
Abstract
Patients benefit from and appreciate the option to use telehealth with their providers. Such patient expectations have therefore led to new questions about the factors that affect providers’ willingness to adopt telehealth as part of their clinical practice. We interviewed 19 physicians across four specialties with differential rates of telehealth use (Psychiatry, Anesthesiology, Physical Medicine & Rehabilitation [PM&R], and Ophthalmology) to discern the barriers and incentives to telehealth adoption among physicians. We then conducted a qualitative analysis of interview transcripts, following precepts of Directed Content Analysis. Conclusions drawn from matrix building and thematic analysis were verified with negative evidence searches and if-then tests. Robust investigations for outliers and rival explanations in responses were used to disconfirm findings. The results of this analysis revealed distinct barriers and incentives to telehealth adoption for the four specialties. Physicians in psychiatry and anesthesiology are refining the strengths and applications of telehealth based on the characteristic needs of their specialties. Physicians in PM&R and ophthalmology face additional barriers to acquiring physical exam data, leading them to use telehealth as a supplement to, rather than as a replacement for, core functions of patient care. The insights stemming from these barriers and incentives can be used to build thoughtful telehealth applications for physicians, allowing them to provide effective clinical care while also improving the patient experience.
Introduction
“Telehealth” is defined as the delivery of healthcare, health education, and health information services via remote technologies. 1 As an umbrella term, telehealth can embody many different use cases, including remote patient monitoring, online patient education materials, and clinical video visits.2–4 The rapid adoption of telehealth across the United States in 2020 was born out of necessity, but its expansion has continued across the country. Currently, more than 80% of US hospitals connect with patients using telehealth video visits and other connected technologies, 5 and patients and providers have expressed high rates of satisfaction in domains such as general surgery consultations, diabetes glycemic control, and outpatient radiology.6–9 Since patients benefit from and appreciate the option to use telehealth with their doctors, the present research explores barriers and incentives to physician telehealth adoption, which has important implications for improving overall patient experience.
Increasingly, physicians are considering the safety, convenience, adherence, and efficacy of telehealth. For example, in a review of the telehealth adoption literature, Rush et al 10 found that telehealth was useful for promoting rural older adults’ health in a meta-analysis of 42 studies, while evidence for ease of use was mixed. A meta-analysis of 66 studies on telehealth for chronic pain patients found that barriers included technological challenges and limited digital literacy, while incentives included convenience and progress tracking. 11 There are clear benefits and challenges to telehealth, and both physicians and their patients are interested in identifying the proper circumstances to improve patient experience and outcomes.
Columbia University Irving Medical Center (CUIMC) ramped up its video visits and its telehealth infrastructure to serve patients when the pandemic began. 5 Telehealth video visit utilization is recorded for internal quality purposes through CUIMC's multispecialty Faculty Practice Organization (FPO). This data has the total number of telehealth video visits conducted by 20 specialties across CUIMC, as well as the percentage of total visits that were conducted via telehealth. In 2021, FPO Data revealed large differences in the percentage of telehealth video visits by specialty (see Table 1).
Fourth Quarter (Q4) 2021 Data Across 20 Specialties in the Faculty Practice Organization.
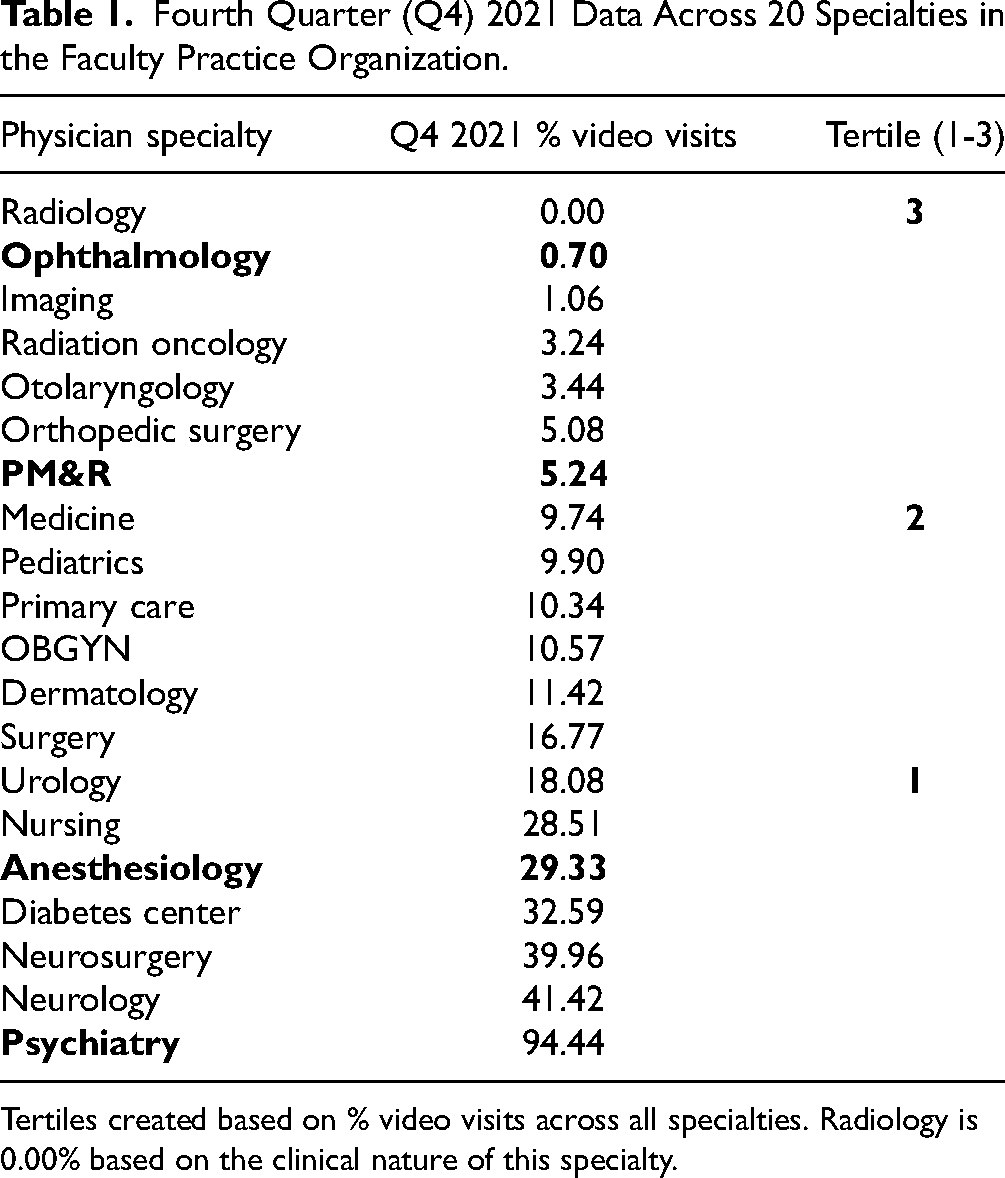
Tertiles created based on % video visits across all specialties. Radiology is 0.00% based on the clinical nature of this specialty.
The present qualitative research study, wherein “telehealth” has been defined as virtual video visits unless otherwise noted, was conducted to ensure physicians from diverse specialties across CUIMC had their voices and clinical perspectives on telehealth elevated, so that any barriers or incentives for telehealth adoption are fully understood from a community context. As they are responsible not only for their patients’ health but also for ensuring their patients can meet with them according to preference and ability, physicians have a particularly deep perspective on the use of telehealth for patient care. The present study offers crucial insights to physician leaders, administrators, policymakers, and technology creators, and it elucidates barriers and incentives for physician telehealth adoption. If physician experiences with telehealth are better understood and improved, the overall patient experience and associated quality metrics may be improved as well.
The value of such clinical perspectives is clear from previous literature. For example, physicians may notice that their disadvantaged or older patients require different directions or infrastructure to use a mobile application for telehealth visits.12,13 Or they may appreciate that available telehealth capabilities are not well aligned with a particular specialty's clinical practice.14,15 It is therefore imperative that, as virtual clinical practice continues to evolve to better suit patient needs, and as technologists and researchers continue to refine these digital tools, physicians engage in honest discussion about telehealth adoption. With an eye on the patient experience implications of increasing the availability of telehealth, the present research uses qualitative methods to elucidate the incentives and barriers to telehealth adoption among physicians in four medical specialties.
Methods
Population Sample
Research participants were licensed and board-certified physicians working at CUIMC. Participants’ ages ranged from 35 to 65 years. The physicians worked in the departments of Anesthesiology (n = 4), Psychiatry (n = 4), Physical Medicine & Rehabilitation (PM&R) (n = 6), and Ophthalmology (n = 5). These four specialties demonstrated robust outpatient volumes in the fourth quarter (Q4) of calendar year 2021: Anesthesiology with 1807 encounters; Psychiatry with 23,689 encounters; PM&R with 9264 encounters; and Ophthalmology with 15,425 encounters. Housed at a large quaternary academic medical center in New York, NY, all specialties boast outpatient and inpatient service lines for both adult and pediatric patients. These specialties were selected from the first (Anesthesiology and Psychiatry) and third (PM&R and Ophthalmology) tertiles for the highest and lowest telehealth utilization, respectively, based on Q4 2021 FPO data from CUIMC. Physicians from the first and third tertiles were deliberately selected to ensure that diverse and representative perspectives were elicited while also maintaining study design efficiency and limiting time obligations for these working professionals. Four to six physicians were interviewed per specialty to achieve thematic saturation for the research question. 16 The study was approved by the Columbia University Institutional Review Board.
Intervention
Investigator AL contacted CUIMC physicians via purposeful sampling. The duration of physician interviews ranged from approximately 15 to 30 minutes. AL conducted semistructured interviews with a 5-question script (Supplement A), allowing physicians to discuss topics not included in the script. Interviews were conducted via secure video call. No audio or video files were recorded; only a text transcript from the video call was saved for subsequent qualitative analysis.
Data Organization and Analysis
Internal and external code generation followed Directed Content Analysis, whereby review of telehealth adoption and healthcare incentive strategy helped create 28 codes defined before and during analysis.17–20 Two codes (“Cardiology” and “Primary Care”) were not frequently discussed by physicians during semistructured interviews, and so, based on the open coding principle of “making the codes fit the data, rather than forcing the data into the codes,” they were removed from the final assessment of qualitative themes.21,22
Interview responses provided by physicians were saved as text transcripts, entered into NVivo 12, and coded line-by-line in 3 passes. 23 To achieve rigorous organization in coding, the first pass consisted of assigning descriptive codes that summarized the topic of the data—similar to surface-level keyword tagging. 24 We decided a priori that our descriptive codes (and two main themes) would consist of Barriers and Incentives given the purpose of the research. For example, the response “I do think telehealth bridges barriers that would prevent people from being able to follow up otherwise” received a code of Barrier. The second pass followed, with interpretive codes that reflect a deeper level of context and seek to explain the concepts contained within the data. The same response above was coded as Perspective during the second pass. The third pass used focused coding to categorize previously coded data based on thematic similarity; for example, Perspective was categorized under Barrier. 24 NVivo was used to enable this multipass organization and the resulting thematic analysis across all physician specialties.
Written analytic memos were completed after each coding round to interpret themes developing in the data. Noting patterns and resultant themes is a method of extracting data; exploring contrasts and comparisons tests the conclusions and practical significance across specialties. To verify conclusions drawn from matrix building and thematic analysis of codes, two tactics were used: looking for negative evidence and making if-then tests. First, looking for negative evidence is a natural complement to the method of drawing conclusions through patterns described above. Outliers and rival explanations were actively sought in the interview responses to disconfirm findings. Second, making if-then tests formalizes propositions for testing in the responses. For example, “If the interview response is marked with the Commute code, then they are more likely to have faced cost barriers.” In summary, descriptive, interpretive, and focused coding developed categories that were sorted, grouped, and synthesized into themes through matrix building; themes were then verified by the conclusion strategies (Table 2).
Third-Pass Code Organization Within the Barrier and Incentive Themes (see Supplement B for Full Table).

Results
We organized our findings first by specialty and then by the themes of Barriers and Incentives in accordance with the cross-case analysis inherent in the study design. Coding themes are shown in diagrammatic form as well (Table 3).
Themes and Subthemes for Barriers and Incentives Grouped by Specialty.

Abbreviation: PM&R, Physical Medicine & Rehabilitation.
Psychiatry
Barrier: Highly Acute Conditions Are Inappropriate for Telehealth
When discussing telehealth, psychiatrists commented on the interplay between the severity of a patient's condition and the acuity of the patient's required care. Severity, as formulated by the interviewees, referred to the seriousness of a patient's condition, whereas acuity referred to the level of immediate patient needs. Psychiatrists commonly expressed willingness, ability, and comfort with managing patients across a range of disease severity, such as mild to severe major depressive disorder, via telehealth visits. In contrast, they were less comfortable managing high-acuity conditions via telehealth, such as a patient noting intermittent acute suicidality. In such a case, the patient was felt to be better served by seeking immediate help at a healthcare facility that can provide needed support and safety provisions. “We did make a medication change. I think that the positive factors are having an ongoing established relationship and knowing the patients well. Regarding my own patients, they're not in an acute emergency, which I think would change the equation.”
Incentive: Telehealth Expands Access to Psychiatrists
Despite the monitoring barriers mentioned above, psychiatrists were often incentivized to use telehealth because of the access to care it provided their patients. While these psychiatrists acknowledged their initial concerns about care quality differences between in-person and telehealth visits, they (and their patients desirous of telehealth) ultimately found them to be effective and sufficient. An unexpected benefit and added incentive for psychiatrists was found in telehealth's ability to offer a previously unseen window into the patient's life. Psychiatrists, for example, detailed situations where patients’ home lives were highlighted in telehealth visits. “I have a patient, and their face lights up when the dog walks into the room. It's an aspect of the interaction and the meaning of this pet, and I never saw that [before telehealth]. In the same way, seeing people interact with their babies, a powerful thing to be able to witness is how they relate. Especially the postpartum period, that's a very valuable thing to be able to observe.”
Anesthesiology
Barrier: Current Telehealth Tools Are Not Designed With the Anesthesiologist in Mind
Barriers for anesthesiologists are summarized as a mismatch between their purpose-built clinical tools and day-to-day work. Of note, the anesthesiologists interviewed were hospital-based and did not have outpatient practices. Day-of needs included in-person physical exams to evaluate a patient's airway access, and informative discussions to counsel them on the anesthesia process. When anesthesiologists were asked to explore their most obvious needs—and whether or not telehealth could provide a solution—they focused on visualization of the airway. Although Mallampati scores, a ubiquitous airway classification system used to predict the ease of intubation, have been gathered via telehealth visits, these scores alone were not, in fact, the highest priority. Indeed, there are other important factors (that are often easier for anesthesiologists to assess in person) that are highly influential in determining a general versus spinal anesthesia route, a key decision point for the practicing hospital-based anesthesiologist. “We want to see the airway, but that's not the only thing we need. Really, the extent of mouth opening—-whether the person has a larger chin or not, whether they have a bigger neck—-is really more indicative of problems. I can see this just walking past the patient… So if I see someone, for example, and I’m going to do a hip replacement, and I see the airways are not going to be easy, I might gear them more and get them ready for spinal as a better option than general anesthesia.”
Incentive: Telehealth Can Assist With Pre-Operative Coordination
The incentives for telehealth adoption among hospital-based anesthesiologists are derived from their indirect interface with resulting data. At CUIMC specifically, anesthesiologists work with the Anesthesia Perioperative Evaluation and Exam (APEX) Clinic. APEX is a perioperative telehealth clinic operated by anesthesiologists, nurses, nurse practitioners, physician assistants, and anesthesiology residents. Pre-operatively, APEX serves a dual function: as a consult clinic for surgeons to receive anesthesiology endorsement of a patient's fitness for procedure, and as a proactive chart review system. The latter function has APEX members perform chart review of upcoming surgery patients, and, if further evaluation is needed, APEX will reach out to the patient for more information and/or pre-operative testing. Without the telehealth APEX Clinic, anesthesiologists felt like they would be at a clinical disadvantage. “It would mean that we would be much less equipped to have acceptable clinical data for patients coming for surgery or procedures. So we depend on that heavily for assessment of their comorbidities, medications, and problems they've had in the past with anesthesia care. So we rely a lot on that pre-operative assessment that is primarily done by telehealth.”
Physical Medicine & Rehabilitation
Barrier: The Physical Exam Must Be Included for Diagnosis
Telehealth barriers for physiatrists relate to the integral and hands-on nature of their physical exam. PM&R is a specialty that aims to enhance and restore the movement and function of people who have lost such abilities due to disease or injury. Interviews highlighted the importance of the initial in-person visit and evaluation. An in-person visit was deemed so crucial that the physiatrists interviewed have all developed a personal rule to never evaluate a new patient via telehealth. The exception to this rule would be a patient who had already obtained a full work-up and imaging from a fellow physiatrist or neurological specialist; otherwise, the in-person evaluation is essential to clinical diagnosis and planning. For example, a patient presenting with left-sided spine pain requires a thorough history and exam to distinguish between different spinal levels, muscular versus neurological etiology, extent of injury, red flag findings, and more. While the history can provide many critical pieces of information, the physical exam often serves as the lynchpin in PM&R. “The physical exam is a necessary component of evaluation better served in person… Eighty percent of your diagnosis comes through history, but that doesn't mean the 20% that comes from the physical exam is worth the sacrifice.”
Incentive: Follow-Up Appointments Are Often Appropriate for PM&R Telehealth
In contrast, the physiatrists emphasized the increase in communication touchpoints and check-ins facilitated by telehealth, offering not only a clinical incentive, but also an efficiency incentive. In the interviews, physiatrists expressed appreciation for the ability to use telehealth for follow-up visits after an initial in-person encounter. The follow-ups ranged from image review and medication management to orthotics maintenance and pain control. “So, for example, [with] any injection or shoulder injection and to be able to, without bringing them into the clinic, have a revisit with them, and get a sense of how the intervention had gone, usually at a one- or two-week interval. This was helpful.”
Ophthalmology
Barrier: Core Tools and Physical Exam Maneuvers Are Excluded From Telehealth
Ophthalmologists, like physiatrists, depend heavily on the physical exam. Furthermore, they have a suite of specialized tools that are not currently amenable to telehealth-based care. Without these tools, the ability to diagnose and devise treatment plans is severely limited. For example, two interviewed ophthalmologists who treat glaucoma referred to the necessity of tonometry to detect changes in eye pressure. They do not have the capability to measure eye pressures during a telehealth visit, and their patients do not have a tonometer they can self-administer. More generally, ophthalmologists use slit lamps to visualize the front of the eye and inside the eye; again, interviewed ophthalmologists stated self-administration of a slit lamp exam was not possible and extremely impractical. Dependance on such a suite of tools means that telehealth visits fail to provide substantive data to the physician. “An iPhone is not going to really help… I don’t feel it offers me tools that will in any way make my exam more useful… Magnification is big and the most important.”
Incentive: Specialty Alignment With Innovation Is Conducive to Efficient Use Cases
Incentives that drive the use of telehealth in ophthalmology were certain triage and follow-up appointments for specific patient populations. Specific patient populations amenable for ophthalmological care via telehealth include cosmetic surgery candidates, routine eye care patients, and those with seemingly emergent but low-risk conditions (e.g., a broken blood vessel in the eye causes subconjunctival hemorrhage, which patients often think is an emergency, but interviewed ophthalmologists noted is usually harmless and can be triaged relatively easily via telehealth). “Patients call me up. It sounds like they're ready to have a stroke because they're so scared. And I say, ‘send me a picture.’ And with a simple iPhone picture, in seconds or minutes I can say ‘relax, breathe, it's nothing’… And there are a few things I can handle like that.”
Discussion
Barriers and incentives to telehealth adoption for our interviewed physicians are summarized in Table 3. Reflecting telehealth's challenges and benefits for both physicians and patients, these specialty-specific subthemes help explain rates of physician adoption of telehealth and the subsequent patient experience that results. Telehealth provides another access channel for a physician's existing patients and an entirely new method of access for first-time patients. With psychiatry, for example, expanded access to mental healthcare is possible largely because of the diminished reliance on an in-person physical exam. Literature has now shown the efficacy of telehealth psychiatric care.25,26 For example, Bulkes et al 25 reported results of a nation-wide retrospective analysis that demonstrated no significant differences between those who had received telehealth versus in-person care with respect to depression and quality of life metrics.
In stark contrast, PM&R requires a hands-on approach to tease out subtle findings from multiple body systems, and to forego this exam is to ignore critical data. While tens of millions of dollars have been invested to find ways to interrogate musculoskeletal conditions via telehealth,23,27 our study's physiatrists articulated a concern that telehealth tools are likely to be unhelpful to their work.
Ophthalmologists are similar to physiatrists in their need for specialized exams and tools. Whereas the physiatrist has ultrasound diagnostics and hands-on maneuvers, the ophthalmologist relies on imaging machines and handheld tools to examine the eye, such as fundoscopes, slit lamps, and tonometers. These tools help make a definitive diagnosis and develop a treatment plan. While there are many new telehealth-enabled technologies and care models seeking to change how the ophthalmologist can provide patients access to this information, they are not widespread or inexpensive. For example, an at-home tonometer can cost around $1000. 28 This price makes ophthalmology telehealth prohibitive for most patients who require regular tonometry for glaucoma. Relatedly, interviewed physicians were wary of these at-home tools and desire validation studies.
For anesthesiologists, the power of telehealth comes from the ability to ensure adequate pre-operative coordination. With telehealth, an anesthesiologist can screen appropriate candidates, identify red flags, and make the day-of operation or procedure more safe and efficient by preventing medical exacerbations or providing patients with a realistic plan. 27 Literature also shows that pre-operative telehealth evaluation (versus in-person evaluation) is associated with shorter hospital length of stay for certain patients, and that telehealth antenatal anesthesia consultations offer the same standard of care for such consultations.29,30
As described above, our research identified the core barriers to telehealth adoption for a variety of physicians, highlighting how they currently worked around these barriers. This research also identified ways in which telehealth is not user-friendly for physicians. For example, all interviewed specialties faced the challenge of patients being unable to log in to the telehealth platform, with a common workaround being conversion of the video visit into a telephone visit. 31 A telephone visit can be useful for information gathering, but it precludes any image review or visual data collection. Another cross-specialty challenge was the operationalization of telehealth for clinical practice, a finding echoed in the literature across American Medical Association, American Hospital Association, and Uniformed Data System analyses.32–34 Interviewed physicians expressed the need for clear guides, use cases, and protocols for triage, screening, and evaluation via telehealth. Without such a telehealth playbook, physicians are often left working individually. Those specialties where telehealth utilization was lower, such as PM&R and ophthalmology, may benefit from devising ways to employ telehealth that account for the specific considerations of those fields. Addressing these barriers and incentives in physicians’ workflows may promote wider telehealth adoption and improve patient experience.
Limitations
This study included physicians that were part of CUIMC. Different physicians in other medical systems may have provided responses in different ways or could have had different insights on the barriers and incentives to telehealth adoption. Assessments of other healthcare stakeholders such as nurses were not explored. Different healthcare systems may have different levels of financial and clinical resources available for telehealth implementation and use.
Conclusion
The insights from this research suggest clear pathways for improving patient experience by promoting intelligent telehealth adoption. Physicians in psychiatry and anesthesiology, first tertile telehealth use departments, are refining the strengths and applications of telehealth based on the characteristic needs of the specialties. Physicians in PM&R and ophthalmology, third tertile telehealth use departments, face additional barriers concerning physical exam data and currently use video visits as supplementary to, rather than as a replacement for, core functions of patient care in their specialties. Each of our 19 interviewed physicians contributed direct needs and recommendations based on personal interactions with their patients via telehealth. These insights should be used as a guide to build thoughtful telehealth applications for physicians so that they may continue to treat their patients safely, effectively, and conveniently, improving their overall experiences in the process.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735241310961 - Supplemental material for Improving Patient Experience by Understanding Barriers and Incentives to Telehealth Adoption Among Physicians at a Large Academic Medical Center
Supplemental material, sj-docx-1-jpx-10.1177_23743735241310961 for Improving Patient Experience by Understanding Barriers and Incentives to Telehealth Adoption Among Physicians at a Large Academic Medical Center by Alessandro Luna and Taylor B Sewell in Journal of Patient Experience
Footnotes
Acknowledgments
We would like to thank the Columbia University physician interviewees for participating in this research. We would also like to thank the Columbia University staff and department heads for facilitating this research.
Author Contributions
AL conceptualized the study, interviewed the participants, analyzed the data, and drafted the manuscript. TS assisted with the study's conceptualization, provided local telehealth data to inform study processes, and critically revised and edited the manuscript.
Availability of Data and Materials
The datasets generated and analyzed during the current study are not publicly available to maintain privacy of participants; relevant de-identified data and analyses are included in the manuscript.
Declaration of Competing Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AL provides consulting services to Regeneron Pharmaceuticals; and he is founder of Maiv Health Inc., a company building digital diagnostics.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AL was funded by National Medical Fellowships grant.
Ethics Approval
This study was approved by the Columbia University IRB (protocol #AAAU1775) on April 24, 2022.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Columbia University Institutional Review Board approval for protocol #AAAU1775.
Statement of Informed Consent
Informed consent was not required by the Columbia University IRB, though participants were told that the confidential responses they provided were being used as part of a survey review on barriers and incentives for telehealth adoption.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.