
Abstract
Telehealth provides greater opportunity for specialty access but lacks components of the physical exam. Point-of-care ultrasound (POCUS) may assist telehealth as a visual substitute for the provision of palpation. We conducted a prospective observational pilot project to survey oncologists about (1) their expectations of POCUS, (2) their use of POCUS in oncology telehealth visits, and (3) post-project assessment of their experiences. The results of the pre-assessment survey showed an interest among the oncologists in the ability to evaluate structures remotely via POCUS. POCUS was utilized in 6.4% of visits, most commonly for lymph node assessment (60% of use). POCUS was not utilized most often due to not being applicable to the patient's visit. There were 14 instances of technical issues limiting views of the relevant anatomy reported. Oncologists rated the use of POCUS as very satisfied or satisfied in the vast number of recorded responses. This pilot study suggests POCUS can be integrated into oncology telehealth visits for specific applications such as lymph node assessment. The surveys indicated a potential interest and positive responses that provide for the foundation of expansion to subspecialty care access for patients with telehealth supported by POCUS.
Key Points
Telehealth lacks components of the physical exam which are important in areas of subspecialty care to provide a full assessment and expand subspecialty care to remote regions.
Point-of-care ultrasound (POCUS) was of interest to oncologists in assessing lymph nodes and was used for this purpose in remote area telehealth.
POCUS could benefit from additional studies to effectively target patients who are likely to benefit from this assessment for oncology and, potentially, other areas of telehealth.
Introduction
Telehealth has rapidly evolved over the last decade. It allows providers to reach patients from the comfort of the patient’s home as well as provide specialty services to critical access regions
In parallel with telehealth, POCUS use has grown rapidly over the past 2 decades, allowing physicians the ability to directly visualize anatomy, physiology, and pathology. 1 Ultrasound can be used in the diagnosis of palpable disease and for image-guided biopsies.2,3 Metha et al 3 found that ultrasound detected additional cervical nodes not detected by clinical examination. With evolving technology, POCUS opens the door for visual supplementation of the physical exam.
We hypothesized the feasibility of POCUS to improve physical assessments and clinical video telehealth visits at remote clinics.
Methods
We performed an observational project with a convenience sample of local oncologists and a remote oncology clinic using pre-, intra- and post-project survey assessments. We conducted semistructured interviews with open-ended questions and Likert-like scales to understand acceptability, feasibility, and barriers among stakeholders (leadership, oncologists, and telehealth nurse practitioners) (Table 1). We asked what they thought of adding ultrasound into the exam: benefits, risks, feasibility, and the reasons for their answers. The questions were developed in conjunction with our implementation science (IS) specialist (EPF), based on IS methodology. 4 However, as the use of POCUS in telehealth medicine for oncology is not currently considered a standard of care, this project was not a true IS study but rather a pilot assessment for the feasibility of this novel application within the context of telehealth.
Qualitative Comments From Semistructured Interviews Among Telehealth Oncology Stakeholders.
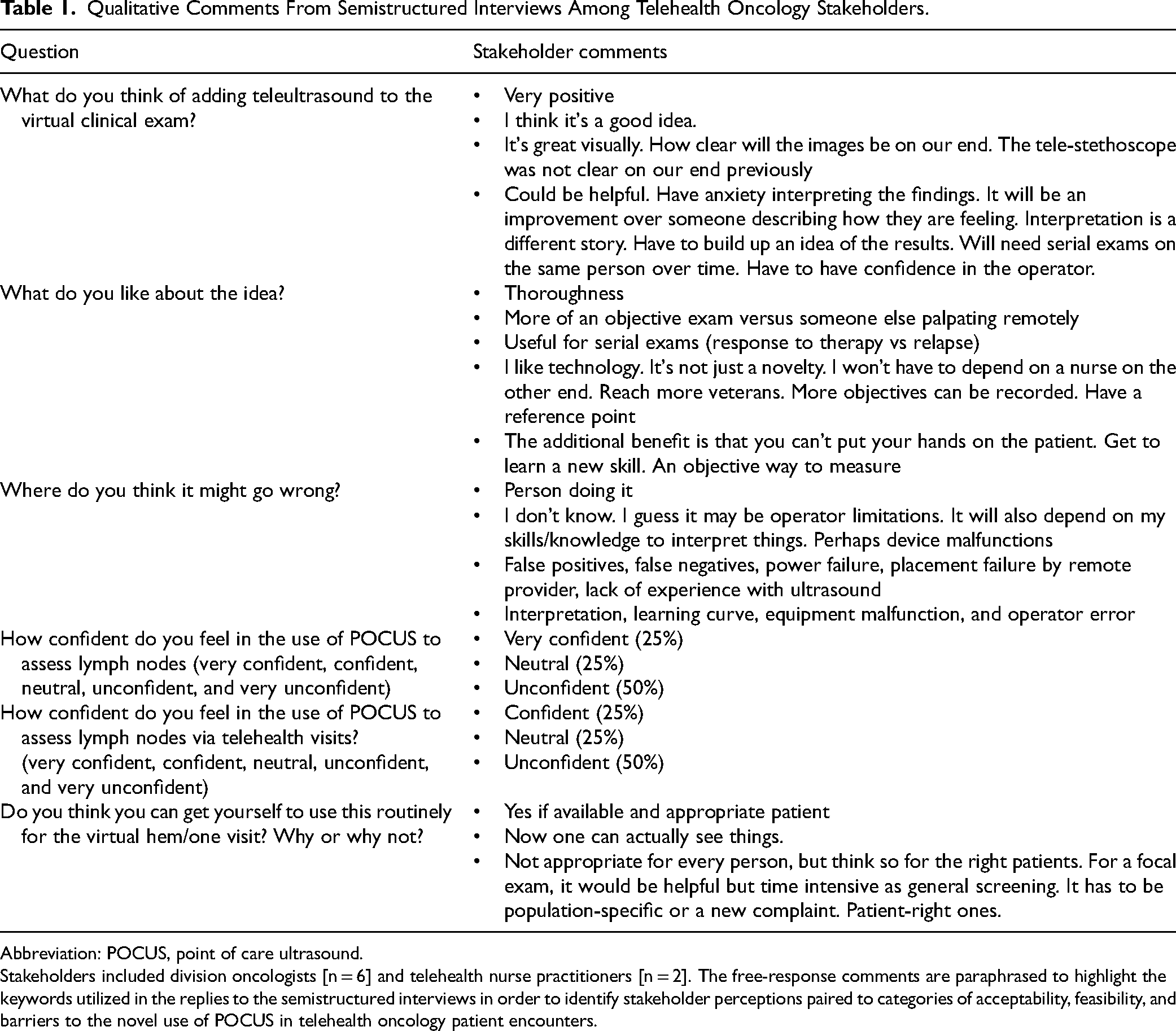
Abbreviation: POCUS, point of care ultrasound.
Stakeholders included division oncologists [n = 6] and telehealth nurse practitioners [n = 2]. The free-response comments are paraphrased to highlight the keywords utilized in the replies to the semistructured interviews in order to identify stakeholder perceptions paired to categories of acceptability, feasibility, and barriers to the novel use of POCUS in telehealth oncology patient encounters.
A subject matter expert (SME) (CKS) with over 10 years of experience teaching POCUS provided initial education in the use of POCUS, with a specific focus on the evaluation of lymph nodes. The SME provided education to both the staff at the local hospital (Pittsburgh, PA) (oncologists, n = 6) and the staff at the remote facility (Altoona, PA) (nurse practitioners [NPs], n = 2). Education was provided to every provider who interacted with patients both locally and remotely. All staff at each site volunteered to participate in this training, serving as a convenience sample. The learners were provided with pre-reading textbook chapters, articles, and prerecorded videos. The SME then met with each provider to demonstrate the use of the POCUS device for image acquisition and interpretation of the relevant anatomy. They continued to use the device for practice during the initial training period. The device was subsequently delivered to the remote site, where the SME provided education, remotely, to the remote site's NPs for device use, interface with the telehealth software, image acquisition and interpretation, to mirror the patient visit experience. During this time, the project leaders and SME would check in to see how comfortable the Pittsburgh providers and Altoona NPs felt with using POCUS, providing any additional training as needed.
Ultrasound examinations were performed by telehealth NPs at the Altoona clinic with the oncologists located in Pittsburgh during a predetermined 6-month pilot period. Each patient visit could be included as an encounter for potential use of POCUS. Teleultrasound was conducted using a Philips Lumify High-Frequency Linear probe (L12-4, 12-4 MHz; Philips North America Corporation, Andover, MA, USA) with remote connectivity through Reacts software (Reacts by Innovative Imaging Technologies, Inc., Montreal, Quebec, Canada). The oncologist in Pittsburgh helped direct the NP to perform the exam in real time during the synchronous telehealth visit.
Upon completion of each clinic visit, the oncologists and the Altoona NPs were asked to complete an after-visit survey (Surveymonkey.com, Momentive Inc, San Mateo, CA). (Supplemental Table 1) There were monthly check-ins with the Pittsburgh oncologists and the Altoona NPs, encouraging the use of POCUS in each visit and inquiring about barriers to implementation. In response to feedback during the interim check-ins, the SME provided additional training for musculoskeletal and deep venous vascular applications via the same educational methods done previously.
After completion of this 6-month pilot, each of the same oncologists (n = 6) and telehealth NPs (n = 2) completed another semistructured interview asking about their experiences. These questions were also developed in conjunction with our IS expert (Supplemental Table 2).
The information from the pre-study training sessions, after-visit surveys, and post-study interviews were gathered and summarized. We performed descriptive analysis on the frequency of POCUS use as well as factors regarding satisfaction, ease of use, pertinence to clinic visits, and barriers to POCUS implementation.
This project was approved as nonresearch Quality Improvement (QI) by the VA Pittsburgh Healthcare System IRB.
Results
The pre-study responses demonstrated that the oncologists were excited about this new technology, specifically as an objective element to the exam. Half of the respondents initially felt unconfident about the use of POCUS to assess lymph nodes via telehealth visits (Table 1).
Between June and December 2021, there were a total of 422 video telehealth visits for the oncology department between Pittsburgh and Altoona. Of these visits, there were 326 after-visit surveys completed by Altoona NPs and 28 from the Pittsburgh oncologists, resulting in 326/422 (77.3%) visit encounters that logged an after-visit response regarding tele-POCUS use. POCUS was used 21/326 (6.4%) times (Table 2). The most common reason for not using POCUS was “not applicable to the patient's presentation/visit” at 94.4% (288/305). Each of the taught exam types was performed: lymph nodes (60%), musculoskeletal (26.7%), and lower extremity venous (13.3%). 100% of the Altoona team's responses stated “I was able to clearly see all relevant anatomy.” Of the 326 logged encounters, there were 14 technical issues reported (13 instances of connectivity issues and 1 device malfunction, assuming the same instance was reported by the MD and NP) (Table 2). Of 21 Altoona team responses, 20 stated they were “very satisfied” (85.7%) or “satisfied” (9.5%) with using POCUS during that visit, reflecting their level of enjoyment with this novel exam.
After Visit Survey Responses.a
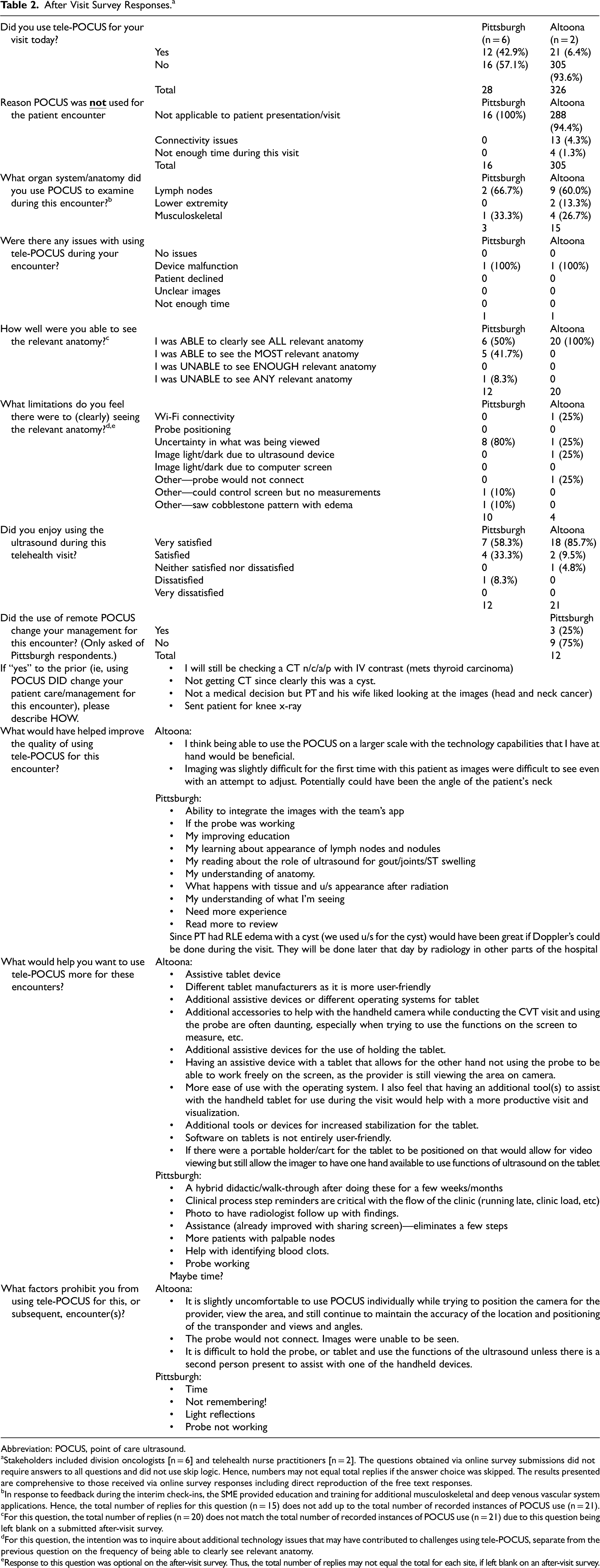
Abbreviation: POCUS, point of care ultrasound.
Stakeholders included division oncologists [n = 6] and telehealth nurse practitioners [n = 2]. The questions obtained via online survey submissions did not require answers to all questions and did not use skip logic. Hence, numbers may not equal total replies if the answer choice was skipped. The results presented are comprehensive to those received via online survey responses including direct reproduction of the free text responses.
In response to feedback during the interim check-ins, the SME provided education and training for additional musculoskeletal and deep venous vascular system applications. Hence, the total number of replies for this question (n = 15) does not add up to the total number of recorded instances of POCUS use (n = 21).
For this question, the total number of replies (n = 20) does not match the total number of recorded instances of POCUS use (n = 21) due to this question being left blank on a submitted after-visit survey.
For this question, the intention was to inquire about additional technology issues that may have contributed to challenges using tele-POCUS, separate from the previous question on the frequency of being able to clearly see relevant anatomy.
Response to this question was optional on the after-visit survey. Thus, the total number of replies may not equal the total for each site, if left blank on an after-visit survey.
Five of the 6 Pittsburgh oncologists had used POCUS during at least 1 telehealth encounter, resulting in 12 logged after-visit survey responses. These survey results demonstrate that they were able to see all or most of the relevant anatomy in 11/12 instances (91.7%), although with uncertainty in what they were viewing in 8/10 (80%) responses. They rated the use of telePOCUS as “very satisfied” (7/12, 58%) and “satisfied” (4/12, 33%) with only one (1/12, 8%) “dissatisfied.” 3/12 (25%) stated that remote POCUS changed management. Not having direct applicability to the patient's reason for their visit was the most common factor identified as prohibiting the use of telePOCUS by the physicians.
Comparing the data from both Pittsburgh oncologists and Altoona NPs, we believe that the 28 after-visit responses from Pittsburgh were included in the 326 from Altoona. During our check-ins and interviews, it was apparent that the faculty at Pittsburgh would not consistently remember to record their results via the SurveyMonkey link, particularly when POCUS was not utilized. We chose to use the data from the Altoona clinic, as it was entered more consistently. Thus, we felt this would be a better reflection of the frequency and indications for use, while the data from Pittsburgh reflected the local physicians’ perception when POCUS was utilized.
The results of the post-pilot semistructured interviews demonstrated that oncologists were able to use POCUS during remote encounters (Supplemental Table 2). Both the physicians and the telehealth team recommended additional training beyond the initial sessions. The telehealth team reported anecdotal comments that patients and their caregivers expressed liking the addition of the POCUS during the clinic visit.
Discussion
The results of this pilot project suggest that POCUS can be used as an adjunct to the physical exam for telehealth encounters. Pre-survey results showed that our local oncologists were excited about the opportunity to use telePOCUS as an adjunct to remote patient encounters. POCUS was able to be utilized in 21 patient visits during this project's pilot period. When applicable, POCUS was able to be used to clearly visualize the desired anatomy with infrequent device malfunction. The qualitative feedback demonstrates that the participants felt its integration was beneficial when needed, requesting additional training to improve the speed or efficiency of use. Based on our aim to evaluate the feasibility of incorporating POCUS into telehealth encounters, we interpreted our results as demonstrating that it can be done. However, additional work would be needed for improved implementation.
At present, there is a paucity of studies on the use of teleultrasound to augment the physical exam in the outpatient setting. Courreges et al 5 reported a small study where robotic teleultrasound provided care in a secondary hospital or isolated healthcare settings with an 83% agreement between the remotely obtained diagnosis and one performed directly on-site with the patient. We believe that our work adds to the literature that it is feasible to use POCUS for specific applications during telehealth patient encounters.
There continues to be a need for access to subspecialty care. The 2018 National Oncologists Workforce Study asserts that by 2025 the oncologist shortage will increase to 2200 oncologists. 6 Access to oncologic care is likely to be disproportionately sparser in rural areas. In January 2018, VA Pittsburgh created a Virtual Cancer Care teleoncology clinic in Altoona where video telehealth continues to be used to deliver oncology care for rural veteran patients. Patients reported high levels of satisfaction related to their experiences with the virtual clinic. The teleoncology remote clinic markedly reduced travel costs and time for veterans who previously would have commuted from central Pennsylvania to Pittsburgh for their oncology care. 7 Thus, the addition of POCUS has the potential to help expand subspecialty care access for patients living in rural areas or when access to care may be limited.8,9 With the rapid expansion of teleoncology and more recently with all telehealth during the COVID-19 pandemic, we expect that POCUS will be an adjunct option for future virtual or remote patient encounters.
TelePOCUS's largest role may be in patient satisfaction. Anecdotal comments from both the Pittsburgh oncologists and Altoona NPs providers stated that patients enjoyed being able to visualize what was being palpated and felt that they were becoming more informed about their disease, findings consistent with the use of POCUS during in-person encounters.10,11 However, this should be better assessed with future studies.
Limitations
The most notable limitation of our project is the potential for reporting bias due to low survey completion by the oncologists' side compared to the responses completed by the Altoona team. Additionally, we were limited only to the evaluation of superficial anatomy, given the properties of the high-frequency linear probe utilized in our study. The low incidence of POCUS use for superficial structures may also reflect that this portion of the physical exam was not needed, even if it would have been an in-person encounter. Perhaps having additional probes for deeper anatomy assessment would have better alignment with the physical exam components during these visits. This could be an opportunity for future study.
Conclusions
This pilot project suggests that the integration of POCUS into telehealth visits is feasible, based on our limited project population. This provides the foundation for further studies on implementation across other specialties with the aim of expanding subspecialty care access for patients via video telehealth visits.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231224516 - Supplemental material for The Feasibility of Using Point of Care Ultrasound as a Visual Substitute for Physical Examination During Telehealth Visits: A Pilot Project
Supplemental material, sj-docx-1-jpx-10.1177_23743735231224516 for The Feasibility of Using Point of Care Ultrasound as a Visual Substitute for Physical Examination During Telehealth Visits: A Pilot Project by Vida C. Passero, Nicole Conley, Erin P. Finley and Christopher Kevin Schott in Journal of Patient Experience
Supplemental Material
sj-docx-2-jpx-10.1177_23743735231224516 - Supplemental material for The Feasibility of Using Point of Care Ultrasound as a Visual Substitute for Physical Examination During Telehealth Visits: A Pilot Project
Supplemental material, sj-docx-2-jpx-10.1177_23743735231224516 for The Feasibility of Using Point of Care Ultrasound as a Visual Substitute for Physical Examination During Telehealth Visits: A Pilot Project by Vida C. Passero, Nicole Conley, Erin P. Finley and Christopher Kevin Schott in Journal of Patient Experience
Footnotes
Acknowledgments
The authors wish to thank the VA Pittsburgh Healthcare System. This material is the result of work supported with resources and the use of facilities at the VA Pittsburgh Healthcare System, Pittsburgh, PA.
Author Contributions
All authors participated in the research and preparation of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimers
The opinions expressed in this article do not reflect those of the Veterans Healthcare Administration.
Ethical Approval
Ethical approval is not applicable to this article. This project was approved by the VA Pittsburgh Healthcare System IRB as nonresearch Quality Improvement.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Department of Veterans Affairs, Veterans Research Foundation of Pittsburgh Medical Education and Patient Safety (MEPS) Grant. None of the funding agencies supporting this work were involved with the study design; collection, analysis, and interpretation of data; writing of the report; or the decision to submit the article for publication.
Informed Consent
There are no human subjects in this article and informed consent is not applicable.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the VA Pittsburgh Healthcare System IRB-approved protocols as nonresearch Quality Improvement.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.