
Abstract
This study's objective was to determine how frontline physicians perceived telehealth for older adults with sensory impairments, cognitive impairments, mobility challenges, or those receiving end-of-life care. We conducted a multiple-methods study of US emergency, geriatric, and primary care physicians. Phase 1 involved semi-structured interviews with 48 physicians on their experiences using telehealth with older adults. In phase 2, we used those qualitative findings to generate a web-based survey administered to 74 physicians. In phase 3, we reintegrated qualitative data to enrich survey results. We identified 3 key findings: (1) 50% of emergency physicians, 33% of geriatricians, and 18% of primary care physicians considered telehealth to be a poor substitute for providing end-of-life care (p = .68); (2) for hearing, vision, and cognitive impairments, 61%, 58%, and 54%, respectively, saw telehealth as a good or fair substitute for providing care (p = .14); and (3) 98% indicated that telehealth was a good or fair substitute for in-person care for those with mobility impairment (p < .001). Preferences and comfort using telehealth with older adults vary by clinical context, patient population, and physician specialty, requiring tailored adaptations.
Introduction
The abrupt onset of the COVID-19 pandemic in the United States in March 2020, led to a large-scale decrease in in-person healthcare, coupled with a corresponding and unexpected growth in telehealth (1,2). Due to concerns with COVID-19, a nationally representative survey found that approximately one-quarter of Medicare beneficiaries, the population disproportionately affected by this disease, reported forgoing medical care during the summer of 2020 (3). Telehealth has become an important means of healthcare delivery given it reduces travel burden and increases efficiency and flexibility for this patient population (4). From May 2019 to June 2020, older adults’ care providers who offered telehealth visits increased from 14% to 62% and participation in telehealth visits increased from 4% in May 2019% to 30% in June 2020 (5).
Unfortunately, older adults face unique challenges with telehealth. When older adults were surveyed about their most common concerns with telehealth, they cited a lack of a physical exam (75%), perceived lower quality (67%), less connectedness to health provider (75%), difficulty seeing or hearing the clinician (25%), and privacy (25%) (5). Research has further demonstrated that these patients’ concerns are validated by the design challenges for telehealth systems development to account for a myriad of age-related issues, including cognitive deficits, physical impairments, including dexterity and facility with technology, as well as difficulties hearing or seeing on small screens, and inexperience with technology that could all serve as barriers for older adults (6). Previous qualitative work with physicians working with older adults by our group highlighted barriers to telehealth including (a) the capacity to use telehealth modalities, (b) the need for alteration of care delivery mechanisms, and (c) the need for team-based care including multiple specialties and caregivers (4,7,8). We noted through this work that older adults are a heterogeneous group and specific adaptations to telehealth delivery are necessary depending on the clinical scenario and patients’ specific impairments. The aim of this paper was to better understand and quantify these qualitative findings.
Objective
During the COVID-19 pandemic, physicians throughout the United States have increasingly adopted telehealth. This presents unique challenges and opportunities to expand access to care for older adults. We developed a national survey based on previous qualitative results (4,7,8). This survey was designed to assess how frontline physicians perceived telehealth for older adults with hearing impairments, vision impairments, cognitive impairments, and mobility challenges, and for those receiving end-of-life care.
Methods
Study Design
We conducted a web-based cross-sectional national survey of US geriatricians, primary care physicians (PCPs), and emergency medicine (EM) physicians. This survey was created using previously conducted semi-structured interviews and a process of iterative feedback as described in Supplemental Text S1. The survey took approximately 8 min to complete during testing and had 36 questions in 7 sections. The full interview guide can be found in Supplemental Text S2.
The survey was distributed in 3 waves between August and November 2021. It captured data relevant to physicians’ perceptions and experiences with methods of telehealth delivery, barriers and challenges to telehealth adoption, and experiences with providing remote care to older adults. Additionally, we estimated the scope of telehealth use during the COVID-19 pandemic and moving forward. Consistent with the American Telemedicine Association's definition, we defined telehealth in our survey as “the use of technology to conduct patient visits remotely, and can include audio-only visits, audiovisual visits, messaging via patient portals or chat-based applications, use of remote monitoring devices, and email or voice messages” (9). We followed the Checklist for Reporting of Survey Studies for reporting web-based survey findings (10). The principal investigator's institutional review board approved the study (1598592).
Study Population
Study-eligible physicians were licensed to practice in the United States in EM, geriatrics, or primary care (internal medicine or family practice). They also needed to have cared for patients 65 years and older (with or without COVID-19) in person, over the phone, or virtually during the COVID-19 pandemic.
Participant Recruitment
We aimed to reach at least 1% of each physician specialty's national membership to approach a representative dataset; geriatricians (5,598 [n = 56]), PCPs (113,514 [n = 1,134]), and EM physicians (42,348 [n = 423]) (11). We solicited physicians through the American Medical Association's (AMA) Physician Masterfile, the most comprehensive list of US physician contacts. We used Redi-Data, Inc., an authorized AMA database licensee, to distribute the survey. With simple random sampling, we selected physicians who were sent an email inviting them to participate, as well as 2 reminder emails. To increase the number of respondents, 3 separate waves of emails were sent out to providers identified from the AMA Physician Masterfile. Physicians were informed prior to participation that they could choose to input their email into a separate, second survey to enter a raffle for a $50 gift card (n = 57 winners). Finally, after the last wave, we also opened recruitment via social media though there was no additional interest in this form of recruitment.
Analytics
We used descriptive statistics to summarize participant demographics, practice features, modes of communication, and facilitators and barriers to telehealth use. Missing values were assumed to be missing completely at random and an available-case approach was taken. All statistical analysis was done in Stata 15.1 (12). Finally, survey findings were enriched by returning to the qualitative data from the first phase of the study to provide illustrative quotations and context (13).
Results
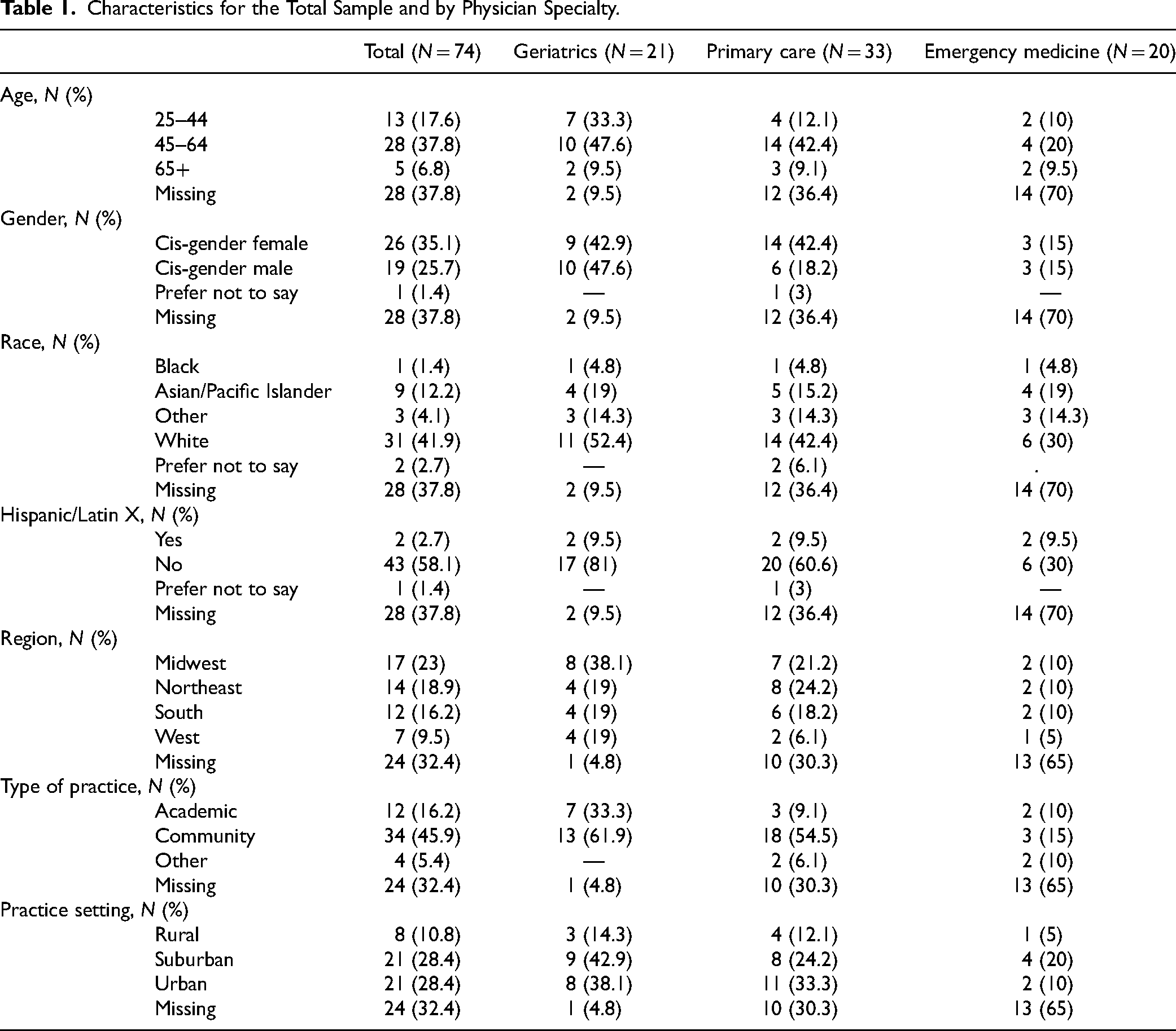
In total, 15,000 physicians were invited to participate via email in 3 waves each with 1 reminder email. A total of 75 physicians consented to participate in the survey, with 74 total physicians (geriatrics [n = 21], primary care [n = 33], EM [n = 20]) answering at least 1 survey question. Surveys were completed in a median of 3.7 min. The median age was 50% and 35% (n = 26) were women. Thirty-four practiced in community settings (46%) and 21 (28%) practiced in urban areas (Table 1).
Characteristics for the Total Sample and by Physician Specialty.
Most physicians (91.5%) thought telehealth helped older patients “Somewhat” or “To a great extent” receive care during the pandemic they would not otherwise receive. Most physicians (83.7%) were also “Somewhat” or “Very likely” to provide medical care for older patients via telehealth after the pandemic. A large number, though fewer, of physicians (48.8%) were “Somewhat” or “Very likely” to increase their use of telehealth for older patients after the pandemic.
How physicians perceived telehealth as a substitute for in-person visits varied by the patient population being served. 63% of physicians saw telehealth as a “Poor substitute” or “I would never use it for this situation” for patients with hearing impairment while 99% of physicians saw telehealth as a “Fair substitute” or “Good substitute” for patients with mobility impairment. How telehealth was perceived by physicians also varied by topic and specialty. For example, for end-of-life care, 50% of EM medicine physicians saw telehealth as a “Poor substitute” while 76% of PCPs saw telehealth as a “Fair substitute” or “Good substitute” (Figure 1). In the setting of the emergency department and unexpected illness, explaining end-of-life care through a telehealth mechanism was not seen as effective by many physicians. On the other hand, advanced care planning in a nonurgent setting via telehealth was seen as an avenue to grant patients access to these important conversations. Illustrative quotations for these survey results are summarized in Supplementary Table S1.

Survey responses to (A) “To what extent is telehealth a substitute for in-person visits for provision of care to persons with” and (B) “To what extent is telehealth a substitute for in-person visits for end-of-life care?”
The top 4 strategies supported by physicians for increasing access to telehealth for older adults included assessing the ability to use technology before an appointment (42%), helping patients with technology during an appointment (43%), providing multiple options to communicate (e.g., doxy.me, zoom, and telephone) (42%), and requesting caregiver help (39%). The top 3 policy barriers included restrictive licensure (eg, need for different state licensure to practice across state borders) (34%), low reimbursement (34%), and limited access to broadband for patients (30%).
Discussion
In this national survey of U.S. geriatricians, PCPs, and EM physicians, we identified key populations and clinical scenarios when telehealth would be most effective as well as the most important barriers that need to be addressed by policymakers and physicians to improve access to telehealth. Specifically, we found that the vast majority (98%) of physicians saw telehealth as a realistic substitute for in-person visits for older adults with mobility impairment. For these patients or those with difficulty finding transportation, televisits may be the only option for patients and their families to get any access to care. Physicians deemed telehealth of limited utility for patients with hearing and vision impairment.
Similarly, Lam et al (14) found that 13 million older adults in the United States were not ready for video visits; citing reasons of “unreadiness” to include difficulty hearing well enough to use a telephone, difficulty seeing the television, possible dementia, not owning or being unable to use internet-enabled devices, or “no use of email”, texting, or internet in the past month.
Telehealth may never be a viable option for certain “unready” patients. However, through our previous qualitative work, we have identified solutions to increase readiness that have face validity as well as anecdotal success among survey participants (4). This includes solutions such as those highlighted in our survey. For example, it will be key to address technological barriers in the patient population by assessing patients’ ability to use technology before the appointment or helping them during the appointment, as well as providing multiple options depending on their comfort with specific communication modalities. Arighi et al (15) found that the presence of a younger caregiver with an older adult with dementia increased success connecting for televisit (p < .001, odds ratio [OR] = 5.14). Increased access to broadband will also be essential moving forward; for example, a 2018 study found that 26.3% of Medicare beneficiaries did not have digital access and this was higher among those with lower socioeconomic status, those over the age of 85, and those in communities of color (16).
Unique to the current study, we found that specific conversations may not be best addressed on a televisit. For example, in the emergency department during an unexpected, high-pressure, and emotional end-of-life conversation, telehealth was seen as a poor substitute for in-person care. On the other hand, end-of-life conversations in the setting of lower acuity visits were seen by geriatricians and primary care providers as an improvement in care.
Limitations
Although this is a national study of frontline physicians using the AMA Physician Masterfile, which is the most extensive list of US licensed physicians available, our results are limited by a low survey response rate, 0.49% (74 of 15,000). Physicians often have a low web survey response rate (17). The COVID-19 pandemic also created additional strain on the healthcare system which likely lowered willingness to respond even further from conventional rates. A recent study found a drop in survey response rates in the COVID-19 era by 15 percentage points within the neurosurgery literature specifically (18). We tried to combat these challenges with recruitment incentives for participation, outreach via listservs in 3 recruitment waves with 2 reminder emails, and outreach via social media. We were, however, able to get a relatively even number of each specialty type. Further, when surveys were completed, many of the variables were missing values including demographics as well as the key information. This is likely also related to the survey fatigue by physicians during the COVID-19 era that led to low response rates. Additionally, our sample included only physicians; other stakeholders such as patients, caregivers, other providers, and staff can also provide valuable and unique insights regarding telehealth. Characterizing other affected stakeholders’ viewpoints is a key next step for future research.
Conclusions
Preferences and comfort using telehealth with older adults vary between emergency, geriatric, and PCPs. Telehealth may be more appropriate for certain populations, such as older adults with mobility challenges, but less suited for clinical contexts such as end-of-life conversations in the acute setting. Specific clinical contexts and patient populations will require tailored telehealth adaptations to ensure physicians can provide high-quality care. Policymakers and administrators should consider physician comfort with telehealth and patient-specific needs, particularly for vulnerable older adults, as they start to expand telehealth programs.
Supplemental Material
sj-docx-1-jpx-10.1177_23743735231160418 - Supplemental material for Physician Views of Telehealth for Special Populations of Older Adults: Preliminary Findings
Supplemental material, sj-docx-1-jpx-10.1177_23743735231160418 for Physician Views of Telehealth for Special Populations of Older Adults: Preliminary Findings by Peter T Serina, Natalie M Davoodi, Kate M Guthrie, Roland C Merchant and Elizabeth M Goldberg in Journal of Patient Experience
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This work was supported by the National Institute on Aging (Grant/Award Number: K76 AG-059983).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.