
Abstract
Dispositional gratitude has been negatively associated with perceived stress (PS) and positively associated with higher well-being in both general and chronically ill people. Attempts to understand the relationship between gratitude and aspects of quality of life (QOL) have been documented; however, there is limited research on determining the potential mediating effect of PS on gratitude and QOL factors in individuals with Multiple Sclerosis (MS). In this cross-sectional study, participant demographics, dispositional gratitude, PS, and QOL factors were collected online via self-report measures from a sample of 68 participants diagnosed with MS. Results indicated that both dispositional gratitude and PS were associated with aspects of QOL and that PS was found to partially and indirectly account for the relationship between gratitude and improved QOL. Findings are consistent with existing research conducted with non-chronically ill samples. Clarifying relationships between PS and dispositional factors in MS is necessary to inform future interventions aimed at maintaining and enhancing an individual's QOL.
Multiple sclerosis (MS) is a progressive neurological disease in which the immune system attacks myelin in the central nervous system. It is estimated that approximately 2.8 million people worldwide live with MS. 1 MS is differentiated by other neurological disorders by its early disease onset, symptom variability, and unpredictable course. Given such disease aspects, MS patients are likely to face a broad spectrum of physical, emotional, social impairments and stressors that may compromise quality of life (QOL), 2 such as lack of autonomy or physical dependence on others, fatigue, depression, anxiety, communication difficulties, and lack of support. 3
The strong association between stress and physical well-being is well known in the literature, 4 as is the relationship between one's reactions to life stressors and the risk of developing some form of an autoimmune disease. 5 Research has found that one's vulnerability to stress has been found to be negatively related to QOL. 6 Furthermore, individuals who presented with several health conditions were found to report lower levels of QOL.7,8 Health conditions may play a role in increasing perceived stress levels and it is important to consider one's overall health when considering impacts on QOL. Cohen and colleagues 9 characterize perceived stress as the degree to which life situations are appraised as stressful, unpredictable, or overwhelming. MS widely varies in its clinical course and from patient to patient, and this unpredictability has been shown to increase levels of anxiety and decrease QOL in people with MS (PWMS). 10 Moreover, MS produces a variety of disabling and debilitating symptoms that are commonly exacerbated or worsened by stress among other factors.11,12
Individuals who encounter multiple stressors in their lives tend to be more likely to experience negative effects on their overall health. 13 Positive psychological traits such as gratitude may serve as a protective factor when confronted with difficult and challenging situations. Gratitude has been previously defined as a disposition or generalized tendency to recognize and demonstrate grateful emotions as well as positive life experiences and outcomes. 14 According to Emmons and Crumpler, 15 gratitude is an emotional state and attitude that can be a source of strength in enhancing one's well-being. Prior research has indicated that gratitude is negatively related to perceived stress and positively associated with better well-being in both general and chronically ill samples.4,16–18 Furthermore, previous studies suggest that gratitude may also lead to lower levels of stress over time.19,20 However, while a breadth of research has been conducted on gratitude and QOL in the context of other chronic illnesses, there have been mixed results regarding gratitude's relationship with QOL in MS. In an earlier study, Büssing and researchers 21 investigated experiences of awe, beauty in life, and gratitude in PWMS. Findings suggested low levels of reported gratitude; however, it is important to note that the study utilized unstandardized and unvalidated measures of gratitude, potentially influencing and limiting the generalizability of the results. Most recently, trait gratitude was found to uniquely predict higher levels of QOL among people living with MS above and beyond additional factors such as cognitive dysfunction, fatigue, and depression, 22 suggesting a strong relationship may in fact be present within this specific population.
Attempts to understand the relationship between gratitude and aspects of QOL have been documented in the literature. In one study conducted by Hill and colleagues, 23 psychological health, health-related activities, and willingness to seek help for health worries were found to explain the relationship between gratitude and physical health. In another study conducted by Eaton et al, 24 higher levels of positive affect among people with chronic illness mediated the relationship between gratitude and QOL. Similarly, in a study conducted by Lin, 25 gratitude was found to indirectly predict well-being partially through self-esteem. However, there is no research to date focused on determining the potential mediating effect of perceived stress on gratitude and QOL in populations with chronic neurological diseases, such as MS. Instead, there has been only one study that found perceived stress to partially explain the relationship between gratitude and QOL among a healthy military sample 26 as well as the indirect role of perceived stress on gratitude and life satisfaction among PWMS. 27 Clarifying the relationships between gratitude, perceived stress, and QOL among MS patients would provide additional, valuable information to the present literature as well as inform future clinical interventions aimed at maintaining and enhancing an individual's QOL.
The present study aimed to: (1) determine whether gratitude, perceived stress, and various patient characteristics are associated with QOL in PWMS, (2) determine if gratitude and patient characteristics are associated with perceived stress, and (3) determine if perceived stress mediates the relationship between gratitude and QOL in PWMS. We hypothesized that dispositional gratitude and perceived stress would be associated with QOL variables, gratitude would be associated with perceived stress, and that perceived stress would mediate the relationship between dispositional gratitude and QOL variables.
Method
Procedure
The present study was a cross-sectional examination of PWMS from 7/7/2021 and 10/14/2021. This study was approved by the Institutional Review Board (IRB) of a large Midwestern academic medical health center.
Participants
For inclusion in the study, participants were required to be at least 18 years of age and have a diagnosis of MS as recorded in their electronic medical record. Participants were recruited via an electronic MyChart message which also served as a research information sheet with a link to the study surveys on REDCap, a secure, web-based application designed to collect and store research data. Participants received a $15 check as compensation for their participation and completion of the survey. Participants who were not formally diagnosed with MS, could not read or write in English, or did not have access to MyChart messaging were excluded from this study.
Measures
Demographics Information Form. All participants provided information regarding their MRN, age, gender, race/ethnicity, marital status, education status, and income.
Gratitude Questionnaire-6 (GQ-6). 14 The GQ-6 is a 6-item self-report questionnaire designed to assess individual differences in the proneness to experience gratitude in daily life. Participants are asked to rate items on a 7-point Likert scale (1 indicating Strongly Disagree, four indicating Neutral and seven indicating Strongly Agree). Following reverse scoring of 2 items, a total scale score is achieved by summing all items. Scores can range from 6 to 42, with the higher numbers indicating higher levels of dispositional gratitude. The GQ-6 demonstrates excellent psychometric properties (α = .82) and high internal consistency in previous literature.
Perceived Stress Scale (PSS).9,28 PSS is a 10-item global measure of perceived stress. The self-report questionnaire was developed to assess the extent to which individuals believe that life events within the last month are unpredictable, uncontrollable, or unexpected. Participants are asked to rate items on a 5-point Likert scale (0 indicating Never, 4 indicating Very Often). Following reverse scoring of 4 items, a total scale score is achieved by summing all items. Individual scores on the PSS can range from 0 to 40, with higher scores indicating higher levels of perceived stress. The PSS has demonstrated good reliability and convergent validity in MS populations. 29
Neuro-QoL Measurement System (Neuro-QoL). 30 QOL in Neurological Disorders (Neuro-QoL) is comprised of a set of self-report measures assessing health-related QOL among adults with different neurological disorders. To measure the physical, mental, and social effects of neurological conditions, the Neuro-QoL is made up of 14 item banks assessing domains pertaining to Upper Extremity Function (Fine Motor, Activities of Daily Living), Lower Extremity Function (Mobility), Fatigue, Sleep Disturbance, Depression, Anxiety, Stigma, Positive Affect & Well-Being, Emotional and Behavioral Dyscontrol, End of Life Concerns, Cognitive Functioning, Communication, Satisfaction with Social Roles and Activities, and Ability to Participate in Social Roles and Activities. For the purposes of the present study, only item banks assessing Depression, Positive Affect & Well-being, Satisfaction with Social Roles and Activities, and Ability to Participate in Social Roles and Activities will be included to assess QoL in MS patients. Neuro-QoL measures have demonstrated good internal consistency, test re-test reliability, and concurrent validity in MS populations. 31
Statistical Analyses
An a priori sample size calculation was conducted with 11 predictors at a significance level of 0.05, power of 0.8 and medium effect size of 0.15 indicated that a sample size of 123 patients would be adequate for regression analyses. Descriptive statistics (eg, means, standard deviations, frequencies, percentages) for demographics (gender, age, race/ethnicity, marital status, income, and educational status) and scores on gratitude, PS, and QOL were computed for the entire cohort.
For Aim 1, factors predicting QOL variables (Neuro-QoL-Depression, Neuro-QoL-Positive Affect & Well-being, Neuro-QoL-Satisfaction with Social Roles and Activities, and Neuro-QoL-Ability to Participate in Social Roles and Activities) were evaluated through separate multivariable linear regression models. The T-score from each of the Neuro-QoL scales was the dependent variable for these models. For each of the four Neuro-QoL scales, separate models were fit where GQ-6 or PSS score was an independent variable. In all models, the following covariates were included: age, sex, race (White vs Black/Asian/Multiracial), marital status (married vs single/divorced/widow), education (Bachelor's/Graduate Degree vs high school degree/GED/Associate's Degree/Some College), and self-reported income ($0-$59,999, $60 000-$120,000, ≥ $120 000). Multicollinearity was checked using variance inflation factors (VIF), with VIF > 5 indicative of multicollinearity.
For Aim 2, we fit a multivariable linear regression model where PSS score was the dependent variable. GQ-6 score and the covariates mentioned above were included as independent variables.
For Aim 3, a series of multivariable linear regressions were conducted to evaluate mediation. Per Baron & Kenny, 32 the mediation analysis was conducted only when both gratitude and perceived stress were found to be significantly associated with QOL variables (Aim 1), and when gratitude was found to be significantly associated with PS (Aim 2). Multivariable linear regression analyses in which gratitude predicted Neuro-QoL variables, after controlling for PS were conducted. To see whether the mediation was significant, we used bootstrapping as proposed by Preacher & Hayes. 33 Bootstrapping for mediation analysis has been found to be more powerful than Sobel's test and is recommended in small samples. 33 Based on the bootstrap results, we reported the average causal mediation effect, average direct effect, total effect, and proportion mediated. Full mediation was supported when the average direct effect of gratitude on Neuro-QoL-Depression, Neuro-QoL-Positive Affect & Well-being, Neuro-QoL-Satisfaction with Social Roles and Activities, and Neuro-QoL-Ability to Participate in Social Roles and Activities was no longer significant following the addition of perceived stress. Partial mediation was supported when the average direct effect of gratitude on Neuro-QoL-Depression, Neuro-QoL-Positive Affect & Well-being, Neuro-QoL-Satisfaction with Social Roles and Activities, and Neuro-QoL-Ability to Participate in Social Roles and Activities was reduced but still statistically significant following addition of PS. Computations were performed in R, 34 version 4.1.0. Tests were two-sided and statistical significance was established throughout at P < .05.
Results
A total of 75 responses to the REDCap surveys were collected. Duplicate and incomplete questionnaires were excluded from analyses. The final sample consisted of 68 patients, average age was 47.8 years, (SD = 12.4). Approximately 75% identified as female and the majority of participants identified as White (85%). Approximately 63.2% reported they were single, 26.5% reported receiving a Bachelor's degree, and participants indicated a current median income of $65 000. Descriptive statistics for these 68 patients are shown in Table 1.
Descriptive statistics for patient sample.

Abbreviations: SD, standard deviation; IQR, interquartile range; GED, General Educational Development.
Table 2 shows the results of multivariable linear regression models for each of the four Neuro-QoL scales of interest. After adjusting for other covariates, each of GQ-6 score and PSS score were significantly associated with all four Neuro-QoL scale T-scores. For each one point increase in GQ-6 score, the Neuro-QoL depression T-score decreased by 0.78 points, on average. For each one point increase in PSS score, the Neuro-QoL depression T-score increased by 0.70 points, on average. Similar interpretations can be made for the other Neuro-QoL scales. After adjusting for PSS score and patient characteristics, males had significantly higher (worse) Neuro-QoL depression T-score (beta estimate = 3.16, P = .022) and lower (worse) Neuro-QoL positive affect/well-being T-score (beta estimate = −2.93, P = .038). This relationship was not observed in the models that included GQ-6 score as a covariate rather than PSS score. No other patient demographics were significantly associated with the Neuro-QoL T-scores.
Results of multivariable linear regression models where Neuro-QoL T-scores were dependent variables. For all 4 Neuro-QoL scales, the omnibus p-values for income were all greater than 0.10.

Abbreviations: CI, confidence interval; GED, General Educational Development; GQ-6, Gratitude Questionnaire -6; PSS, Perceived Stress Scale.
Table 3 shows the results of the multivariable linear regression model for PSS score. After adjusting for GQ-6 score and other patient demographics, males had PSS scores that were 5.93 points lower than females, on average (P = .004). GQ-6 score was independently associated with PSS score, such that for each one point increase in GQ-6 score, the PSS score decreased by 0.88 points, on average.
Results of multivariable linear regression model for PSS score.
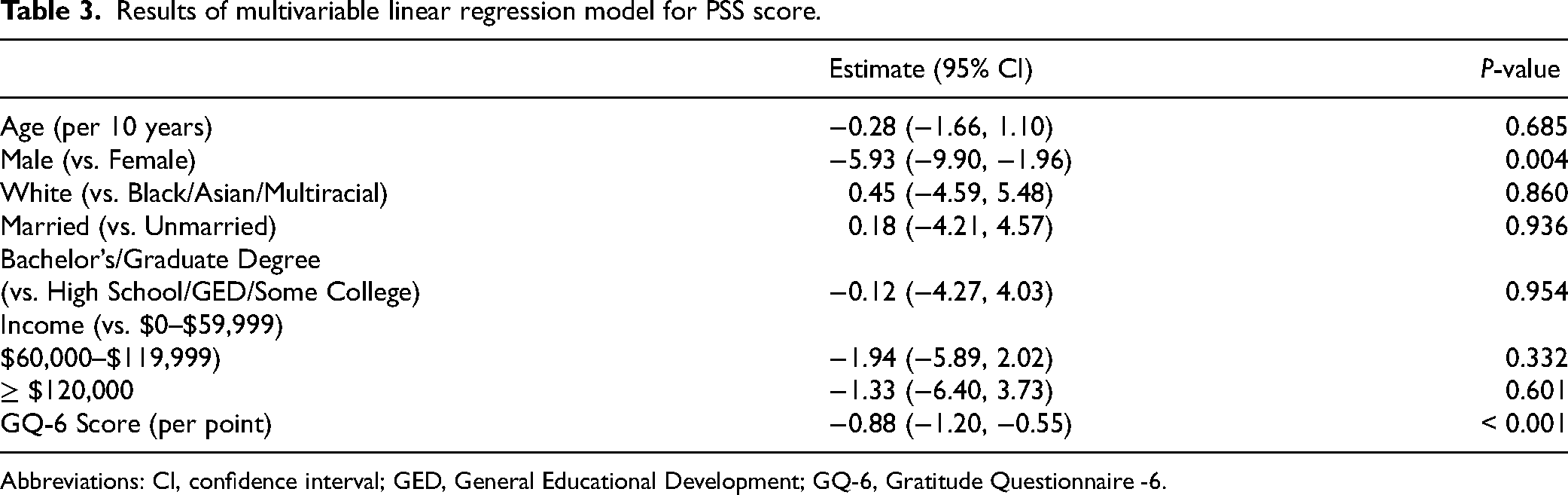
Abbreviations: CI, confidence interval; GED, General Educational Development; GQ-6, Gratitude Questionnaire -6.
Table 4 shows the results of the bootstrapped mediation analysis. The total effect represents the effect of GQ-6 score on each Neuro-QoL T-score, without adjustment for PSS score. The average direct effect represents the effect of GQ-6 score on each Neuro-QoL T-score, after adjusting for PSS score. Adding PSS score to the model changed the beta coefficient for GQ-6 score from −0.78 to −0.24 for depression, 0.80 to 0.24 for positive affect/well-being, 0.54 to 0.04 for satisfaction with social roles, and 0.66 to 0.15 for ability to participate in social roles. The average causal mediation effect represents the indirect effect of GQ-6 on each Neuro-QoL T-score through PSS score and is calculated as the difference between the total effect and average direct effect. In all models, the total effect and average causal mediation effect were significant. The average direct effect was statistically significant for positive affect/well-being, indicating a partial mediation, but was not significant for the other three scales, indicating full mediation. Thus, PS partially mediated the relationship between gratitude and positive affect/well-being and fully mediated the relationship between gratitude and depression, satisfaction with social roles, and ability to participate in social roles.
Results of mediation analysis using 10,000 bootstrap replications. The 95% confidence intervals were computed using the bootstrap percentile method.
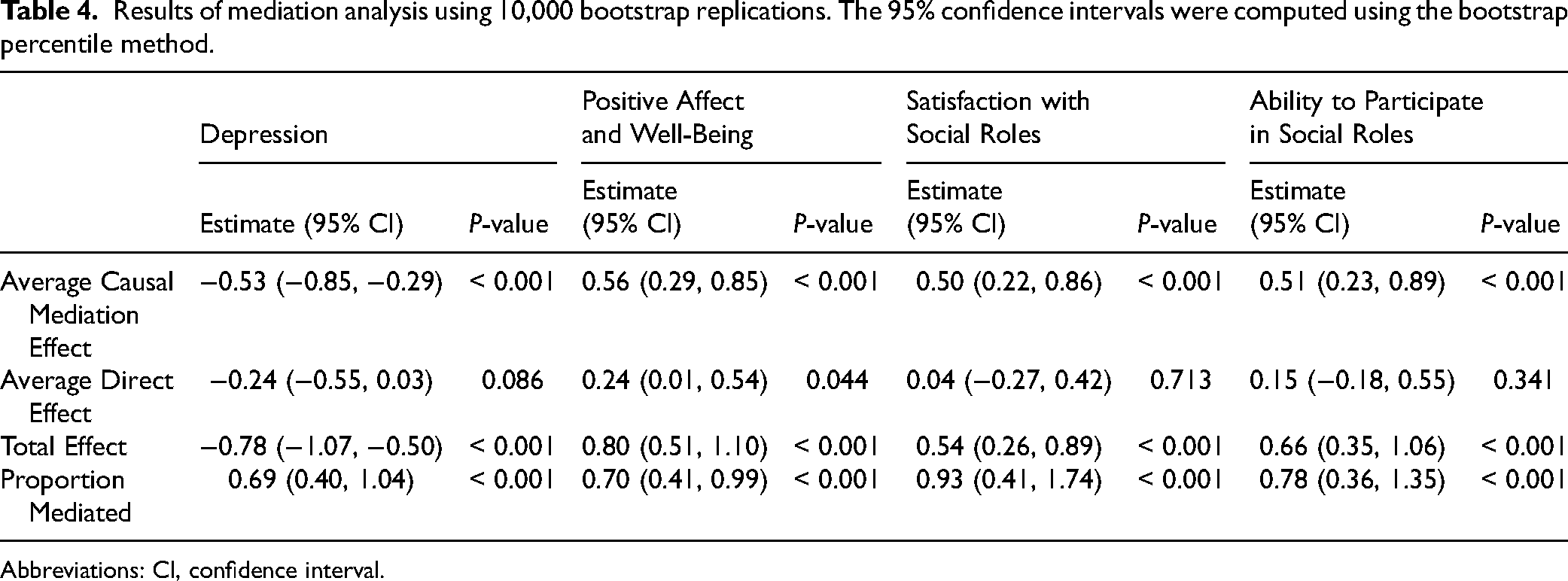
Abbreviations: CI, confidence interval.
Discussion
MS is a chronic, progressive disease of the central nervous system that is characterized by an unpredictable course of neurological symptoms that are exacerbated by stress and negatively impact QOL (QOL). 11 A strong association between stress and physical wellbeing is well known in the literature 4 and positive psychological traits such as gratitude have been found to be associated with decreased stress17–20 as well as increased well-being in both general and chronically ill samples.4,16–18 The results from the present study suggest higher levels of dispositional gratitude in PWMS are significantly associated with lower levels of PS and indirectly associated with improved QOL factors, which supports previous research findings. 17
Indeed, results of the present study indicated that the relationship between gratitude and QOL factors was both partially and fully mediated by PS, suggesting that one's perception of stressors may indirectly explain how practicing gratitude can influence QOL. Findings are consistent with studies conducted in non-chronically ill samples 26 and previous research determining the role of PS on life satisfaction in PWMS. 27 Similarly, recent research also indicates that trait gratitude predicts positive QOL in MS, above and beyond cognitive dysfunction, fatigue, or the presence of mental health symptoms, 22 suggesting that gratitude may also act as a direct and protective factor in maintaining well-being. This is important as PWMS have been shown to report lower levels of QOL compared to individuals diagnosed with other chronic illnesses. 10
McCullough et al 14 defined dispositional gratitude as a tendency to recognize the roles of other people's goodwill and compassion in positive experiences and outcomes with a sense of appreciation. Practicing gratitude can assist individuals in recognizing and acknowledging positive life experiences despite uncertain circumstances related to their health.14,21 This shift in perspective can lead to feeling less stressed or depressed16,18 and often can lead to motivating one to engage in prosocial behaviors such as practicing empathy or forming close, supportive relationships. 14 Clinicians may consider interventions incorporating the practice of gratitude (eg, naming and reflection of personal strengths, gratitude journaling, and conveying gratitude to others) as this may assist in reducing PS and subsequently promote QOL in PWMS. 16
Limitations
We acknowledge a number of limitations in the present study. First, while there are studies that have shown the effects of trait-based gratitude on factors associated with QOL, measurements of gratitude practice are required to establish more causal conclusions. This cross-sectional study was observational and therefore cannot determine cause-and-effect relationships. Future longitudinal research would be beneficial in examining patient characteristics and behaviors over time. Secondly, due to logistical and clinical constraints, recruitment was limited. The study was likely underpowered due to a small sample size, therefore, studies with larger sample sizes and broader recruitment strategies are needed to verify the results. Furthermore, our sample was restricted to patients who had access to our institution's electronic patient portal, MyChart, and this likely resulted in selection bias, with our sample appearing to be wealthier (median income $65 000) and with more education (44% with Bachelor's degree or higher). Finally, the scope of this study focused primarily on dispositional factors that may contribute to one's experience living with MS. However, it is important to note that both dispositional factors as well social determinants of health may intersect or interact to influence one's QOL. Future research would benefit from examining the role of perceived stress and gratitude on PWMS while also accounting for the wider public health environment.
Conclusions
The study presents several contributions to the current MS literature. Firstly, it is one of few examining the role of gratitude on QOL factors in PWMS. Secondly, results of this study may help future clinicians gain a better understanding regarding the role of dispositional factors as it relates to chronic disease adjustment and management and this may help to inform future interventions aimed at maintaining and enhancing an individual's QOL. PWMS who may be at risk for poor QOL may benefit from cognitive behavioral interventions that highlight strengths and the practice of gratitude in addition to stress management skills training.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
This study was approved by the Institutional Review Board of Cleveland Clinic, Cleveland, Ohio (21-358).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Statement of Human and Animal Rights
All procedures in the study were conducted in accordance with the Institutional Review Board of Cleveland Clinic, Cleveland, Ohio (21-358) approved protocols.
Statement of Informed Consent
Written informed consent was obtained from the patients for their anonymized information to be published in this article.