had previously had her toe amputated due to diabetes to explain her lifestyle after the operation. When the patient realized that she could return to a normal life after the operation, she listened to me” (P11).
Using Distraction to Reduce Patients’ Stress and Suffering
Fear, anxiety, and suffering from illness interfere with the positive communication of patients. In this regard, participants stated that using thought destruction methods such as watching TV, reading books, asking deviant questions, or involving patients in self-care can promote empathetic nurse–patient communication.
A male nurse expressed, “There was a child in the ward. At first, he did not look at us or talk at all … he was scared. I took a latex glove and made a doll, and talked in a funny cartoon character. I brought him a piece of paper. He painted for me. We played like this, and we all laughed, and then he trusted me and answered the questions” (P6).
Using Spirituality to Reduce Patients’ Pain and Stress
Participants in the study believed that in addition to distraction techniques, focusing on spirituality could reduce patients’ suffering and create an empathetic nurse–patient relationship.
A female nurse said, “One of the patients who had just been diagnosed with cancer was very upset and crying. I explained to him that God loves the patients very much because of the pain and suffering they endure. I told him to pray and ask God for help and hope. After that, the patient's mood improved” (P14).
Normalization of new Conditions
The presence of patients in new conditions, especially the presence of various medical equipment connected to the patient, can increase the patient's stress, and this stress is a barrier to effective communication with patients. Most participants in the study stated that normalization of new conditions using methods such as explaining patient-connected equipment, providing an opportunity for sick children to touch medical equipment, and showing a film of postoperative conditions could reduce the patient's stress as a barrier to empathetic communication.
A female head nurse commented, “In the ICU, a child was scared and anxious because of seeing the types of equipment and did not allow us to take care of him… I helped him to touch the equipment that was connected to him… this reduced his stress, and I was able to take care of him” (P12).
A male nurse commented, “my patient regained consciousness and opened her eyes … she was very agitated … I explained to her where she is, what happened to her and why she is here … with my explanations, the patient calmed down, and she did not fight with the ventilator.” (P13).
Discussion
This study showed that nurses try to establish empathetic nurse–patient communication by having humanistic and unique behaviors with the patient, providing a calm and happy environment for the patient, and reducing the patient's fear and consolation to them.
Finfgeld-Connett, argues that having intimate relationships with the patients requires listening, providing information, encouraging close associates to express their concerns, ensuring that they look after themselves, helping them cope with difficult situations, and sharing personal thoughts and feelings openly and honestly (29). Raudonis also showed that an empathic relationship means acknowledging patients as valuable individuals regardless of their physical diagnoses and have a friendly relationship with them (22). Unlike the current study, Finfgeld-Connett and Raudonis do not mention providing a happy environment for more effective communication. According to the findings of this study, providing a calm and happy environment for the patient can be effective in establishing effective empathetic nurse–patient communication. Some studies highlighted that physical environmental factors such as adequate lighting, a quiet environment, and providing pen and paper can support the patients in communication to be more involved in conversations (30–32). However, the difference between the findings of our study and these studies is that in these studies, the environment is considered more as a physical environment. None of these studies mentioned the use of techniques to create a happy environment with the patient. According to the findings of our study, nurses can provide a happy environment for the patients using jokes, providing conditions for family meetings, and being neat and happy. Our study participants believed that these techniques could establish effective nurse–patient communication by creating a sense of coherence between them and reducing patients’ depression and anxiety.
Lukmanulhakim showed that effective communication with the patient requires the nurse's eye contact, quick response to the patient's needs, clarity of speech, comprehensible language, active listening, and friendly treatment of the patient (33). The findings of the Lukmanulhakim study focus more on the principles of proper message delivery, and reducing the patient's fear and consolation to them has been neglected. Papadantonaki commented that effective communication requires understanding patient experiences and understanding what concerns the patient (34). However, she did not explain how to alleviate the patient's concerns.
Some studies have described ways to reduce patients’ fear and anxiety. Appukuttan found that dental anxiety can be managed by psychotherapeutic interventions such as muscle relaxation, relaxation breathing, imagery, hypnosis, acupuncture, distraction, and positive reinforcement (35). Croke suggested aromatherapy, acupuncture, music, therapy dogs, visitation, education, and virtual reality as ways to help reduce preoperative patient anxiety (36). According to the findings of our study, using some strategies such as giving hope, building trust, using distraction, using spirituality, and normalizing new circumstances, nurses can reduce patients’ fears and thus establish empathetic communication with them. In our study, unlike the above two studies, the use of spiritual care has been introduced as one of the basic strategies to reduce patients’ fears. This can be related to the high importance of spirituality among the Iranian people. Scott et al. believe that trust and hope are the outcomes of an effective relationship with the patients (37). However, according to the findings of our study, giving hope to patients and establishing trust with them are the main elements of empathetic communication with the patient. In line with the findings of our study, Rutherford emphasized that trust, as one of the nursing's intangible assets, is an essential component of the establishment of meaningful relationships with patients (38).
Wu introduced four types of empathy as namely cognitive empathy, affective empathy, sharing empathy, and nurturant empathy (39). Connett states that an intimate nurse–patient relationship requires listening, providing information, encouraging close associates to express their concerns, ensuring that they look after themselves, helping them cope with difficult situations, and sharing personal thoughts and feelings openly and honestly (29). Also, Hashim emphasized that effective nurse–patient communication requires understanding the patient's perspective entails exploring the patient's feelings, ideas, concerns, and experience regarding the impact of the illness (40). These studies have focused on interacting to identify patients’ feelings, concerns, and needs. However, they did not explain how to identify the patients’ feelings, concerns, and needs. Our study showed that in interacting with patients, nurses should respect patients’ beliefs and culture, maintain their dignity, and have friendly relations with them so that patients trust them and express their real feelings, needs and concerns. There is a limitation in this study. The nurses were interviewed while they were under a lot of stress due to the Covid-19 crisis. This can affect the quality of the interviews.
Conclusion
The findings of our study are similar to other studies in terms of having unique relationships with patients and reducing their fears and concerns in empathetic nurse–patient communication. However, it is unique in features such as friendly behavior with patients, maintaining patients’ dignity, providing a happy environment, and using spirituality to reduce patients’ pain and stress. The framework developed in this study for empathetic nurse–patient communication can be used to design a context-based tool instead of existing theory-based tools to measure the empathetic relationship. The characteristics mentioned in this article for the empathetic nurse–patient communication can be used as an educational framework for nursing students and nurses to improve their relationship with the patient.
Footnotes
Acknowledgments
The authors would like to thank the Research Administration of Tarbiat Modares Universityand all patients who participated in the study.
Authors’ Contribution
A.B, E.M, A.S contributed to study design and conceptualization. A.B, E.M, A.S contributed to data collection. A.B, E.M, A.S contributed to data analysis and interpretation. A.B, E.M, A.S contributed to manuscript writing. E.M, A.S contributed to study supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research Council of the Tarbiat Modares University financially supported the study.
Ethical Approval
Ethical approval to report this case was obtained from Research Committee of Tarbiat Modares University (Ethical code: IR.MODARES.REC.1397.234).
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Research Committee of Tarbiat Modares University (Ethical code: IR.MODARES.REC.1397.234) approved protocols.
Statement of Informed Consent
Verbal informed consent was obtained from the patient(s) for their anonymized information to be published in this article.