
Abstract
Cognitive dysfunction (CD) is a common, impairing symptom experienced by persons with fibromyalgia (FM). This study explored how individuals with FM describe their experience of CD in an online peer support environment. Posts referencing cognitive symptoms were extracted from two Facebook FM peer support groups at two timepoints. Using inductive Thematic Analysis, key discussion themes were identified and compared across groups and time. Four themes represented the way members described their cognitive experiences in FM: understanding and describing CD experiences, distrust of cognitive abilities, choosing between pain and medication side effects, and misunderstanding and judgement from others. Two themes represented the impact of CD on members’ lives: impaired social interaction and loss of identity. Group members described broad impairments in daily functioning that significantly and negatively impacted their quality of life, indicating CD symptoms may play a more prominent role in the FM experience than previously understood. An infographic is included to aid patient education and help facilitate patient-provider discussions of CD symptoms.
Introduction
Fibromyalgia (FM) affects 2–4% of persons worldwide and is characterized by chronic widespread pain, fatigue, sleep disturbance, and mental health symptoms. 1 Most patients also experience and are distressed/impaired by cognitive dysfunction (CD; often referred to as “fibrofog”).2-4 Many factors likely contribute to FM-related CD including physiological overlap in cognitive processes and pain sensation detection mechanisms underlying pain processing,5,6 disturbed sleep, which even in the absence of pain, is associated with CD,7-9 comorbid mental illness, which can directly contribute to CD,10-12 and medication (eg, gabapentin, duloxetine) side effects.13,14
Researchers have identified impairments in concentration, verbal fluency, processing speed, short- and long-term memory, inhibitory control, and set shifting as common CD symptoms in FM.15-18 Although objective test findings verifying FM-related CD have helped legitimize cognitive complaints among this often-stigmatized population, they do not convey how patients experience the realities of life with CD. This lack of understanding may contribute to the disparity found between clinicians’ and patients’ treatment priorities, such that CD is often regarded as a low priority by clinicians, despite being considered a top priority by patients. 4 Thus far, CD has only been briefly mentioned in research concerning patient experiences of FM2,19 and patients’ understanding and experience of their CD has not yet been explicitly examined. 20
Improved understanding of patients’ lived experiences could enhance empathic, collaborative patient-provider relationships, which help foster patient empowerment and better adjustment to chronic illness.4,21 Improved understanding may also highlight accommodations health providers can make to better meet the needs of FM patients who may struggle to communicate their difficulties due to CD. Finally, given patients’ understanding of their difficulties influences adaptation and coping, improved understanding of patient experiences may provide insights relevant to why some patients are more engaged in illness-management than others.22,23 Thus, the purpose of this study was to explore how patients discuss their lived experiences of CD and its impact on their lives.
Method
Online peer support groups (OPSGs) provide a unique platform from which to observe how individuals with FM discuss their experience of CD and its impact on their daily lives. Observational data collected from publicly accessible OPSGs also allows researchers to minimize the burden of research participation on patients by utilizing data patients have already created. Given most persons with FM have experienced stigmatization or otherwise negative interactions with health providers, persons with FM may also feel most comfortable authentically discussing their experiences with peers. Thus, an observational methodology was employed in accordance with published guidelines for research in internet-based communities.24,25
Data Collection
The data used in this study was comprised of relevant excerpts of data from a larger dataset 26 (see Crump & LaChapelle, 2022 for full methodological details about data collection) as well as novel data collected using identical methodology two years after the first data collection period. Two time points were included to increase the trustworthiness of identified themes and to determine whether discussion themes changed over time as the membership of the group evolved. Further, given the recent proliferation of research concerning FM-related CD, we were interested in whether knowledge translation efforts have led to changing views among those living with FM. Data collection was undertaken following approval by the authors’ institutional Research Ethics Board. Given the observational approach used prevented the researchers from obtaining informed consent, careful consideration was given to ethical issues including consent and potential risk to participants to ensure compliance with article 10.3 of the Canadian Tri-Council policy statement on ethical conduct for research involving humans. 27 In accordance with Eysenbach and Till's 25 guidelines for discerning public versus private groups, each OPSG observed was publicly searchable, had at least 500 members, did not have posted rules to keep discussion content private, and could be accessed by simply clicking “join”. Detailed explication of how this research complied with the five conditions necessary to waive the requirement of informed consent by the Canadian Tri-Council policy is provided in Crump & LaChapelle. 26 The Tri-Council policy also requires research exempt from the requirement of consent to demonstrate potential benefit to participants, the population studied, or society in general. 27 The authors hope the current study may contribute to a better understanding of the lived experience of CD symptoms in the context of FM both for individuals with FM and health providers.
Sample/OPSG Members
Due to the non-interactive observational approach, verifiable demographic information about group members could not be collected. Based on the information posted (eg, pronoun use, profile photos), however, it appeared most group members identified as adult women/female (fewer than ten members identified as men/male). There appeared to be considerable variability in members’ ages, relationship statuses, spiritual beliefs, cultural backgrounds, and illness durations. Most members appeared to reside in North America with fewer than ten members indicating they lived abroad (eg, Europe, Australia, Africa).
Data Analysis
Discussion content collected from each group at both timepoints was substantial. Thus, a decision rule was developed to facilitate identification and extraction of content relevant to the question of how cognitive symptoms are experienced and described. To be included in this study's analysis, the poster or responder must have referenced cognitive symptoms (eg, attention, focus, concentration, memory, mental slowness, verbal fluency, fibrofog, or other common synonyms).
The first author initiated an inductive Thematic Analysis 28 of the extracted content using NVivo 12 Software. 29 First, she reviewed the excerpts from each OPSG and both time points repeatedly to familiarize herself with the data (Phase 1). Next, initial codes were generated in each group sequentially to describe patterns in the data (Phase 2). These codes were used to generate preliminary coding hierarchies within each OPSG and at each data collection timepoint. Codes were examined separately by OPSG and year first, then collated into potential themes (Phase 3). Themes in each OPSG were repeatedly evaluated and refined; no noteworthy differences were identified between OPSGs or across timepoints, which allowed for the construction of one unified thematic map (Phase 4). Finally, broad themes were defined based on the thematic map and underlying coding structure (Phase 5, 6). Repeated analysis of the data and discussion of alternative interpretations among the authors and with members of the research team were undertaken to ensure the trustworthiness of our findings. 30
Researcher Frame of Reference
The authors all have personal experience living with chronic pain within the context of the Canadian medical system and both coauthors have experience in the psychological treatment of pain conditions including FM.
Results
Review of data excerpts collected from both OPSGs at two time periods exactly two years apart revealed one group discussed CD more frequently, however, this group had more than twice as many members which may account for the differences in the frequency of relevant content. The content of discussions about CD did not differ thematically between groups or change notably over a two-year period. Four themes were identified that represented individuals’ cognitive experiences in the context of FM: (1) Understanding and describing CD experiences, (2) Distrust of cognitive abilities, (3) Choosing between pain and medication side effects, and (4) Misunderstanding and judgement from others. Two themes were identified that represented the impact of CD on quality of life: (1) Impaired social interaction and (2) Loss of identity (see Tables 1 and 2 for illustrative quotes/content from the OPSGs).
RQ1: How do Patients with FM Discuss Lived Experiences of Cognitive Dysfunction (CD)?

RQ2: How Do Patients Describe the Impact of CD on Quality of Life?

CD Experiences in FM
Understanding and Describing CD Experiences
OPSG members described experiencing one or several CD symptoms including perceived memory impairment and difficulties with speech, attention, and concentration, which impacted their ability to complete activities of daily living (eg, missed appointments, medication adherence) and interfered with parenting, work, or school obligations. CD symptoms were commonly described as chronic and sometimes progressive. Occasionally, members identified perceived causes of their CD including medication side effects, sleep disturbance, or pain. Most posts, however, did not label a perceived cause. Members frequently described struggling to articulate their experience of CD symptoms to people outside the OPSG.
Distrust of Cognitive Abilities
Consequent to their perceived CD, members described losing trust in their cognitive capacities, including their ability to retain memories and form new ones. To compensate for perceived deficits, members sometimes shared strategies to cope with CD symptoms such as note-taking to aid recall. Members frequently reminded each other to write notes prior to and during medical appointments as a compensatory strategy.
Choosing Between Pain and Medication Side Effects
Discussion content reflected members’ difficulty deciding between enduring the pain associated with FM or enduring the cognitively impairing side effects of medications. Content reflective of this theme included posts enquiring about other members’ experiences with specific medications and replies describing medication side effects. Members also described medication as futile due to its impairing side effects.
Misunderstanding and Judgement from Others
Members discussed feeling misunderstood and judged by society, their doctors, family, and friends because of their CD. Members noted it is hard for others to understand their experience and expressed gratitude for the OPSG, which allowed them to connect with FM-peers who understood and made them feel less lonely. Some members indicated a desire to share CD-related content from the OPSG to legitimize their experience and generate more understanding and compassion from others.
Impact of CD on Quality of Life
Impaired Social Interaction
Content reflective of this theme included members’ reports of difficulty following conversations due to CD symptoms and reported difficulties with speech production, comprehension, and word recall, which impaired their ability to sustain in-person conversations. As a result of this perceived difficulty, some members indicated they withdraw from conversations when they experience CD symptoms. Despite wanting social contact, some members described the cognitive effort of conversations to be overwhelming.
Loss of Identity
Discussion content reflected group members’ perceived loss of identity or reduced capacity to be the person they used to be due to CD symptoms. Some members discussed losing their ability to work due to CD, resulting in a perceived loss of a valued identity component. Members also described feeling unable to engage in previously cherished hobbies/activities (eg, knitting, reading) because they were unable to concentrate enough to engage in these activities. Some members also described fear and despair associated with forgetting important moments that gave meaning to their life narrative or helped define important aspects of their identity (eg, mother, family member).
Discussion
To the authors’ knowledge, this is the first qualitative examination of patient's perceptions of CD in FM OPSGs. Observing discussions within a peer-based online environment provides a novel perspective on persons with FM's CD experiences distinct from interview or survey-based studies. Insights from OPSG environments may be useful to identify whether peer- versus researcher-led discussions about FM-related CD converge on the same ideas, in keeping with a patient-centered approach.
Discussion content of the OPSGs was thematically consistent across both time points, two years apart, suggesting a lack of major advancements in treatment of CD symptoms in recent years. Four themes characterized the way individuals described their experience of CD (understanding and describing CD experiences, distrust of cognitive abilities, choosing between pain and medication side effects, misunderstanding and judgement from others) and two themes characterized the impact of CD on their lives (impaired social interaction, loss of identity).
Consistent with previous research,15,18 OPSG members described experiencing impaired speech, attention, concentration, memory, verbal fluency, and processing speed. Group members expressed resistance to taking pain medications because they produced or exacerbated CD symptoms and resulted in various negative impacts on their quality of life. This finding suggests patients with FM do not always prioritize pain management over CD management and lends credence to previous research that has indicated individuals with FM regard CD as a top concern when seeking treatment despite the lesser emphasis placed on CD by clinicians and researchers.4,18
Group members described difficulty comprehending and articulating their experience of CD, perhaps as a direct result of their CD. This is an important finding because difficulties in effectively communicating experiences to friends, family, and healthcare providers can have several negative consequences. First, it may create suspiciousness about the legitimacy of patient's symptoms, thereby adding to the stigmatization experienced by those with FM. 1 Indeed, perceived lack of support and compassion was a common motivator for joining the OPSGs. 26 Second, this study's findings suggest CD may be an overlooked barrier to the benefits of social interaction, which is often encouraged as a method to improve quality of life among patients with chronic pain. 23 For example, OPSG members indicated CD symptoms impacted their ability to communicate, rendering social contact overwhelming and disheartening. Members described withdrawing in response to social difficulty, which may lead to social isolation, loneliness, and increased vulnerability to concurrent psychological disorders.31,32
The experience of CD symptoms and difficulties with communication appeared to contribute to members’ distrust of their cognitive abilities and increased reliance on OPSGs for social interaction. By communicating asynchronously, members avoid the demand that in-person socializing places on cognitive resources; they can take time to formulate responses and choose not to respond when experiencing heightened CD symptoms. While the reduction in cognitive demand may be desirable, individuals may inadvertently increase the severity of their CD via deconditioning of the cognitive skills necessary for in-person social interaction. 22 Furthermore, while OPSGs may be beneficial for providing support and reducing loneliness, they are not a permanent solution nor an equal alternative to in-person social contact.24,32
This study's findings also suggest CD symptoms are uniquely devastating in that they challenge an individual's capacity to retain a valued sense of identity and self-continuity (ie, the connection between a person's past and present selves). 33 Members described difficulty creating and recalling memories of important life events (eg, child growing up, personal milestones) since developing FM, which appeared to challenge their sense of identity (eg, parent, employee), and generate fear and despair. For some, the experience of identity loss was described as more difficult to manage than pain. This is an important consideration given clinicians tend to prioritize the treatment of FM symptoms such as pain, sleep disturbance, and psychological disorders over CD, likely with the expectation that treating these symptoms will improve CD indirectly. 4 Unfortunately, these findings suggest CD symptoms may be contributing to increased psychological stress, which is associated with increased pain, sleep disturbance, and CD.23,34 From this perspective, prioritizing treatment of some patients’ CD symptoms and its impact on identity may be vital to their FM-management.
Clinical Implications
Based on these findings, health providers are encouraged to discuss CD symptoms with patients to help understand and prioritize treatment targets and accommodate cognitive difficulties. A FM-specific CD infographic was developed based on the literature and included within this publication (see Figure 1) as an educational tool and resource to stimulate discussion with FM patients about the CD symptoms they experience. With limited time available during appointments, this infographic may benefit both clinicians and patients by prompting points of discussion. Self-report checklists are also an effective tool for stimulating discussions about CD symptoms because they emphasize recognition rather than free recall abilities (eg, Multiple Abilities Self-Report Questionnaire, 18 Multidimensional Inventory of Subjective Cognitive Impairment 35 ).
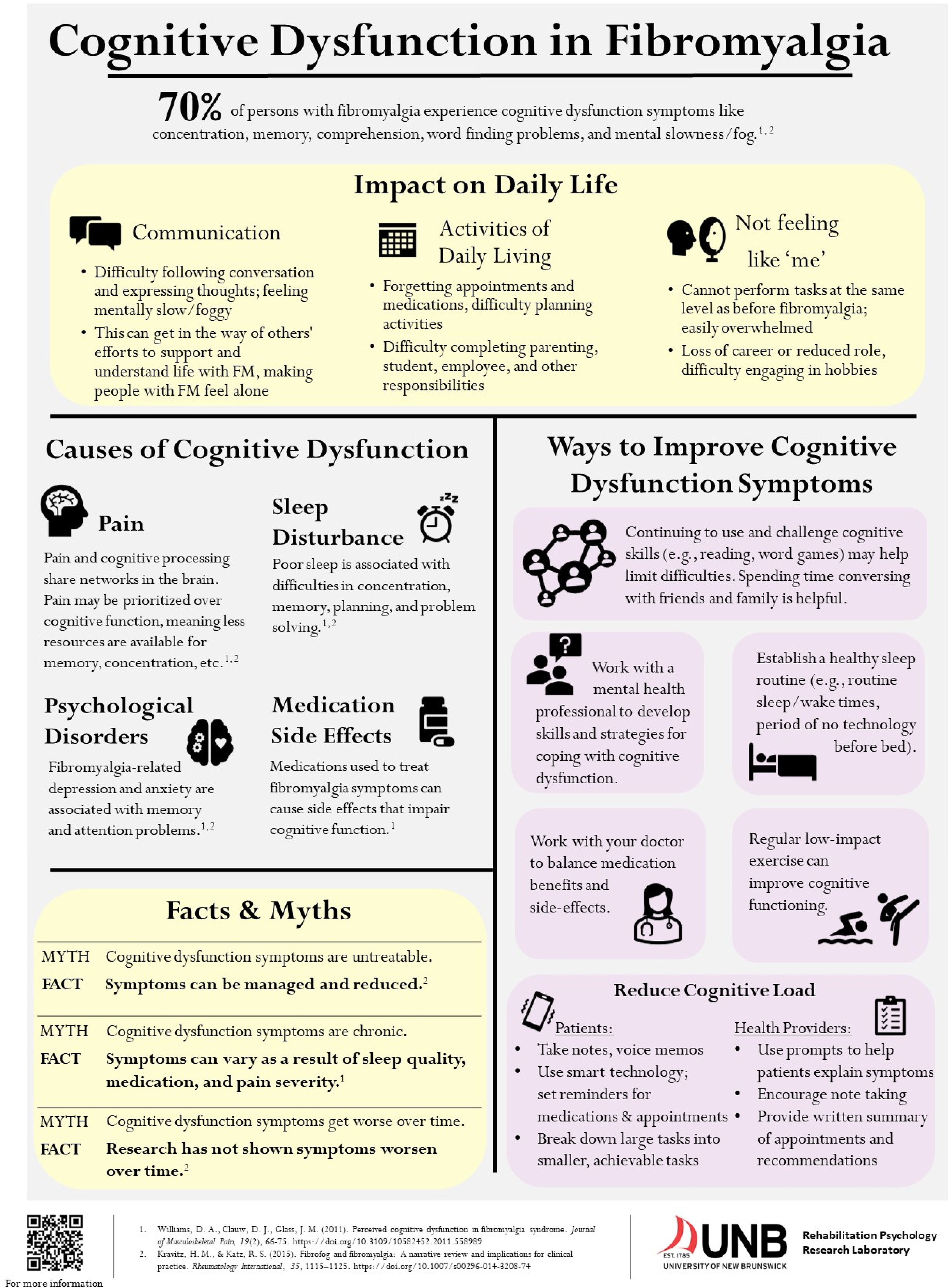
Educational infographic for FM-related CD to aid health care workers in providing patient education and facilitating discussions of cognitive symptoms.
Prescribing professionals and pharmacists would also benefit from regularly assessing and discussing the costs and benefits of medications (including their impact on cognitive functioning) with patients. Our findings suggest patients often engage in this analysis on their own and with peers. This may be especially important for patients deemed nonadherent; efforts to avoid CD symptoms may better explain nonadherence than patient resistance. Such discussions may indicate the use of assistive technology (eg, calendars with appointment/medication reminders) could improve patient adherence. It may also be useful to provide written treatment recommendations and encourage patients to record voice memos/take notes during appointments to improve their ability to recall important information. Patients can also be provided with the infographic, which includes further suggestions to reduce cognitive load and manage CD symptoms.
Finally, mental health and allied health professionals are encouraged to integrate techniques to develop and improve cognitive skills into their treatments for FM. For example, they might encourage engagement in low-impact exercise with a cognitive component (eg, Tai Chi) and mindfulness meditation which appear to be effective in improving cognitive functioning.36,37 Similarly, social engagement provides opportunities for social support and is associated with improved cognitive functioning. 36 It is important to emphasize, however, that intervention needs to be individualized given the cause and presentation of CD will vary across patients.
Limitations and Future Research
The use of a non-interactive, observational approach facilitated examination of the ways individuals with FM describe their CD experiences in a peer-to-peer rather than researcher-led environment. This was useful for gaining insight into members’ perceptions while minimizing the potential influence of socially desirable responding, which can occur in studies where the presence of the researcher is known.24,38 This approach, however, prevented collection of specific demographic information, follow-up inquiry about specific topics related to CD, and member checking the identified themes. Future research using an interactive approach would be useful for gaining more insight into patients’ perceived causes of CD.
It would also be valuable to examine the effectiveness of interventions such as cognitive rehabilitation and assistive technology (eg, electronic planners, alarms/reminders) to compensate for some of the difficulties imposed by FM-related CD. Both are commonly recommended and effective for individuals who suffer a traumatic brain injury, which can precipitate CD symptoms similar to those experienced by individuals with FM (eg, impaired attention/concentration, memory, communication, and mental slowness). 39
Additional research examining other sex and gender identities would also be useful given most of the discussion content reviewed was posted by individuals who presented as women/female. Thus, the assumed transferability of these findings to persons with FM with other sex and gender identities is discouraged. The potential impact or role of culture, race, and other identities within persons with FMs’ discussions of CD was also beyond the scope of this study; examination of these identities would help to extend the current understanding of patients’ experiences.
Conclusion
Group members described broad impairments in daily functioning that significantly and negatively impacted their quality of life, mental health, and social functioning, indicating CD symptoms may play a more prominent role in the FM experience than previously understood. Focused treatment of CD may be vital for coping with FM and its’ associated symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a Canadian Institutes of Health Research Canada Graduate Scholarship (Doctoral) and New Brunswick Innovation Foundation Doctoral Scholarship awarded to Lyndsay Crump and by the Harrison McCain Foundation Young Scholar Award presented to Diane L. LaChapelle. These supporters were not involved in the study design or in the collection, analysis, and interpretation of the data.
Key Findings
Comorbid CD may complicate FM treatment and reduce the effectiveness of standard treatment approaches. CD challenges individuals' capacity to engage in social activities and uniquely contributes to a sense of identity loss and associated distress, which has serious implications for patients' mental health, coping, and quality of life. Focused treatment of CD may be vital for coping with FM and its' associated symptoms.