
Abstract
Recognizing the paucity of literature describing the non-medical effects of care at a tertiary parental fetal care center upon families, the purpose of the study was to better examine the potential barriers that our patients face related to care in a parental fetal care center. An anonymous survey was sent via email to patients who received care from 2015 to 2021. The survey included questions regarding demographics, fetal diagnoses, non-medical expenses related to care, and the impact of care on patient relationships, employment, and other children. 453 patients (15.9%) responded out of the 2684 emails sent. 58.3% of patients traveled >100 miles to reach our referral center, with 20% traveling >300 miles. 42.6% of patients reported non-medical expenditures exceeding $1000, with nearly 1 in 10 reporting expenditures of >$5000 (8.6%). Overall, 38.2% of women reported moderate to severe financial burdens related to receiving care at the parental fetal care center. This study illuminates the financial and social burdens that care at a tertiary parental fetal care center imposes upon families. By acknowledging these barriers, we can strive to minimize them to best provide equitable access to high-quality fetal care services.
Keywords
Introduction
Recent advancements in fetal imaging, genetic diagnosis, and even fetal intervention have altered the face of perinatal medicine, and the parental fetal care center (PFCC) arose in response to these innovations. PFCCs represent a collaborative approach between practitioners of obstetrics and pediatrics. The goal is to provide comprehensive care and counseling to families expecting a baby with a structural anomaly, a twin-related complication, and/or a genetic abnormality. This goal is medically noble, but there has been little exploration of the non-medical impact of this care upon the patient and/or the family unit.
Many patients must travel from another city, state, or even country to receive care at a PFCC. For example, Bergh and colleagues demonstrated that patients were required to travel a mean distance of 271.1 miles (interquartile range of 184-473 miles) to seek care for evaluation and treatment of twin-to-twin transfusion syndrome. 1 Such travel may be onerous for a family, and, when direct non-medical costs are considered along with lost wages from missed work, this care may also be financially prohibitive, particularly for the subset of patients who are advised to relocate following in utero surgical intervention or in preparation for delivery. Notably, these costs and travel all occur prior to delivery, a fact that may be compounded by the weeks or months that the baby may remain hospitalized at our children's hospital.
Non-medical costs have been at least partly explored for care in the neonatal intensive care unit (NICU), with studies conservatively estimating that out-of-pocket medical costs and non-medical costs for NICU care amount to 5-10% of parental income. 2 These costs frequently cause financial stress and can act as barriers to care, especially for families of lower socioeconomic status (SES).2–4 A similar exploration of costs and burdens has yet to be performed related to care at a PFCC prior to delivery. The objective of this survey was to better define the non-medical effects of care at a regionalized PFCC as part of an overarching goal to improve equitable access to high-quality fetal care services to all in need.
Methods
We conducted a single-site cross-sectional survey of patients who received care at our PFCC from January 1, 2015 through June 1, 2021. This project was approved by the Institutional Review Board at our institution, and patient e-mail addresses were provided through an electronic medical records query.
The anonymous survey was entirely web-based, using SurveyMonkey to create, disperse, and collect responses. The survey was reviewed with an expert in survey creation prior to sending this to potential participants. The survey was initially sent via electronic mail to all identified patients on May 28, 2021, a reminder was sent on June 30, 2021, and the survey was closed on July 14, 2021. This was an open survey in that a password was not required for participation, but only patients seen at our center received a link for access to the survey. Data were captured and stored anonymously within the SurveyMonkey system, and researchers could only access the results using a single designated username and password.
This was a voluntary survey without incentives to participate. Survey respondents first encountered an introduction section describing the purpose of the project, the potential risks, survey specifics, and the plan for data storage. Potential respondents were informed that, by choosing to start the survey after this introduction, they were consenting to participate in the study but could withdraw this consent at any time. Excluding the consent and introduction pages, the questions were distributed over 10 pages with 2-14 questions on each page. All items included a “not applicable” or “other” non-response option, and, to prevent biases, the answers were randomized on certain questions. Participants could review and change their responses prior to submitting the survey. We did not include a completeness or consistency check at the end of the survey. All data were included in the results, regardless of survey completion or time employed to complete the survey, but the number of patients answering each question was available for analysis. The data were examined to ensure that no individual sets of survey responses were identical, but computer IP addresses were not specifically compared nor were cookies used to identify participant computers.
The full survey is available upon request, but, in short, the survey was divided into eight sections (number of questions in each section provided in parentheses): Demographics (7), Travel (6), Family and physician support (6), Homelife (14), Pregnancy (14), Delivery (3), Newborn outcomes (4), and Impact of care upon home life (14).
This was primarily a descriptive study, but calculations of 95% confidence intervals were performed using Wilson's method. Illogical or inconsistent responses were excluded from data analysis. To better understand the relationship betweenSES and the financial impact of care at our PFCC, patients were classified as being of lower SES (reported annual income of <$30,000 chosen for simplicity purposes, extrapolated from the cutoff of <$26,500 used as the poverty level for a family of four per the United States Health and Human Services department in 2021), middle SES, or upper SES (reported annual income of >$150,000). Comparisons were then made among these groups using chi-square tests of independence. A similar analysis was employed to compare costs and reported burdens among local patients (<50 miles) and patients traveling ≥50 miles for care at our center. We did not employ any methods to adjust for non-representative samples.
The Checklist for Reporting Results of Internet E-Surveys (CHERRIES) was employed to optimize the quality of this survey and the subsequent publications. 5
Results
A total of 2845 surveys were emailed to identified patients. Of these, 161 failed to send secondary to incorrect or non-active email addresses, such that 2684 surveys were successfully sent. We had 453 total responders (16.9%), 395 of whom completed the survey (395/453 for a completion rate of 87.2%) while 58 partially completed the survey (58/453, 12.8%). Demographics are provided in Table 1 and data regarding fetal diagnoses and delivery details are outlined in Table 2.
Self-Reported Demographics of Survey Respondents.

Demographic data from survey respondents are included.
Self-Reported Data Regarding Fetal Diagnoses and Delivery Details.

Self-reported data regarding fetal diagnoses and delivery from survey respondents are included.
Of 405 respondents, 208 (51.4%) did not undergo invasive procedure(s) while 84 underwent fetoscopy with at least attempted laser photocoagulation of a complicated monochorionic twin pregnancy (20.7%), 73 underwent amnioreduction(s) with or without laser photocoagulation (18%), 45 underwent amnioinfusion(s) via either port placement or serial procedures (11.1%), 18 underwent prenatal myelomeningocele repair (4.4%), and 13 underwent a shunting procedure (3.2%).
As depicted in Figure 1, three out of every five patients reported traveling ≥100 miles to reach our PFCC (58.3%, 95% CI 53.7-62.8), with one out of every five reporting travel of ≥300 miles (20%, 95% CI 16.5-23.9). As also seen in Figure 1, although one in four patients only attended one visit (27.4%, 95% CI 23.2-32.1), one-third of patients traveled ≥10 times for care (33.6%, 95% CI 29.1-38.4). Most patients traveled to and from our city via personal car (239 of 251 respondents, 95.2%), with three reporting travel via either taxi or rideshare (1.2%) and three traveling via airplane (1.2%).
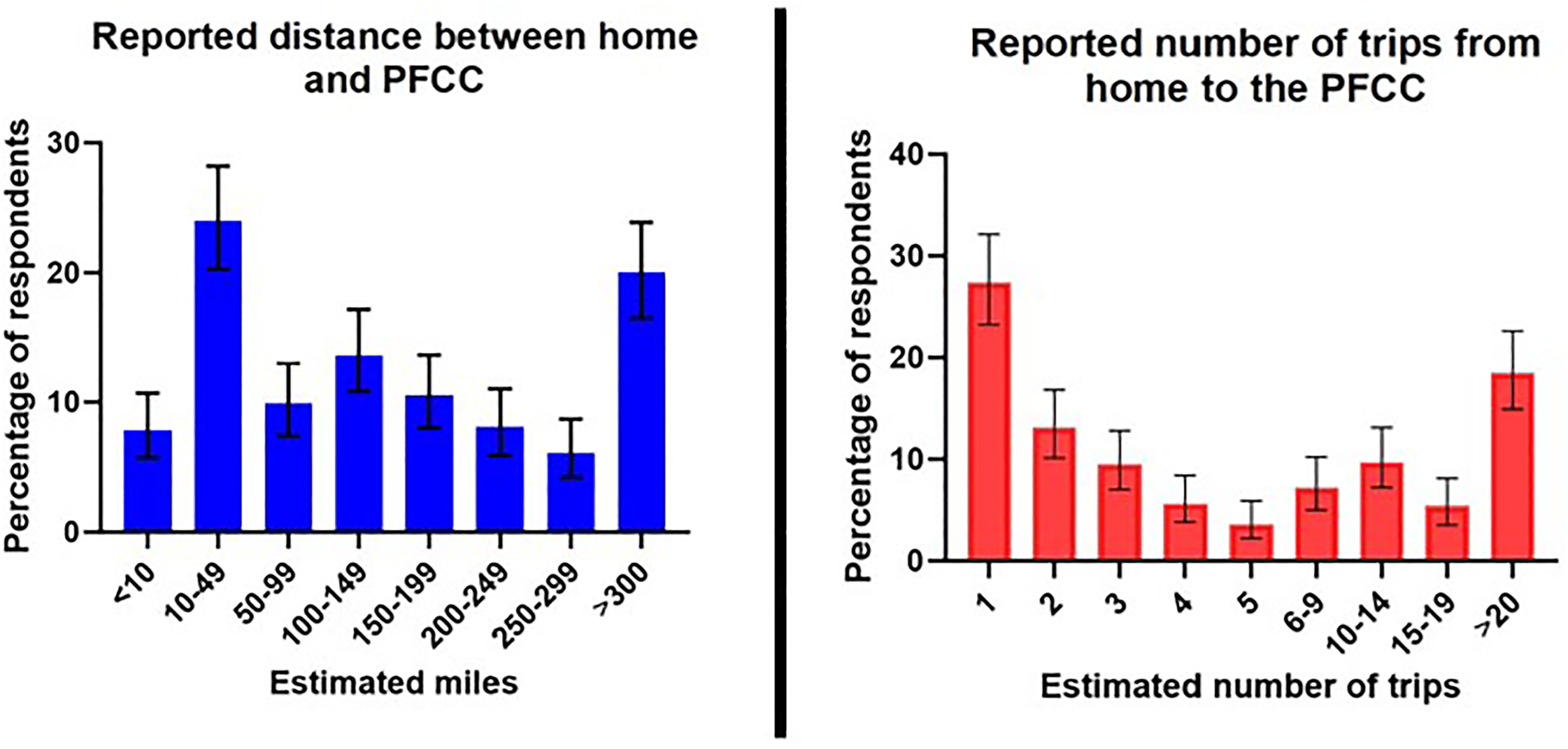
Distance and number of times traveled to the PFCC. Data regarding travel, including the distance between home and the PFCC and the estimated number of trips required during the pregnancy are depicted.
Most patients relied upon their partners to attend prenatal visits at home (76.2%, CI 71.9-79.9) and at our center (83.7%, 95% CI 81.9-88.5), provide emotional support (85.6%, CI 81.9-88.5), and provide support at home (72.3%, CI 67.9-76.2). Over one-third of respondents (37.5%, CI 32.9-42.3) were caring for one child and one-fourth were caring for ≥2 children (27.9%, CI 23.8-32.5). Most patients with other children (81.4%, CI 76.2-85.6) relied upon their partners or family to provide childcare assistance, resulting in childcare expenditures of <$100 for 82.9% of patients (CI 77.9-87). Most patients reported minimal to no perceived impact upon their relationships with partners and family related to care at our PFCC, but nearly half (47%, CI 32.8-54.2) described a moderate to severe adverse impact upon their other children.
Ongoing employment was reported by 79.8% of respondents (95% CI 75.6-83.4), with half reporting full-time employment (53.4%, CI 48.6-58.2). Ninety percent of partners were classified as working full-time during the pregnancy (92.5%, CI 89.5-94.7). Of the employed patients and partners, respectively, 42.2% (CI 37-47.6) and 41.6% (CI 36.8 36.8-46.5) missed 1-5 days, 17.7% (CI 14-22.2) and 22.4% (CI 18.6-26.8) missed 6-10 days, 8.9% (CI 6.2-12.5) and 11.3% (CI 8.6-14.9) missed 11-15 days, and 28.7% (CI 24.1-33.9) and 19.4% (CI 15.8-23.6) missed >15 days of work related to PFCC care. Only 5.3% of partners denied missing work related to this care (CI 3.5-8). In all, >40% of patients reported a moderate to severe negative effect on their employment or education related to care at our PFCC (41.6%, CI 36.8-46.5).
Over two-thirds of patients (68.9%, CI 64.2-73.2) stayed overnight in our city while receiving care at our center. Excluding patients who either lived within a reasonable driving distance or did not need to stay overnight, most respondents obtained lodging at a hotel (83.5%, CI 78.4-87.7) or at our local Ronald McDonald House (19.8%, CI 15.2-25.2). Nearly half of patients (45.3%, CI 39.8-50.9) received a recommendation to temporarily relocate nearer to our PFCC prior to delivery, but 28.6% (CI 21.6-36.8) were unable to comply with this request for reasons provided in Table 2. Of those who relocated, 23.4% (CI 15.3-34) spent <7 days in our city before delivering but 42.9% (CI 32.4-54) spent >28 days.
As seen in Figure 2, nearly half of the patients reported significant non-medical expenditures exceeding $1000 (42.6%, 95% CI 37.7-47.6), with nearly 1 in 10 reporting expenditures of >$5000 (8.6%, 95% CI 32-37.6). Figure 2 also outlines the primary contributors to these costs. Overall, 38.2% (95% CI 33.5-43.1) of respondents reported moderate to severe financial burdens related to receiving care at our PFCC. Patients traveling ≥50 miles to seek care at our center were more likely to report moderate to severe financial burdens related to this care than those traveling <50 miles (29.5%, CI 25.2-34.3 vs 9.7%, CI 7.1-13, p < 0.01).
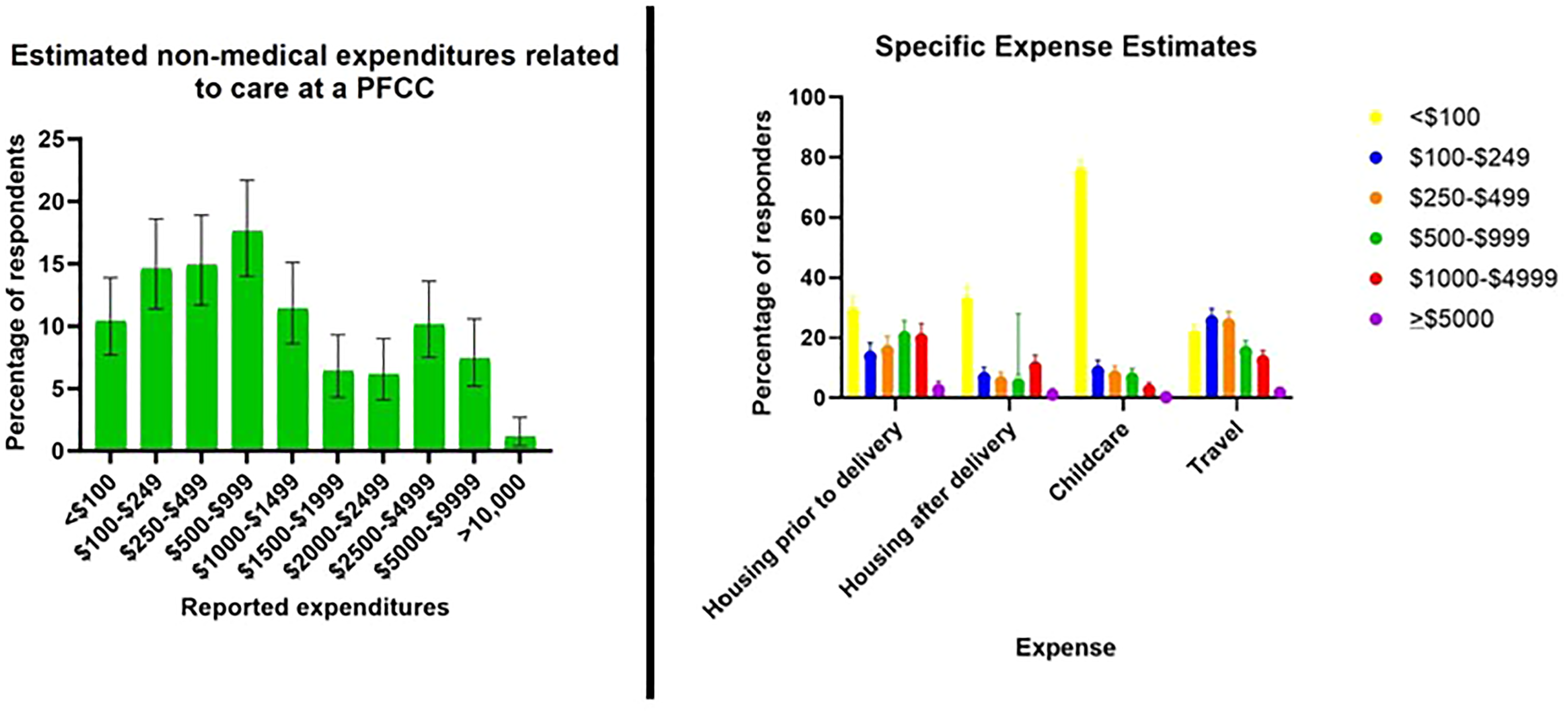
Non-medical expenditures related to care at a PFCC. The financial implications of care at a PFCC, including the overall non-medical expenditures during the pregnancy and the specific expense estimates related to housing, travel, and childcare are reflected.
Finally, in comparing responses according to SES, 101 patients were classified as being of lower SES (22.4%, CI 18.8-26.5), 300 as middle SES (66.5%, CI 62-70.7), and 50 of upper SES (11.1%, CI 8.5-14.3). Although estimates of non-medical expenses, the impact of care upon employment/education, and the distances traveled to our center were similar among the three groups, patients of lower SES were statistically more likely than those of upper SES to report moderate to severe financial burdens related to care at the PFCC (38.6% vs 10%, p < 0.01).
Discussion
To our knowledge, this is the first study to explore the financial, social, familial, and work-related burdens of care at a regionalized PFCC. More than 40% of patients reported moderate to severe financial burdens related to this care. An understanding of these non-medical burdens may allow us to better serve this vulnerable population.
Patients are referred to our PFCC following diagnosis of a myriad of fetal anomalies, genetic abnormalities, and/or complicated monochorionic gestations. Each patient referred to our PFCC must, at minimum, undergo a full day of advanced imaging, meetings with support staff and consultations with physicians. During this visit, we strive to provide an in-depth understanding of the plan for the pregnancy and delivery, the general plan for the care of the newborn, and the potential outcomes for the child.
Our primary referral area encompasses five neighboring states, but patients do not infrequently travel from more distant states to seek care are our PFCC. After their initial visit, most patients return to their primary obstetric providers for ongoing prenatal care, but many are advised to return to our PFCC for delivery to facilitate appropriate care of the neonate by pediatric providers. These latter patients may be asked to temporarily relocate to our city two to five weeks before delivery to ensure that unplanned deliveries may still occur in the vicinity of our children's hospital. For the patients who can stay at the local Ronald McDonald House or those whose insurance covers the costs of housing, the direct costs related to housing and/or meals may be subsidized, but this is not universally available and cannot account for other costs such as lost wages.
A large portion of the estimated costs were incurred related to travel, and, accordingly, patients traveling ≥100 miles to and from our center reported both higher non-medical expenses overall and higher expenses due specifically to transportation and housing. Evidence regarding the treatment of twin-to-twin transfusion syndrome suggests that neither travel by automobile nor airplane negatively impacts pregnancy outcomes, and some experts even argue that fetal care should be consolidated into a select few centers of excellence given that high volume and experience are both known to correlate with better survival rates.2,6–10 Regionalization of fetal care centers has thus been proposed as a potential way to improve outcomes for certain fetal/neonatal conditions. However, in a combined 2011 statement by The American College of Obstetricians and Gynecologists and the American Academy of Pediatrics regarding fetal care centers, concerns were noted that “limiting interventions to a few centers of excellence for the sake of quality of care will create both geographic and financial barriers to access,” and a recommendation was made to strive for a “balance of offering geographic access while having the quantity of cases necessary to develop clinical expertise and quality outcomes.”11,12
In 1996, The US Panel on Cost-Effectiveness in Health and Medicine urged researchers to explicitly comment upon the societal framework of their analyses, but many subsequent studies either failed to comply with this recommendation or omitted potentially important elements such as transportation costs or costs related to caregiver time.13–15 Analyses continue to focus on costs from a health system perspective while overlooking the societal effects. While studies have documented the financial stress of care in a NICU setting,2–4 our study is the first to explore the burden placed upon families who require specialized fetal care.
Further research is needed to better elucidate the financial, social, familial, and work-related effects of care of care at PFCC, including the effects of SES and race/ethnicity upon patient experiences. This work is ongoing at our center, with plans to conduct prospective assessments of these potential non-medical barriers to care. It is important that we also include patients in these analyses who are entirely unable to be seen at our center due to financial or social constrictions, as this may represent an especially vulnerable population.
Furthermore, a more complete exploration of these non-medical burdens would include a comparison of non-medical implications of care at a regionalized PFCC to care nearer to patient's homes. The increased monitoring and more intensive prenatal care recommended for these high-risk pregnancies may translate to significant burdens even if this care is provided locally. There is little data available in the literature regarding this, but our data demonstrates a higher financial burden for patients traveling <50 miles to our center than those traveling ≥50 miles. It is unlikely that burdens can be eliminated entirely given the need for such highly specialized and frequent monitoring, but future research should also be conducted to determine if reliance upon care by local providers can meaningfully decrease these burdens while still ensuring that an appropriate level of care and expertise is provided to this vulnerable population.
Our study suggests that burdens may be significant for some families, and these burdens may serve as barriers to care for some patients. Medical providers at PFCCs should be aware of these potential burdens, and attempts should be made to minimize these onuses. Collaboration with providers closer to patients’ homes may be the key to achieving this goal. Maternal–fetal medicine physicians are universally trained in ultrasound performance and interpretation, and they have the skills to perform the follow-up assessment of fetal well-being that is often recommended following consultations at a PFCC. The relationships between providers at a PFCC and local maternal fetal medicine specialists should be developed and maintained to best serve this vulnerable population of patients, minimizing unnecessary travel expenses and work absences through a collaborative approach among providers.
Limitations
There are a number of limitations inherent to survey-based studies, including recall bias and selection bias. We attempted to limit the effects of recall bias by excluding patients seen at our PFCC prior to 2015, but we recognize that estimates of expenditures may be vulnerable to memory degradation over time. Responses were relatively equally distributed according to the year that patients were seen at our center, but we recognize that patterns of response and/or nonresponse may differ when comparing patients seen more versus less recently. Although we attempted to mitigate the effects of selection bias by sampling a large number of patients, we obtained a poor response rate of only 15%. We hypothesize that the poor response rate may be related to lack of confidence regarding answers, particularly to some of the more specific questions, but it is also possible that patients were reluctant to recall a time that was fraught with anxiety or even a heartbreaking death of a child. Furthermore, white patients accounted for a disproportionate number of these responses, but we are unable to compare the demographics of the respondents to the demographics of the overall population served at our center, data that could prove useful in better analyzing the results of this survey. Finally, we employed income alone as an indicator of SES. To simplify answers for respondents, a cutoff of <$30,000 was chosen as the poverty line, but a more accurate cutoff of $26,500 may have been employed based upon data from the Department of Human Health and Social Services. Moreover, we recognize that a better estimate of SES would include other factors such as occupation and household composition.
Conclusions
While care at a PFCC may be necessary for optimization of pregnancy and neonatal outcomes in certain circumstances, the non-medical burdens, including financial implications and effects upon other children, can be significant. As we continue to expand our knowledge regarding these potential burdens, we can better address the barriers to such care to provide efficient and equitable care to all in need of such services.
Footnotes
Acknowledgment
The views expressed in this manuscript are those of the authors and not an official position of our institution(s).
Authors’ Contribution
The project was conceived by Kara Markham and the majority of the manuscript was written by this individual as well. Dr Gregory and Dr Abbasi were both intimately involved in the survey creation and interpretation of the results, and Dr Gregory also performed the statistical analyses of the data.
Consent to Participate
Written consent was not required, but patients provided consent for participation by agreeing to complete the study. Survey respondents first encountered an introduction section describing the purpose of the project, the potential risks, survey specifics, and the plan for data storage. Potential respondents were informed that, by choosing to start the survey after this introduction, they were consenting to participate in the study but could withdraw this consent at any time.
Data Availability
Data is available for review by editors, reviewers, and readers. The data is stored in both our SurveyMonkey project page and within an Excel spreadsheet owned by the authors of this manuscript. Further enquiries can be directed to the corresponding author.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study protocol was reviewed and approved by The Institutional Review Board at our institution, approval number 2021–0248.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.